A Rare Case of Pericardial Tuberculoma with Impending Tamponade in a 52-Year Old Woman: A Case Report
Clement C̀ Kabakama1, Zahra Daudi Khan2, Pilly Chillo3, Amos Rodger Mwakigonja5
1 Resident PharmD Researcher, Department of Internal Medicine, Muhimbili University of Health and Allied Sciences, Dar-es-Salaam, Tanzania.
2 Resident MMED, Department of Internal Medicine, Muhimbili University of Health and Allied Sciences, Dar-es-Salaam, Tanzania.
3 Senior Lecturer and Cardiologist, Department of Internal Medicine, Muhimbili University of Health and Allied Sciences, Dar-es-Salaam, Tanzania.
4 Professor and Head, Department of Pathology, Muhimbili University of Health and Allied Sciences, Dar-es-Salaam, Tanzania.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Clement C̀ Kabakama, Post Box 65252, Muhimbili Dar-Es Salaam, Tanzania.
E-mail: cleykabakama@gmail.com
Pericardial tuberculoma is a rare complication of tuberculous pericarditis. It may mimic a compressive mediastinal mass, often misinterpreted as a mediastinal tumour. Since, it arises from the pericardium, pericardial tuberculoma invariably compresses structures of the heart and may present with features of either-sided heart failure depending on the side of the compression. Hereby, the authors present a case of a 52-year-old woman with progressive difficulty in breathing and symptoms of right-sided heart failure as well as clinical signs of impending cardiac tamponade following a history of extra-pulmonary tuberculosis. Echocardiogram examination revealed a mass compressing the right side of the heart but was inconclusive of the mass origin. CT Scan of the chest showed a mass arising from the pericardium. The mass was later surgically excised. Histopathology confirmed pericardial tuberculosis and a diagnosis of a pericardial tuberculoma was reached. Patient’s heart failure symptoms regressed after surgery and she was discharged to continue with anti-tuberculosis regime. This report discusses the inclusion of pericardial tuberculoma in the differential diagnoses of cardiac compressing masses, particularly in tuberculosis endemic areas and emphasise on prompt CT Scan imaging when echocardiogram is inconclusive.
Cardiac masses, Extra-pulmonary tuberculosis, Mediastinal mass, Post-tuberculous sequalae, Tuberculosis complications
Case Report
A 52-year-old-woman presented with progressive difficulty in breathing for the past six months, dull-aching chest discomfort accompanied with dry cough for six months and abdominal distension for the preceding two months. Furthermore, she gave a history of being diagnosed with tuberculosis three years back, where she presented to a peripheral hospital with history of cough, weight loss, drenching night sweats and fever. A diagnosis of extra-pulmonary tuberculosis was reached following a negative sputum for acid fast bacilli test. She was prescribed 8-month anti-tuberculosis regimen with good compliance with good compliance and she completed the course about two years prior to presentation at this hospital.
The patient however continued to have symptoms of low grade fever from the past three years progressively with weight loss and now with shortness of breath, abdominal distension and dull-aching chest discomfort. There was no history of coughing up blood and she denied history of difficulty in swallowing, hoarseness of voice or posture-related symptoms. Neither was there any history of nausea, vomiting or change in bowel habits. She is a mother of five children and five years postmenopausal, never smoked, nonalcoholic, not hypertensive or diabetic.
The Body Mass Index (BMI) was 18.5 kg/m2. She was moderately pale, not jaundiced; had palpable, firm, nontender, mobile left axillary and supra-clavicular lymph nodes (approximately 1.5 cm). The extremities were warm with bilateral pitting oedema of the lower limbs. Her pulse rate was 96/minute, good volume and synchronous with other peripheral pulses. Supine BP was 115/75 mmHg, with negative pulsus paradoxicus. The Jugulo-Venous Pressure (JVP) was raised at 9 cm/water and a positive Kussmaul sign was noted. The apex beat was undisplaced, S1 and S2 were unremarkable. There were no murmurs but a pericardial knock was heard. Her respiratory rate was 14 breaths/min and she was saturating at 96% in room air. Chest findings were consistent with left sided pleural effusion. Abdominal examination revealed a uniformly distended abdomen, hepatomegaly of 18 cm and spleen that was palpable 12 cm below the left costal margin and positive shifting dullness. There were no distended veins noted. Other systems were essentially normal.
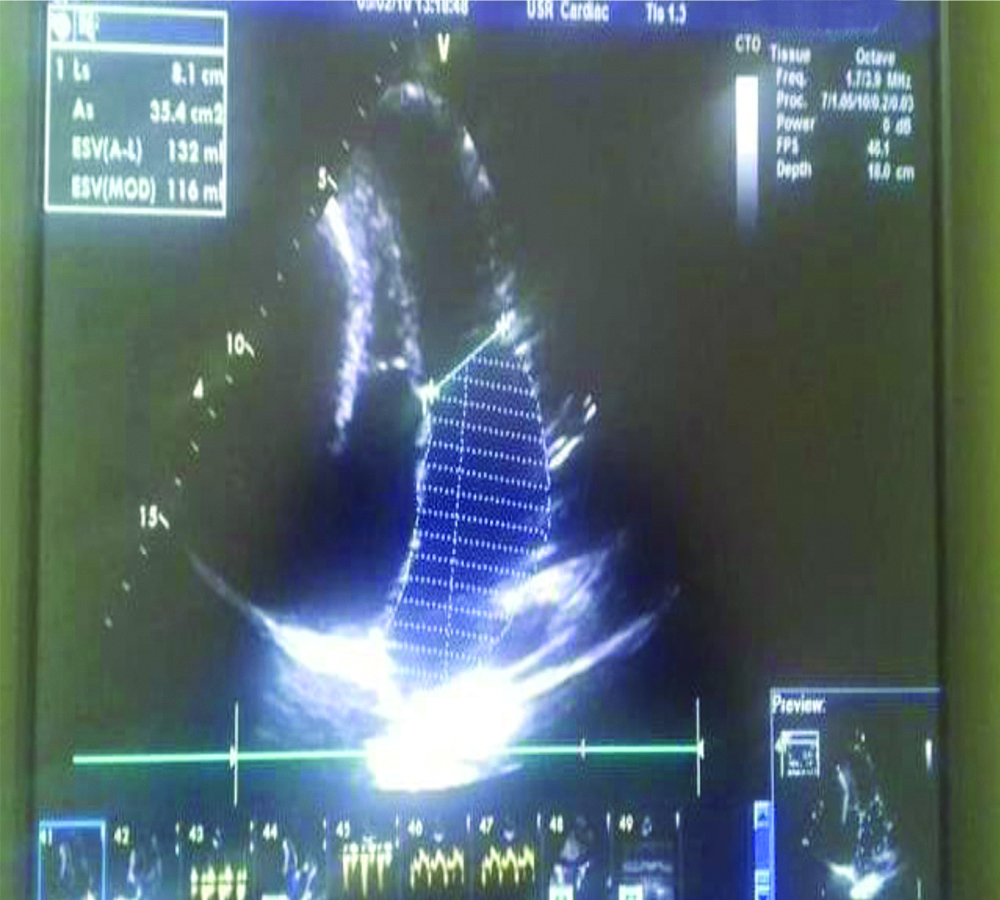
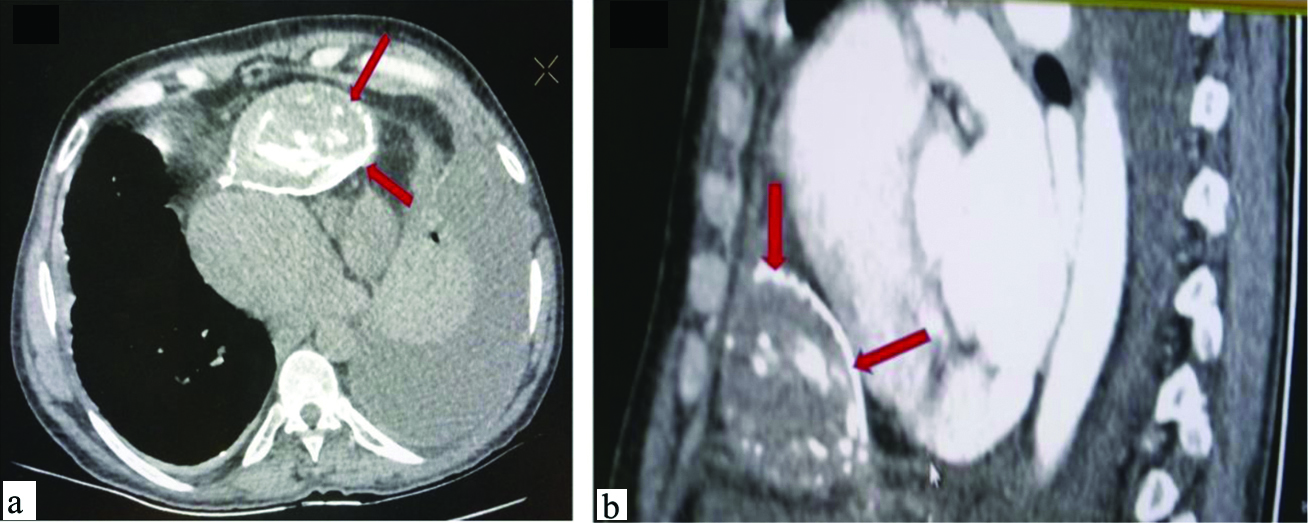
The laboratory work-up showed that patient had anemia (Hb 9.2 g/dL) with normal white cell counts and differentiation, erythrocyte sedimentation rate of 10 mm/hour, normal serum creatinine and normal liver function tests. Serum ADA was raised at 43.58 U/L (normal 0-15 U/L), had normal thyroid function tests and blood work-up for tumour markers was negative. The chest radiograph revealed widened mediastinum (8 cm on supine AP view). Her ECG showed sinus tachycardia with low-voltages in all leads. On echocardiogram examination, the pericardium was found to be thickened and calcified and the right atrium and ventricle were noted to be compressed [Table/Fig-1]. However, the echocardiogram examination could not ascertain the origin/cause of the right heart compression. The left heart was unremarkable and a left ventricular ejection fraction of 70% was noted. Trans-mitral Doppler studies in combination with tissue Doppler studies revealed echocardiographic features suggestive of constrictive pericarditis. A CT Scan of the chest was then ordered and the scan revealed a large well-defined calcified non-enhancing mass within the anterior mediastinum in continuity with the pericardium, compressing the right heart [Table/Fig-2a,b].
Echocardiogram found thickened and calcified pericardium and compressed right ventricle and atrium.
CT Scan of the chest showing mass (arrows) in the anterior mediastinum arising from the pericardium.
A diagnosis of pericardial mass was reached and the patient was referred to cardiothoracic surgeons where a decision to perform surgical pericardiectomy with minimal invasive technique was proposed for the relief of symptoms, as well as to confirm the diagnosis. Before pericardiectomy, patient had fine needle aspiration biopsy of the mass which revealed no malignancy.
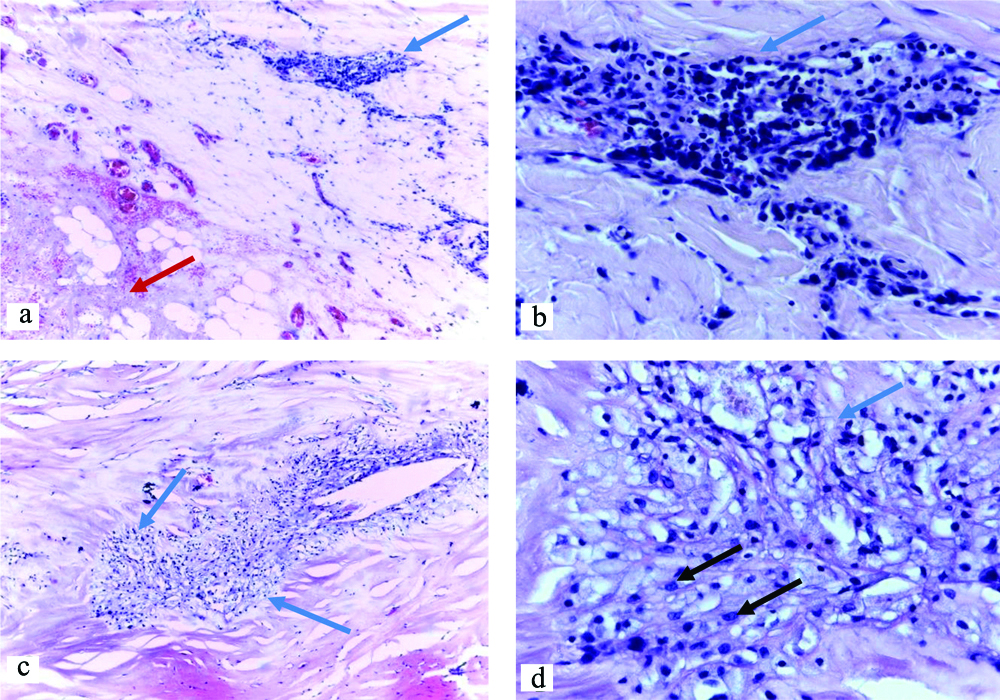
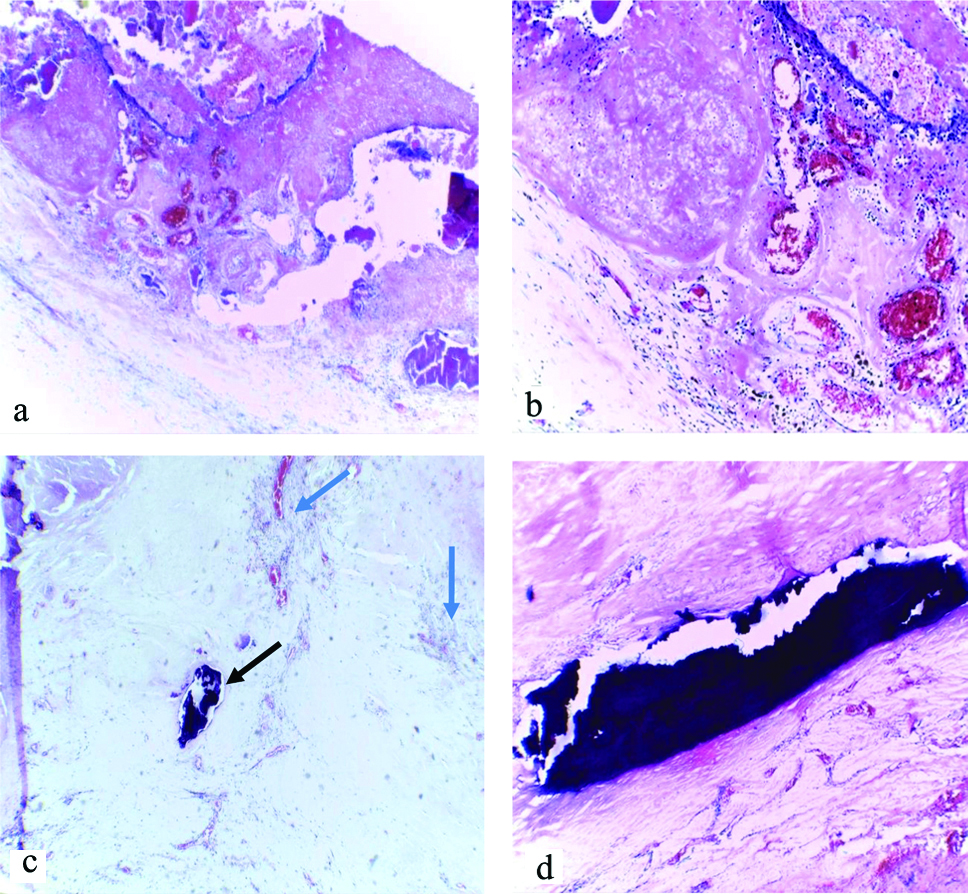
Pericardiectomy confirmed a caseating mass that originated from the pericardium and measured 6×8 cm in gross examination. Histology revealed clusters of chronic inflammatory cells as well as caseation and calcification consistent with tuberculosis of the pericardium [Table/Fig-3,4].
Histological (H&E) sections of the pericardium showing granulomas (blue arrows), caseous necrosis (red arrow) and epithelioid cells (black arrows); [(a&c) x10, (b&d) x40 Magnification].
Histological (H&E) sections of the pericardium showing extensive caseous necrosis [(a)x10 & (b)x40]; granulomas (blue arrows, c) and calcifications [black arrows (d)x10 & h (x40)].
The patient’s symptoms improved after surgery and on the basis of raised ADA and presence of constitutional symptoms, she was kept on anti-tuberculous treatment regimen which included (isoniazid, rifampicin, pyrazinamide and ethambutol for two months and continue with rifampicin and isoniazid for four months). She was discharged 14 days postsurgery without heart failure symptoms and was to be followed-up after six months.
Discussion
Tuberculosis is endemic in sub Saharan Africa [1]. Tuberculous pericarditis as an extra-pulmonary manifestation of tuberculosis has been reported to occur in 1-4% of cases [2,3]. The common complications of tuberculous pericarditis are pericardial effusion, often presenting with large effusions with or without tamponade [4], as well as constrictive pericarditis which is a later manifestation [5]. This report was an unusual case of pericardial tuberculoma which is a rare complication of tuberculous pericarditis.
Tuberculomas are clinical manifestation of tuberculosis where tubercles compile into a firm lump therefore presenting as solid masses. The usual site of extrapulmonary tuberculomas is the brain but tuberculomas rarely occur in the heart where they can arise from the pericardium [6] and even as intra-cardiac masses [7]. Histologically, tuberculomas consist of a central core of caseating necrosis with a surrounding wall of a florid granulomatous reaction containing Langhan’s giant cells, epithelioid histiocytes and lymphocytes [8]. When tuberculomas arise from the pericardium, they invariably compress the heart chambers and similar to the index case, they are more likely to compress the right side of the heart. This has been explained as probably due to the frequent tuberculous involvement of the right mediastinal lymph nodes with consequent spread to the right side of the heart [9].
Clinically, pericardial tuberculomas mimic mediastinal masses and similar to the present case almost all previous reported cases were firstly misdiagnosed as mediastinal tumours [6,9]. Therefore, a finding of a compressed heart without a clear origin of the compressing mass on echocardiogram in a patient with prior diagnosis of tuberculosis should raise a possibility of a pericardial tuberculoma. In this case, the patient had also echocardiographic features of constrictive pericarditis as well as thickened pericardium which should increase the suspicion of a pericardial tuberculoma. Clinical signs of tamponade including Kussmaul’s sign and pulsus paradoxus can present in a patient with a pericardial tuberculoma that compresses the right ventricle and impairs its diastolic filling. In a setting of no or minimal pericardial effusion, the presence of these signs of impending tamponade should raise the possibility of a pericardial tuberculoma.
With increasing use of high-precision imaging tools, it is possible to make a diagnosis of a pericardial tuberculoma fast and therefore prompt initiation of proper treatment of this otherwise treatable condition when compared to its differentials i.e., mediastinal tumours. In this case, the CT Scan was quick to show the mass, however due to its rarity the conclusion that the mass arose from the pericardium was not straight forward. There were different opinions from radiologists, cardiologists and the cardiothoracic surgeons. Then the authors conducted a literature search which revealed similar CT Scans and echocardiogram images from previous case reports and therefore conclusion and consensus was reached. Of note, there is an under-representation of reported cases emanating from sub Saharan Africa where we found only one previous case reported [6]. It is possible that the condition is missed.
The patient underwent surgical excision which has the advantage of relieving the patient’s symptoms as well as confirming the diagnosis. In this case, the diagnosis of tuberculosis was confirmed by histology and supported by the raised serum markers (raised ADA). Others have found positive acid-fast bacilli and positive culture for mycobacterium tuberculosis in tissue samples from the tuberculoma [10] but the usual finding is that of granulomatous inflammation which include epithelioid cell granulomas and areas of necrosis [11], similar to the index finding. In this case there were many reasons pointing towards tuberculosis as the causative agent, and the patient responded well after surgery and on antituberculosis treatment.
Conclusion(s)
The authors presented a rare case of tuberculous pericarditis complication. Due to the high tuberculosis burden in the region, this finding may be present much more than currently reported. The authors expect the case to raise awareness and therefore lead to prompt diagnosis and treatment of this treatable condition. Pericardial tuberculoma should be in the list of differential diagnosis of cardiac compressing masses, especially in TB endemic regions like sub Saharan Africa.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Apr 30, 2020
Manual Googling: Sep 23, 2020
iThenticate Software: Jan 20, 2021 (9%)
[1]. Global tuberculosis report. Geneva: World Health Organization; 2018. Licence: CCBY-NC-SA3.0IGO [Google Scholar]
[2]. Sagrista-Sauleda J, Permanyer-Miralda G, Soler-Soler J, Tuberculous pericarditis: Ten year experience with a prospective protocol for diagnosis and treatmentJournal of the American College of Cardiology 1988 11(4):724-28.10.1016/0735-1097(88)90203-3 [Google Scholar] [CrossRef]
[3]. Larrieu AJ, Tyers GF, Williams EH, Derrick JR, Recent experience with tuberculous pericarditisThe Annals of Thoracic Surgery 1980 29(5):464-68.10.1016/S0003-4975(10)61681-5 [Google Scholar] [CrossRef]
[4]. Cegielski JP, Lwakatare J, Dukes CS, Lema LE, Lallinger GJ, Kitinya J, Tuberculous pericarditis in Tanzanian patients with and without HIV infectionTubercle and Lung Disease: The official Journal of the International Union against Tuberculosis and Lung Disease 1994 75(6):429-34.10.1016/0962-8479(94)90116-3 [Google Scholar] [CrossRef]
[5]. Schrire V, Experience with pericarditis at Groote Schuur Hospital, Cape Town: An analysis of one hundred and sixty cases studied over a six-year periodSouth African Medical Journal = Suid-Afrikaanse Tydskrif Vir Geneeskunde 1959 26(33):810-17. [Google Scholar]
[6]. Leye M, Jobe M, Diatta S, Ndiaye MB, Aw F, Deguenonvo GN, A case of pericardial tuberculoma presenting as a left anterior chest wall massInternational Archives of Medicine 2013 6(1):4810.1186/1755-7682-6-4824350768 [Google Scholar] [CrossRef] [PubMed]
[7]. Ngow HA, Khairina WM, Right atrial tuberculoma: A diagnosis too lateCardiology Journal 2011 18(5):560-63.10.5603/CJ.2011.0014 [Google Scholar] [CrossRef]
[8]. Chang BC, Ha JW, Kim JT, Chung N, Cho SH, Intracardiac tuberculomaThe Annals of Thoracic Surgery 1999 67(1):226-28.10.1016/S0003-4975(98)01081-9 [Google Scholar] [CrossRef]
[9]. Jeilan M, Schmitt M, McCann G, Davies J, Leverment J, Chin D, Images in cardiovascular medicine. Cardiac tuberculomaCirculation 2008 117(7):984-86.10.1161/CIRCULATIONAHA.107.69176618285579 [Google Scholar] [CrossRef] [PubMed]
[10]. Farnetano BDS, Farias ML, Mota GSM, Leão CN, Machareth MMV, Pericardial tuberculosis-A case reportJ Tuberc Ther 2016 1(1):102 [Google Scholar]
[11]. Hajsadeghi S, Iranpour A, Kalantari S, Dashti F, A rare manifestation of extrapulmonary tuberculosis: left ventricular cardiac tuberculoma in an HIV infected male “case report”Cardiovasc Diagn Ther 2020 10(5):1341-44.10.21037/cdt-20-44633224758 [Google Scholar] [CrossRef] [PubMed]