A Rare Case of Hypothenar Hammer Syndrome Triggering Guyon’s Canal Syndrome
Guruprasad Rai1, Ganesh Sevagur Kamath2, Vaishnavi Kavirayani3, Arvind Kumar Bishnoi4, Revanth Reddy5
1 Associate Professor, Department of Cardiovascular Thoracic Surgery, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
2 Professor, Department of Cardiovascular Thoracic Surgery, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
3 MBBS Student, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
4 Professor, Department of Cardiovascular Thoracic Surgery, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
5 Associate Professor, Department of Cardiovascular Thoracic Surgery, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Ms. Vaishnavi Kavirayani, 101, Uma Sanjivini Residency, 1st Main Road, Lakshmi Nagar, JP Nagar, 7th Phase, Bangalore, Karnataka, India.
E-mail: vaishnavi.kavirayani@learner.manipal.edu
In certain occupations, injuries and microtrauma are commonly encountered by the soft tissues of the hand in the adult population, which may, however, less frequently lead to arterial occlusion. One such example is that of the Hypothenar Hammer Syndrome (HHS). It is a rare traumatic disease of the hand, caused by blunt traumas to the heel of the hand that may damage the ulnar artery at the level of hypothenar eminence. This results in occlusion or aneurysm of the vessel. It is of clinical importance due to the risk of loss of limb function following digital ischemia. The ulnar nerve barely gets compressed in the Guyon’s canal, which may in turn cause Guyon’s canal syndrome. This is a case of a 43-year-old male patient who presented with painful swelling of the right hand, which was diagnosed as a bizarre presentation of a bilobed and partially thrombosed pseudoaneurysm of the ulnar artery producing Guyon’s canal syndrome that had to be surgically excised. The objective of this case is to highlight the clinical presentation of HHS for early diagnosis and treatment.
Bilobed pseudoaneurysm, Ulnar artery, Ulnar nerve
Case Report
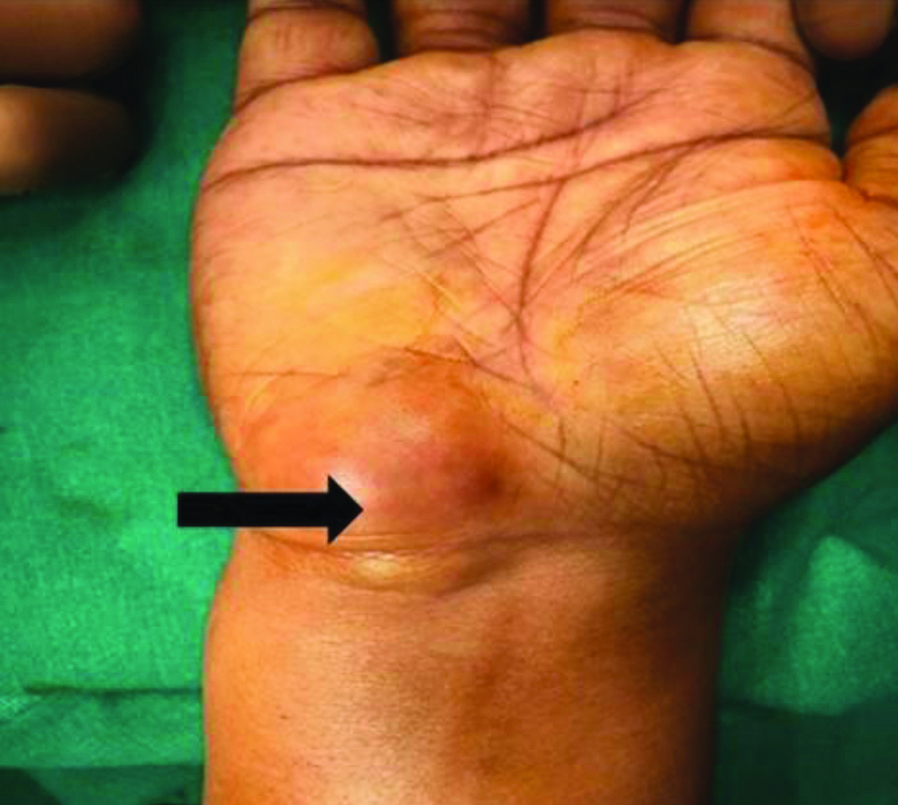
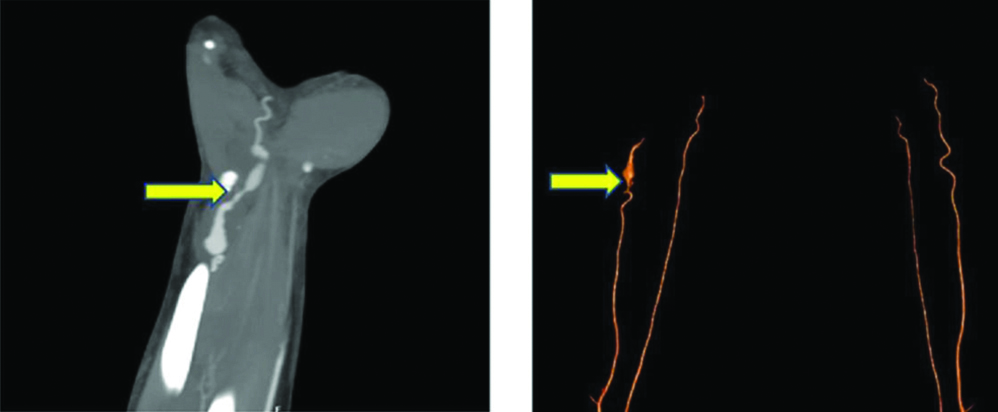
A 43-year-old male bank employee who has to spend long hours on the computer presented with painful swelling in the right hand with a duration of five years. The swelling was insidious in onset, progressive, initially, the pain was noted on the movement of hand at the wrist, no discoloration of hand/fingers. For the last six months, pain and swelling increased around the hypothenar eminence, with reduced mobility, tingling, and paraesthesia over the little and ring fingers of the right hand [Table/Fig-1]. No similar complaints were noticed on the opposite hand. On local examination, the swelling was present in the right wrist over the hypothenar eminence with mild tenderness. It was pulsatile in nature, no local rise of temperature, non-fluctuant, soft to firm. Sensory examination revealed diminished sensation over the little finger and the ulnar half of the ring finger on their volar surfaces and there was no motor weakness. In nerve conduction studies, electromyogram was performed to diagnose if there were any neuromuscular diseases, motor problems, nerve injuries, or degenerative conditions. As swelling was pulsatile, a likely diagnosis of pseudoaneurysm was made and the patient underwent Computed Tomography (CT) Angiogram. CT Angiogram revealed proximal ulnar artery was normal in caliber and contrast opacification. However, the distal ulnar artery was tortuous in the course and showed two fusiform dilatations, proximal partially thrombosed aneurysm measuring 3.3×1.9×2.3 cm (with patent lumen measuring 7×95×22 mm) noted in the distal third of the forearm, and distal partially thrombosed aneurysm measuring 3.2×1.7×1.6 cm (with patent lumen measuring 8×8×21 mm) noted at the level of hypothenar muscles. This aneurysm was seen to compress on the ulnar nerve distally. The radial artery flow was normal and supplying both superficial and deep palmar arches [Table/Fig-2].
Swelling in the right hand, near the hypothenar eminence.
Computed tomography angiogram shows bilobed, partially thrombosed aneurysms.
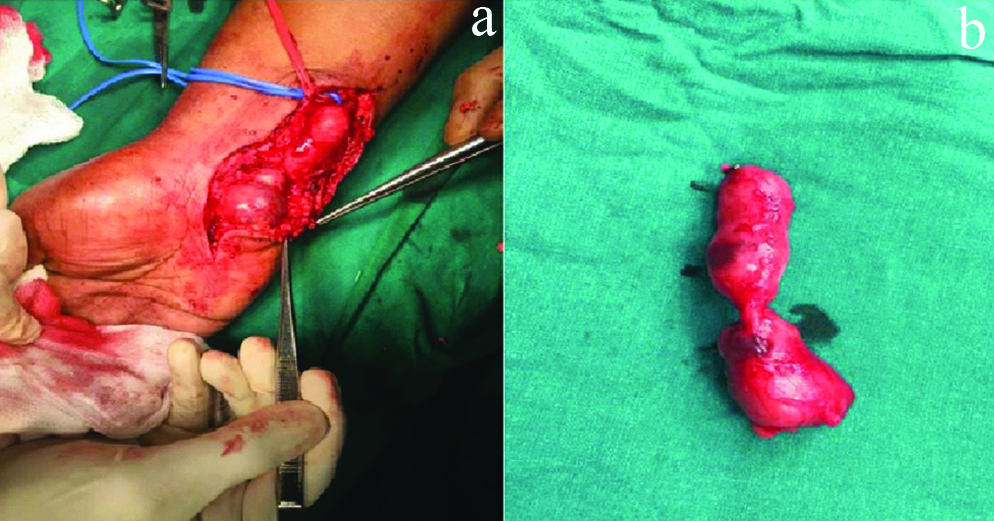
To relieve symptoms of neuropathic pain, the patient was taken up for surgical exploration under the brachial block with excision of aneurysm and ligation of ulnar artery just proximal to the bifurcation of ulnar artery to the palmar arches. As collateral flow was sufficient from the radial artery, ligation was adequate [Table/Fig-3]. Postoperatively, symptoms were relieved and vascular supply of the hand was normal.
Intraoperative pictures showing: (a) dissection and (b) enucleated specimen.
One month follow-up was done and the patient showed symptomatic improvement. His sensory and motor symptoms decreased. Postoperative recovery was uneventful and the patient was diagnosed with HHS (Right ulnar artery pseudoaneurysm) causing Guyon’s canal syndrome.
Discussion
Hypothenar hammer syndrome is a rare traumatic disease of the hand, due to repetitive injury to the ulnar artery. It was first described by Von Rosen (1934) [1]. There are intimal and medial wall degeneration and thrombosis caused by the repeated trauma to the ulnar artery, with or without aneurysm, and subsequent embolic occlusion of the digital arteries, resulting in symptomatic ischemia [2]. It is commonly seen in manual labour with continued vibratory stimuli, automated coercion, and repetitive trauma to the hand. In present case, the aetiology was presumed to be repetitive pressure on the hypothenar eminence due to continuous use of the mouse for computer work.
The ulnar artery is vulnerable to mechanical injury because of its anatomical placement. Guyon’s canal is a fibro-osseous tunnel within the ulnar aspect of the wrist [3]. This tunnel was named after Felix Guyon French surgeon in 1861 [4]. It is defined radially by the hamate, roof by the volar carpal ligament, floor by the transverse carpal ligament, and ulnarly by the pisiform and the flexor carpi ulnaris [5]. The ulnar neurovascular bundle enters the hand through Guyon’s canal below the palmar fascia and runs through to form palmar arches. In Guyon’s canal, the ulnar artery is above the hook of hamate bone, and repetitive blunt trauma at this point, damages the ulnar artery, leading to thrombosis and ischemia of the digits. Aneurysm formation compresses the ulnar nerve in this enclosed space and leads to Guyon’s canal syndrome [6].
Guyon canal syndrome is a comparatively uncommon peripheral ulnar neuropathy that is associated with entrapment of the distal portion of the ulnar nerve as it travels through the Guyon’s canal at the wrist. Patients’ usual presentation may be associated with pure sensory disturbance, pure motor disturbance, or a combination of both depending on the level of entrapment. The symptoms being paresthesia to the 4th and 5th fingers along with the lateral part of the palm and painful hypothenar eminence. The severity of symptoms depends on where the obstruction is located [7].
Shea JD and McClain EJ were the first to have reported Guyon’s canal lesions into three types: Type I-proximal lesions having both sensory and motor involvement (30%), Type II-lesions causing weakness of the intrinsic muscles (52%), and Type III-distal lesions causing only sensory abnormalities (18%) [8]. The present case is Type III according to Shea and McClain’s classification.
In this case, a traumatic ulnar artery pseudoaneurysm causing an acute ulnar nerve compression at the Guyon’s canal with pure sensory disturbance is quite rare. The rarity of the HHS triggering Guyon’s canal syndrome generally leads to a delayed diagnosis because the syndrome may go undetected due to flow compensation through the radial artery and is probably underestimated in hand workers. The therapeutic approach of this syndrome is strictly correlated to its symptoms, starting from a simple oral antiplatelet aggregation therapy to surgical excision of the affected vessel and its reconstruction with a bypass [9]. Patients with severe ischemic symptoms and entrapment of the nerve require surgical excision. In the presence of doubtful collateral circulation, revascularisation with a venous graft (generally taken from a saphenous vein) is essential.
With as little as 150 reported cases of HHS, ulnar artery aneurysm occurrence is not frequent [10]. The prevalence of this condition is estimated at 14% in the population at risk (manual labourers and hand workers) [11]. In contrast, the incidence of this condition in the patients who present with hand vascular problem is only 1.1-1.6% (from a study conducted on Industrial population in Australia) [11] and its prevalence with Guyon’s canal syndrome in the general population have not yet been precisely estimated due to the lack of studies [12,13].
Conclusion(s)
Hypothenar hammer syndrome with a bilobed aneurysm leading to Guyon’s canal syndrome is a very rare presentation. In present case, a bilobed aneurysm grew into Guyon’s canal compressing the ulnar nerve. It is a preventable and curable cause of digital ischemia or neuropathy of the upper extremity. However, its diagnosis is frequently delayed often leading to permanent disability. Most of the time, symptoms are non-specific, do not show clearly, and go undetected in the preclinical stage. Hence regular screening must be undertaken among the occupational population in involved industries, to prevent disability.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 28, 2020
Manual Googling: Jan 09, 2021
iThenticate Software: Jan 27, 2021 (15%)
[1]. Von Rosen S, Ein Fall Von Thrombose in der Arteria Ulnaris nach Einwirkung von Stumper GewaltACTA Chir Scand 1934 73:500-06. [Google Scholar]
[2]. Ablett CT, Hackett LA, Hypothenar hammer syndrome: Case reports and brief reviewClin Med Res 2008 6(1):03-08.10.3121/cmr.2008.77518591371 [Google Scholar] [CrossRef] [PubMed]
[3]. Guyon F, Note on the anatomical arrangement of the anterior surface of wrist, not previously describedBull Soc Anat Paris 1861 6:184-86. [Google Scholar]
[4]. Guyon F, Note on the anatomical condition affecting the underside of the wrist not previously reportedJ Hand Surg Br 2006 31(2):147-48.10.1016/J.JHSB.2005.12.00816442675 [Google Scholar] [CrossRef] [PubMed]
[5]. Gross MS, Gelberman RH, The anatomy of the distal ulnar tunnelClin Orthop Relat Res 1985 (196):238-47.10.1097/00003086-198506000-00033 [Google Scholar] [CrossRef]
[6]. Ramage JL, Varacallo M, Anatomy, Shoulder and Upper Limb, Hand Guyon Canal. [Updated 2020 Sep 8]StatPearls 2021 Jan Treasure Island (FL)StatPearls PublishingAvailable from: https://www.ncbi.nlm.nih.gov/books/NBK534814/ [Google Scholar]
[7]. Middleton SD, Anakwe RE, A 37-year-old man with numbness in the handCMAJ 2015 187(8):593-95.10.1503/cmaj.14044125691791 [Google Scholar] [CrossRef] [PubMed]
[8]. Shea JD, McClain EJ, Ulnar-nerve compression syndromes at and below the wristJ Bone Joint Surg Am 1969 51:1095-103.10.2106/00004623-196951060-00004 [Google Scholar] [CrossRef]
[9]. Yuen JC, Wright E, Johnson LA, Culp WC, Hypothenar Hammer Syndrome: An update with algorithms for diagnosis and treatmentAnnals of Plastic Surg 2011 67(4):429-38.10.1097/SAP.0b013e31820859e121372671 [Google Scholar] [CrossRef] [PubMed]
[10]. Bernik JT, Montoya M, Dardik H, Bernik TR, Ulnar artery aneurysm and hypothenar hammer syndromeJ Vasc Surg Cases Innov Tech 2018 4(2):131-32.10.1016/j.jvscit.2017.09.00729955673 [Google Scholar] [CrossRef] [PubMed]
[11]. Little JM, Ferguson DA, The incidence of the hypothenar hammer syndromeArch Surg 1972 105:684-85.10.1001/archsurg.1972.041801100090045081541 [Google Scholar] [CrossRef] [PubMed]
[12]. Aleksenko D, Varacallo M, Guyon Canal Syndrome. [Updated 2020 Jul 20]In: StatPearls [Internet] 2021 Jan Treasure Island (FL)StatPearls PublishingAvailable from: https://www.ncbi.nlm.nih.gov/books/NBK431063/ [Google Scholar]
[13]. Monacelli G, Rizzo MI, Spagnoli AM, Monarca C, Scuderi N, Ulnar artery thrombosis and nerve entrapment at Guyon’s canal: Our diagnostic and therapeutic algorithmIn Vivo 2010 24(5):779-82. [Google Scholar]