Isolated Proximal Ureteric Injury after a Penetrating Stab Wound to Lumbar Region
Manav Goyal1, G Sivasankar2, J Sivabalan3
1 Resident, Department of Urology, Government Royapettah Hospital, Chennai, Tamil Nadu, India.
2 Professor, Department of Urology, Government Royapettah Hospital, Chennai, Tamil Nadu, India.
3 Assistant Professor, Department of Urology, Government Royapettah Hospital, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manav Goyal, 19/40, B-Block, 6th Street, Anna Nagar East, Chennai, Tamil Nadu, India.
E-mail: docmanavgoyal@gmail.com
Urological injuries fall far behind other abdominal injuries when it comes to involvement during trauma. Amongst urological trauma, ureteral injuries account for 1-2.5%. An isolated ureteral injury is infrequently encountered because of a safe retroperitoneal location and a smaller diameter of the ureter as compared to other organs. A high index of suspicion is needed as a delayed or missed diagnosis of penetrating ureteral trauma or an unrecognised and mismanaged ureteral injury can lead to significant complications, including formation of urinoma, abscess, ureteral stricture or urinary fistula, and potential loss of the ipsilateral kidney. The present case report is of a 35-year-old male who presented to the Emergency Department of tertiary care hospital with a stab injury in left lumbar region and was diagnosed with isolated ureteral injury on Contrast Enhanced Computed Tomography (CECT). Without much delay, ureteroscopy was done, a double J stent was placed and ureteroureterostomy was performed.
Computed tomography, Ureteral injury, Ureteric repair
Case Report
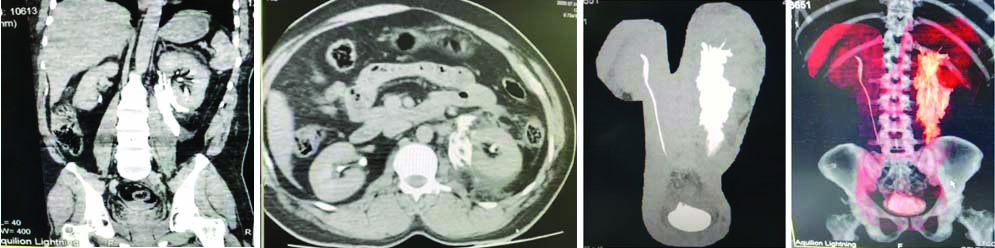
A 35-year-old male patient presented to our Emergency Department with an alleged history of a stab wound to the left lumbar region. He had persistent pain in the left lumbar region, but there was no history of anuria or haematuria on presentation. No other injury was noted. On examination his vitals were stable. Per abdomen examination revealed a laceration of 4×2 cm in the left lumbar region with a peritoneal breach. There was marked tenderness in the lumbar region, but no rigidity, guarding or abdominal distension. Complete blood counts and renal function tests were found to be within the normal range. A CECT abdomen and pelvis was performed which showed that contrast uptake was present in both the kidneys [Table/Fig-1]. An extravasation of the contrast was noted just adjacent to the left upper ureter extending into the perirenal space and left paracolic gutter. All other abdominal organs seemed uninvolved in the scan.
Computed Tomography (CT): Contrast extravasation noted adjacent to left upper ureter extending into the perirenal space and left paracolic gutter (showed in coronal, axial and 3D images).
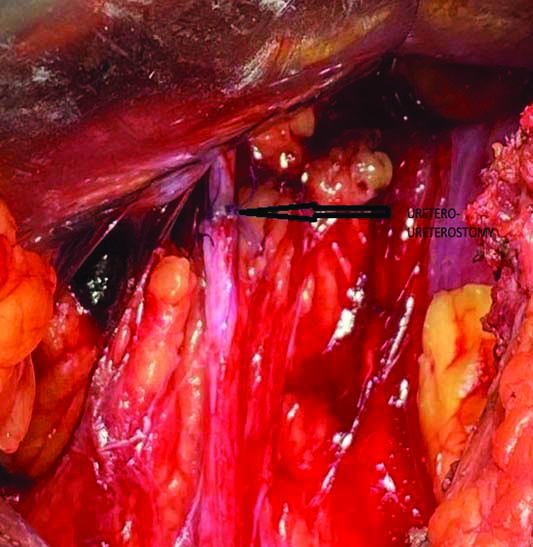
A left-sided ureteroscopy was performed, which revealed that 3/4th circumference of the proximal ureter was transected. A paracolic haematoma was present but with no significant intraperitoneal organ injury. A double J stent was placed across the transected left ureter and left open ureteroureterostomy was performed [Table/Fig-2,3]. The patient had an uneventful postoperative course and showed significant recovery during his hospital stay. The retroperitoneal drain was removed on the 4th day and the patient was discharged from hospital on the 10th postoperative day. Patient was followed-up after four weeks and DJ stent was removed. On repeat contrast study, both uptake and excretion were noted from the left kidney.
Transected 3/4th of the proximal ureter with Double J stent in-situ.

Water tight ureteroureterostomy using 4-0 vicryl.
Discussion
Amongst all penetrating trauma to abdomen, ureteral injuries account for just 1-2.5% [1]. Ureteral injuries following abdominal stab wounds are rare and difficult to diagnose [1]. Isolated ureteral injury is rare because of small diameter of ureter and it’s protective retroperitoneal location. A delayed and missed diagnosis of penetrating ureteral trauma is often associated with impairing morbidity, increased nephrectomy rates and prolonged hospital stay [2]. More than 90% of patients with ureteral injuries have a concurrent abdominal or retroperitoneal organ injury [3]. Significant ureteral injury can occur in the absence of any sign or symptom, so it is difficult to anticipate and diagnose [4]. Haematuria is a non-specific indicator of ureteric injury [4]. An unrecognised or mismanaged ureteral injury can lead to significant complications, including formation of urinoma, abscess, ureteral stricture or urinary fistula, and potential loss of the ipsilateral kidney.
CT urography is the best diagnostic modality for detecting ureteral injury [5]. The CT findings that indicate ureteral injuries include presence of contrast extravasation from the ureter, non-visualisation of the ureter, ipsilateral hydronephrosis, and poor renal excretion localised to one side [6]. So, CT can be extremely helpful to diagnose ureteral injury especially in haemodynamically stable patients as in present case. The American Urological Association (AUA) trauma guidelines recommend performing abdominopelvic CT with intravenous contrast and delayed scans for all stable patients with suspected ureteral trauma [7]. The primary goal of a ureteral repair is to maintain renal drainage [8]. Management options depend on the site of injury, extent of the devitalised ureter, and other concomitant injuries. The basic surgical principles include a tension free anastomosis, debridement of devitalised tissues, spatulation of each end, and securing a water tight anastomosis [9]. In this case, there was a partial transection of the proximal ureter, so ureteroureterostomy was performed after placing double J stent. Early ureteric injury can be managed with a Double J stent, ureteroureterostomy, ureteroneocystostomy with a psoas hitch and external diversion depending upon the grade of ureteric injury [10]. Delayed recognition of ureteric injury is found to have a poor prognosis with a higher incidence of nephrectomy when compared with those patients who receive immediate treatment [11].
Failure to make a prompt diagnosis can further lead to several complications, including formation of urinomas, periureteral abscess, fistula and strictures which are readily preventable with proper stenting and timely placement of nephrostomy tube [12]. In cases with complete ureteral damage, surgical options of appendiceal interposition and ileal segment interposition have been well documented [13,14].
Conclusion(s)
Ureteral injuries are relatively rare, and more common in penetrating injuries than in blunt injuries. A delayed diagnosis or missed diagnosis can be associated with a high level of morbidity and mortality. CT urography is the best imaging modality for diagnosing ureteral injury in an emergency setting. Immediate and meticulous repair remains the cornerstone for preservation of renal function and preventing life threatening complications.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 09, 2020
Manual Googling: Feb 11, 2021
iThenticate Software: Mar 22, 2021 (20%)
[1]. Siram SM, Gerald SZ, Greene WR, Hughes K, Oyetunji TA, Chrouser K, Ureteral trauma: Patterns and mechanisms of injury of an uncommon conditionAm J Surg 2010 199:566-70.10.1016/j.amjsurg.2009.11.00120359576 [Google Scholar] [CrossRef] [PubMed]
[2]. Kunkle DA, Kansas BT, Pathak A, Goldberg AJ, Mydlo JH, Delayed diagnosis of traumatic ureteral injuriesJ Urol 2006 176:2503-07.10.1016/j.juro.2006.08.00317085143 [Google Scholar] [CrossRef] [PubMed]
[3]. Pereira BM, Ogilvie MP, Gomez-Rodriguez JC, Ryan ML, Pena D, Marttos AC, A review of ureteral injuries after external traumaScand J Trauma Resusc Emerg Med 2010 18:610.1186/1757-7241-18-620128905 [Google Scholar] [CrossRef] [PubMed]
[4]. Elliott SP, McAninch JW, Ureteral injuries: External and iatrogenicUrol Clin North Am 2006 33:5510.1016/j.ucl.2005.11.00516488280 [Google Scholar] [CrossRef] [PubMed]
[5]. Kawashima A, Sandler CM, Corl FM, West OC, Tamm EP, Fishman EK, Imaging of renal trauma: A comprehensive reviewRadiographics 2001 21:557-74.10.1148/radiographics.21.3.g01ma1155711353106 [Google Scholar] [CrossRef] [PubMed]
[6]. Gayer G, Zissin R, Apter S, Garniek A, Ramon J, Kots E, Urinomas caused by ureteral injuries: CT appearanceAbdom Imaging 2002 27:88-92.10.1007/s00261-001-0052-511740616 [Google Scholar] [CrossRef] [PubMed]
[7]. Morey AF, Brandes S, Dugi DD 3rd, Armstrong JH, Breyer BN, Broghammer JA, Urotrauma: AUA guidelineJ Urol 2014 192:327-35.10.1016/j.juro.2014.05.00424857651 [Google Scholar] [CrossRef] [PubMed]
[8]. Brandes S, Coburn M, Armenakas N, McAninch J, Diagnosis and management of ureteric injury: An evidence-based analysisBJU Int 2004 94:277-89.10.1111/j.1464-410X.2004.04978.x15291852 [Google Scholar] [CrossRef] [PubMed]
[9]. Park SH, Kim KH, Isolated ureteral injury following a stab wound: A case reportTrauma Case Reports 2019 21:10019710.1016/j.tcr.2019.10019731011616 [Google Scholar] [CrossRef] [PubMed]
[10]. Best CD, Petrone P, Buscarini M, Demiray S, Kuncir E, Kimbrell B, Traumatic ureteral injuries: A single institution experience validating the American Association for the Surgery of Trauma-Organ Injury Scale grading scaleJ Urol 2005 173(4):1202-05.10.1097/01.ju.0000155526.37963.ef15758748 [Google Scholar] [CrossRef] [PubMed]
[11]. McGinty DM, Mendez R, Traumatic ureteral injuries with delayed recognitionUrology 1977 10(2):115-17.10.1016/0090-4295(77)90007-3 [Google Scholar] [CrossRef]
[12]. Tezval H, Tezval M, von Klot C, Herrmann TR, Dresing K, Jonas U, Urinary tract injuries in patients with multiple traumaWorld J Urol 2007 25:177-84.10.1007/s00345-007-0154-y17351781 [Google Scholar] [CrossRef] [PubMed]
[13]. Dagash H, Sen S, Chacko J, Karl S, Ghosh D, Parag P, The appendix as ureteral substitute: A report of 10 casesJ Pediatr Urol 2008 4:14-19.10.1016/j.jpurol.2007.08.00418631886 [Google Scholar] [CrossRef] [PubMed]
[14]. Kochakarn W, Tirapanich W, Kositchaiwat S, Ileal interposition for the treatment of a long gap ureteral lossJ Med Assoc Thai 2000 83:37-41. [Google Scholar]