Metabolic syndrome is a well-known disease of multiple risk factors that has at its core secondary to insulin resistance that accompanies abnormal deposition and function of adipose tissues in the body. It is a risk factor for multiple lifestyle diseases like coronary artery disease, fatty liver, diabetes and several cancers [1,2]. As per guidelines of the National Heart, Lung, and Blood Institute (NHLBI) and the American Heart Association (AHA), diagnosis of metabolic syndrome is established when atleast three of five abnormal criteria related to fasting blood glucose level, blood pressure, serum triglyceride and High-density Lipoprotein (HDL) level and waist circumference are met [3].
Multiple studies demonstrate a potential relationship between VFT and metabolic syndrome, more so in fact, than with Body Mass Index (BMI) or the amount of subcutaneous fat [4-6]. Recent articles emphasise the use of Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) to quantify visceral and sub-cutaneous fat [7-9]. The role of the ubiquitous ultrasonography has largely been documented to demonstrate hepatic steatosis and fatty accumulation around the visceral organs [10,11]. The role of Ultrasound in providing visceral fat quantification is comparable to the gold standard modality such as Computed Tomography (CT) scan in predicting metabolic syndrome [12]. Such studies are generally few with no documented cut off values which may provide an objective guideline to possible Metabolic syndrome. Hence, this study aimed to correlate the relationship between VFT measurement on ultrasound and with the risk of metabolic syndrome.
Materials and Methods
This cross-sectional study was carried out at a tertiary care hospital during the period of August 2016 to August 2019. Informed consent was obtained from each patient included in the study. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the Institutional Ethics Committee (08/27/IEC/CHWC/2014).
Inclusion criteria: All patients who underwent ultrasound at the study centre between August 2016 to August 2019 and were clinically suspected of metabolic syndrome at the Endocrinology OPD by fulfilling any of the following criteria:
Blood pressure value ≥130/85 mmHg (or receiving drug therapy for hypertension).
Waist circumference in men ≥90 cm or in women ≥80 cm.
Exclusion criteria: Patients with chronic diseases like cirrhosis, lymphoma or renal failure and those with history of bariatric or aesthetic surgery were excluded from the study.
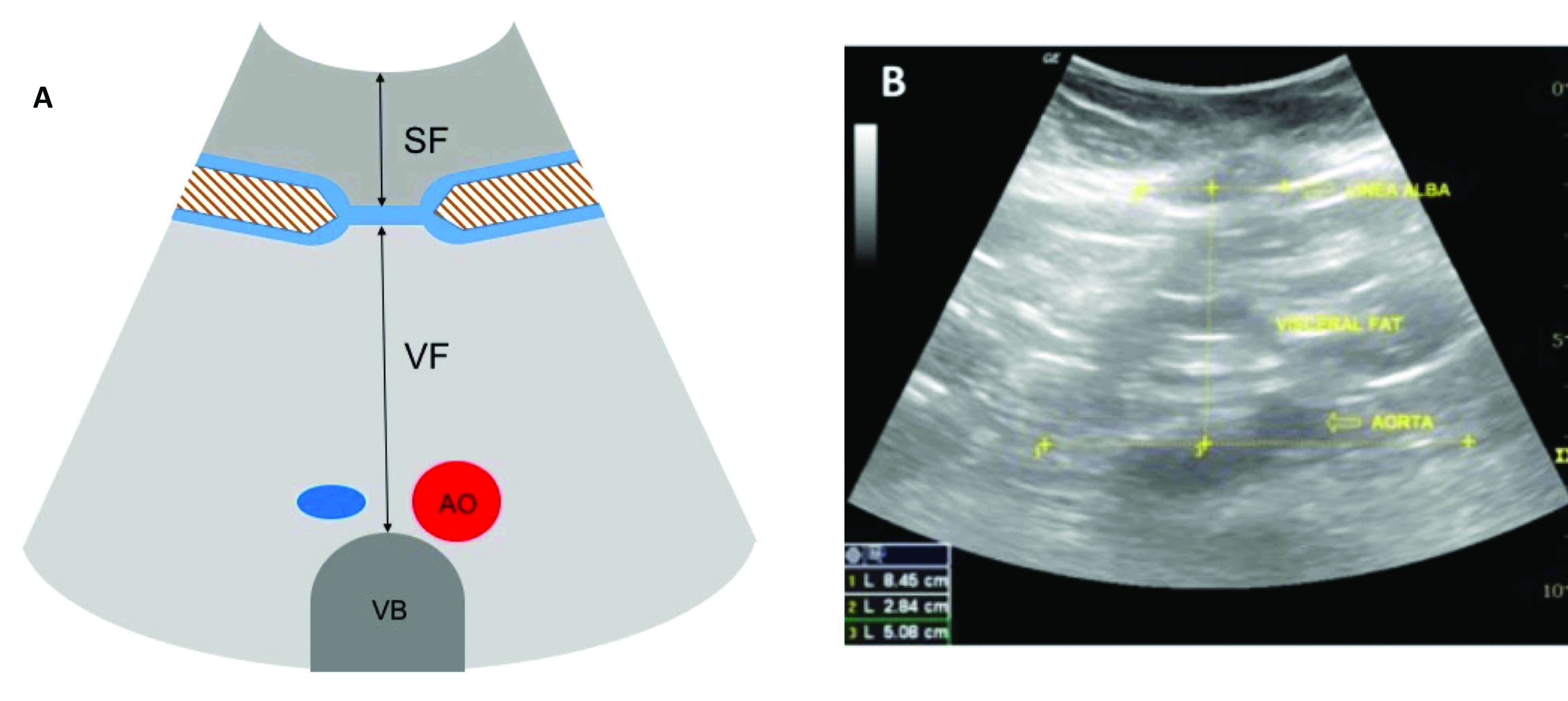
All scans were performed on a single Logiq P5 ultrasound system (GE, USA), using a 2.5 to 5 MHz multifrequency convex transducer. The ultrasound scan was performed with the patient in dorsal decubitus position and measurements of subcutaneous and VFT were performed. A convex 3.5-5 MHz transducer was placed on the midline in the transverse plane, 1 cm above the umbilical scar, during the expiratory phase, without applying pressure on the abdomen. Subcutaneous fat thickness was measured as the distance (in centimeters) between the skin and the anterior surface of the linea alba. VFT was measured as the distance (in centimeters) between the posterior surface of the linea alba and the plane of the posterior aortic wall [Table/Fig-1].
Subcutaneous and Visceral Fat Thickness (VFT) measurement.
SF: Subcutaneous fat; VF: Visceral fat; AO: Aortic wall
Two radiologists (DY and AR) with 15 and 19 years of respective experience in sonology performed the ultrasound scans in all patients. Initially, 50 patients were scanned by both radiologists separately and blinded to each other’s findings. Interobserver variability was determined, if a variability of more than 5% between the measurements obtained by the two radiologists were noted. Subsequently, the rest of the patients were scanned independently by either of the two radiologists (DY or AR) and the results pooled into a common result sheet.
The patient data was distributed into three categories based on the VFT as follows [12]:
Category 1: VFT <7 cm
Category 2: VFT of 7 cm to 10 cm
Category 3: VFT >10 cm
Collation of data in these categories was done on the basis of tertiles in the Receiver Operating Characteristic (ROC) curves. The patients in each category underwent further testing for blood glucose and lipid profiles and metabolic syndrome was either ruled out or diagnosed in these patients according to the criteria listed above.
Statistical Analysis
Calculation of sensitivity, specificity, PPV and NPV was done in each of the groups to determine the usefulness of VFT in predicting the risk for developing metabolic syndrome. The data was collected on Microsoft Excel (2019 version) and Statistical analysis was performed using STATA version 15.1. Positive and NPV for different cut-off levels of VFT were calculated to predict metabolic syndrome.
Results
A total of 2254 patients fulfilling the inclusion criteria underwent ultrasound examinations at the study centre between August 2016 and August 2019. Of these, 232 patients suffered from chronic disease or had undergone prior surgery (falling in the exclusion criteria) and were excluded from the study forming a cohort of 2022 patients.
The mean age of patients was 55.2±13.3 years. Male patients formed 48.28% (n=976) of the cohort while female patients were 51.72% (n=1046). There was 100% inter-observer correlation (Interobserver variability of <5%) in the scans performed on the initial 50 patients by both radiologists.
The VFT ranged between 4 cm to 16 cm with a mean value of 10.8 cm and standard deviation of 2.8. Males showed higher VF with a visceral to subcutaneous fat (V/S) ratio of 4.56 as opposed to 3.46 in females.
The number of VFT patients in the different categories with metabolic syndrome are detailed in [Table/Fig-2]. Highest number of metabolic syndrome was noted in patients with VFT >10 cm.
Results of Visceral Fat Thickness (VFT) and subjects with metabolic syndrome in the study population.
| VFT thickness | Number (%) (N=2022) | Number (%) detected with metabolic syndrome (N-1264) |
|---|
| >10 cm | 1071 (53%) | 999 (93.3%) |
| 7 cm-10 cm | 627 (31%) | 244 (38.9%) |
| <7 cm | 324 (16%) | 21 (6.5%) |
[Table/Fig-3] summarises the specificity/sensitivity and predictive values for predicting metabolic syndrome. VFT greater than 10 cm was found to have high specificity and PPV while VFT less than 7 cm was found to have high NPV. VFT values between 7 to 10 were found to be poorly predictive of either confirming or ruling out metabolic syndrome.
Table showing sensitivity, specificity, PPV and NPV of different cut-off values for Visceral Fat Thickness (VFT).
| VFT | Sensitivity | Specificity | PPV | NPV |
|---|
| <7 cm | 95.11 | 19.5 | 1.6 | 95.10 |
| 7-10 cm | 92.1 | 27.7 | 19.6 | 94.7 |
| >10 cm | 79 | 92.52 | 92.53 | 21.3 |
PPV: Positive predictive value; NPV: Negative predictive value
No significant correlation was found between V/S ratio and metabolic syndrome. No definitive cut-off value for V/S ratio that could predict the risk for developing metabolic syndrome could be determined.
Discussion
Abdominal obesity has been traditionally considered to be one of the most important modifiable risk factor for metabolic syndrome, but the importance of compartmental distribution of this fat has recently come to focus with visceral fat considered to be the hormonally active component and therefore more significant contributor to development of metabolic syndrome. This study highlights the importance of sonographic measurement of VFT as a simple, inexpensive and easily reproducible tool in predicting metabolic syndrome. In a recent study done on Japanese Americans, it was found that visceral fat deposition is a predictor of future insulin resistance [3]. The Framingham Heart Study also supports similar findings and hypothesis that visceral fat is more strongly associated with an adverse metabolic risk profile [5]. Anjana M et al., had earlier reported that in Asian Indians, it was visceral fat rather than subcutaneous abdominal fat that was associated with type 2 diabetes [13].
Two hypothesis have been proposed for a strong association of visceral fat with metabolic syndrome in absence of knowledge of the exact molecular mechanisms. One of these being the direct drainage of metabolites and free fatty acids into the liver due to anatomical proximity of visceral fat to portal vein, leading to hepatic insulin resistance which can cause increased hepatic gluconeogenesis [14]. The other hypothesis states that the increased lipolytic nature of visceral adipocytes could lead to harmful visceral fat deposition compared to the subcutaneous abdominal deposition. Porter SA et al., have raised a possibility of protective value of subcutaneous fat [15]. Since almost the past two and a half decades, CT has been considered as the gold standard method to quantify abdominal adiposity [16]. According to Després JP and Lamarche B, a lower limit of 130 cm2 for visceral fat area was found to be associated with a relatively higher risk of cardiovascular events [17].
Even though, BMI is the most common method used for estimating body fat, but an increase in BMI does not occur if the fat or lean mass compartment is deficient. Furthermore, it does not differentiate subcutaneous from visceral fat accumulation. An estimate of body fat can be made by measuring skin fold thickness and few skin fold ratios can be used to measure fat distribution [18]. Measurement of waist circumference has been used in few studies due to ease of use, low cost, and accuracy [19]. Bioelectrical Impedance Analysis (BIA) has also been used proposed as a specialised technique for the assessment of adipose tissue distribution, to quantify the percentage of lean and fat mass [20].
Armellini F et al., initially proposed the use of ultrasound in assessment of intra-abdominal fat [21]. Utility of ultrasound for assessment of visceral fat was further confirmed by strong correlations with the CT-determined visceral fat area by Suzuki R et al., [22]. In a study by Ribeiro-Filho FF et al., visceral distance as determined by ultrasound was also shown to correlate strongly with CT measurements [23]. According to their study, this coefficient was the best among all the methods investigated. Eifler RV, found correlation of VFT measured on ultrasound with hepatic steatosis, a well known entity in Metabolic Syndrome [12].
Ultrasound may be the most specific method for visualisation of subcutaneous and visceral fat. Additionally, ultrasound has added advantage of being noninvasive and quick with good reliability as well as lack of radiation exposure and lower costs than CT scans. Drawbacks to this method are requirement of specific equipment and a well-trained examiner. Furthermore, the number of subjects with VFT and metabolic syndrome in Category 1 was higher than in Category 3. In addition, this study suggested that a VFT of >10 cm was a cut-off for predicting the presence of metabolic syndrome. These cutoff values for VFT were shown to have high specificity and PPV for metabolic syndrome. Therefore, the ultrasonographic measurement of VFT might be a good method of predicting metabolic syndrome and evaluating the consequent risk of Cardiovascular Disease (CVD) without the limitations of anthropometric indexes.
Limitation(s)
The study had a few limitations: Firstly, being an observational, cross-sectional study, no cause/effect inferences can be drawn. Secondly, as the study only included patients with metabolic syndrome, the conclusions of present study cannot be automatically extended to the general population. Furthermore, the measurements were not grouped into different age and sex-based categories. The authors propose that future studies should have control groups and these be further sub-divided into different age and gender groups.
Conclusion(s)
Ultrasound seems to be the best screening tool for the assessment of intra-abdominal fat deposition in patients at risk of metabolic syndrome. Its diagnostic value could be maximised by the cut-off of VFT >10 cm.
PPV: Positive predictive value; NPV: Negative predictive value