Isolated Fallopian Tubal Torsion Complicated by a Large Hydrosalpinx in a Perimenopausal Woman
Masanori Kanemura1, Atsushi Yoshida2, Akihiko Toji3, Yumi Murayama4, Emi Iwai5
1 Medical Doctor, Department of Obstetrics and Gynaecology, Osakaminami Medical Centre, Kawachinagano, Osaka, Japan.
2 Medical Doctor, Department of Obstetrics and Gynaecology, Osakaminami Medical Centre, Kawachinagano, Osaka, Japan.
3 Medical Doctor, Department of Obstetrics and Gynaecology, Osakaminami Medical Centre, Kawachinagano, Osaka, Japan.
4 Medical Doctor, Department of Obstetrics and Gynaecology, Osakaminami Medical Centre, Kawachinagano, Osaka, Japan.
5 Medical Doctor, Department of Obstetrics and Gynaecology, Osakaminami Medical Centre, Kawachinagano, Osaka, Japan.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Masanori Kanemura, 2-1 Kidohigashi, Kawachinagano, Osaka, Japan.
E-mail: kanemura@ommc-hp.jp
Adnexal torsion frequently causes acute pelvic pain in women. Ovarian tumour torsion is common; twisting and torsion of a fallopian tube are rare. This report presents a rare case of fallopian tubal torsion requiring the management of a large hydrosalpinx with laparoscopic surgery. A 48-year-old woman reported with acute abdominal pain and lower abdomen tenderness. Transvaginal ultrasonography and Magnetic Resonance Imaging (MRI) showed a cystic mass on the anterior uterine surface. Emergency surgery was performed for a suspected torsion of the left ovarian cyst. In the abdominal cavity, the left fallopian tube was enlarged (neonatal head size), dark purple coloured, and exhibited a 180° torsion; the left ovary was normal. Laparoscopic left salpingectomy was performed and the postoperative course was uneventful. Surgical pathology revealed hydrosalpinx with torsion. As diagnosing isolated fallopian tube torsion before surgery is difficult, laparoscopic surgery is useful in diagnosing and treating isolated tubal torsion.
Acute abdomen, Adnexal torsion, Laparoscopic surgery
Case Report
A 48-year-old perimenopausal woman, gravida 2 para 2, visited Osakaminami Medical Centre because of two days of persistent lower abdominal pain. She had undergone surgery for breast cancer two years ago. She observed menstrual irregularity with longer menstrual cycles and her last menses occurred four months ago.
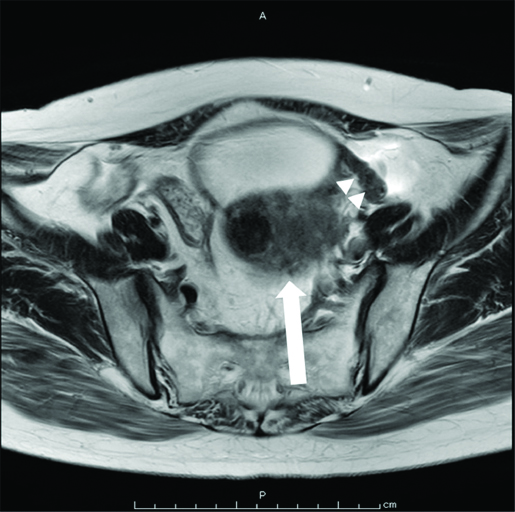
On examination, her vitals were stable with pulse rate of 90/min and systemic examination was within normal limits. The patient had rebound tenderness in lower abdomen. Vaginal ultrasonography confirmed the presence of a cystic mass of 87.8 mm diameter without a solid component, suggestive of an ovarian tumour. Ascites was scant, and there were no abnormal findings of the uterus and the right adnexa. MRI showed a cystic mass without any fat component [Table/Fig-1]. In the axial image, a coil-like structure was detected between the uterus and the cyst [Table/Fig-2]. Normal ipsilateral ovary could not be detected.
T2-weighted MRI scan demonstrating cystic mass (arrow) without any solid part (Sagittal).

T2-weighted MRI scan demonstrating a coil-like structure (arrow heads) between the uterus (arrow) and the cyst (Axial).
All biochemical and haematological parameters were within normal limits except the WBC count, which was 13870/μL (normal 3300-8600/μL). The serum tumour marker levels were within the normal range: CA125, 14.3 U/mL (normal <35.0 U/mL); CA19-9, 17.6 U/mL (normal <37.0 U/mL); and Carcinoembryonic Antigen (CEA), 2.0 ng/mL (normal <5.0 ng/mL).
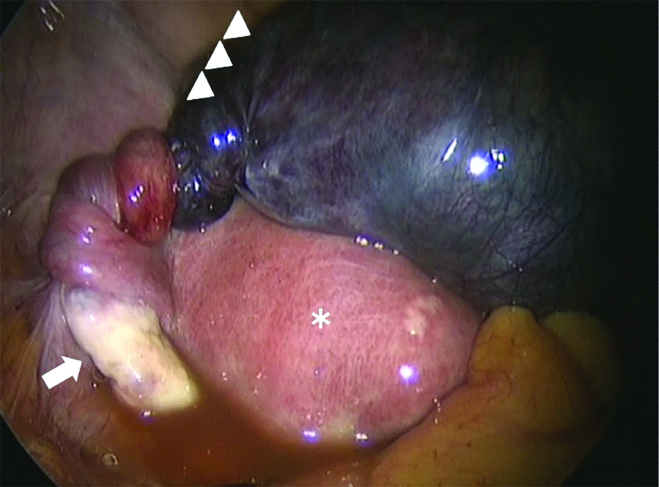
The diagnosis of the torsion of the ovarian cyst was made based on these data, and laparoscopic surgery was performed. An exploratory laparoscopy revealed an enlarged (about 9-10 cm) left fallopian tube, appearing dark purple in colour, exhibiting a 180° torsion. However, no abnormality was found in the left ovary [Table/Fig-3]. A laparoscopic left salpingectomy was performed.
Laparoscopy revealed a necrotic, twisted, left tubal mass of 9 cm diameter (arrow head) above the normal uterus (asterisk) and left ovary (arrow).
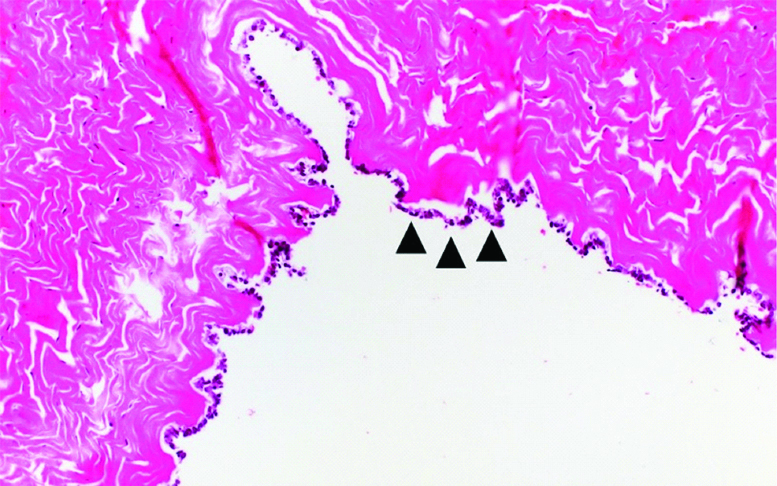
The patient’s postoperative course was uneventful. She was discharged on the fourth postoperative day. The pathological findings confirmed that the left fallopian tube dilated with one layer of squamous metaplasia, with necrosis and haemorrhage [Table/Fig-4]. It was suggested that the ischaemic changes were caused by the torsion of the hydrosalpinx.
The left fallopian tube dilated with one layer of squamous metaplasia (arrow heads), with necrosis and haemorrhage (H&E x20).
Discussion
Acute pelvic pain in women is caused by various diseases of the reproductive tract. Ectopic pregnancy, leaking or rupture of an ovarian cyst, adnexal torsion, Pelvic Inflammatory Disease (PID), tubo-ovarian abscess, uterine leiomyomas, and endometriosis may be considered for its differential diagnoses. Inappropriate diagnosis can lead to serious morbidity and even mortality [1]. Therefore, preoperative diagnosis is very important. Isolated fallopian tubal torsion is extremely rare, with an incidence of approximately 1 in 1,50,000 women [2]. To the best of our knowledge, there is only one report of a torsion on hydrosalpinx larger than 8 cm [3]. This was a rare case of fallopian tubal torsion, complicated by a large hydrosalpinx, which was managed with laparoscopic surgery.
Isolated fallopian tubal torsion primarily affects ovulating women, and is rarely seen in postmenopausal women [4]. It may occur more rarely in the premenarchal [5] or perimenopausal period [6]. There are intrinsic and exogenous causes of tubal torsion. The intrinsic causes include congenital anomalies in the length and shape of the fallopian tube, or acquired pathologies, such as hydrosalpinx, haematosalpinx, fallopian tube tumour, and previous fallopian tube ligation. The exogenous causes include ovarian or paraovarian tumours, adhesions, pelvic infections, pelvic congestion, and trauma [7]. In this case as well, a hydrosalpinx of approximately 9 cm diameter was observed.
In hydrosalpinx, the distal end of the fallopian tube is blocked because of inflammation or adhesion, and fluid accumulates inside the fallopian tube. Symptoms such as abdominal pain and increasing vaginal discharge due to inflammation may occur in women with hydrosalpinx, but many patients are asymptomatic. PID is often an ascending infection and is caused by sexually transmitted diseases, such as chlamydia. PID can be a source of infertility and is often found at the reproductive age. After menopause, it is estimated that neoplasms such as cancer can impair the passage of the fallopian tube and result in a high risk of developing hydrosalpinx and haematosalpinx [8]. In this case, as a result of the torsion of the fallopian tube and congestion, a haematosalpinx-like condition was observed. However, there was no neoplasm such as tubal cancer. There was no history of PID or tubal ligation, and because of its asymptomatic nature, it was not discovered until it was twisted.
A preoperative diagnosis of isolated tubal torsion is indistinguishable because its clinical symptoms are similar to those of ovarian torsion. Therefore, images become important for diagnosis. In hydrosalpinx, fluid accumulates inside the fallopian tube, and the hydrosalpinx can appear as an expanded tubular structure. The diagnosis is more reliable if incompletely eliminated mucosal and submucosal plicae are found along the wall [9]. However, it is difficult to distinguish it from ovarian cysts if there are no such findings. In isolated tubal torsion, ultrasonographic findings include tubal dilation with thickened echogenic walls and internal debris or concomitant cystic mass away from the ovaries [10].
MRI makes it possible to easily distinguish normal ovaries from cystic masses, and the whirlpool sign of a twisted pedicle may be observed on T2-weighted magnetic resonance images. The identification of ipsilateral normal ovaries is important in isolated tubal torsion cases. Contrast-weighted subtraction T1-weighted MR imaging helps to detect the vascularity of the affected organs [11]. In this case, there was an incomplete disappearance of mucous and submucosal plicae, and the left ovary was not detected in the MRI findings. Therefore, it was not possible to make a definitive diagnosis of tubal torsion before surgery. However, as a coil-like structure was observed continuously in the cyst; the findings led to the diagnosis of torsion.
Laparoscopy is less invasive than open surgery and suitable for the diagnosis and treatment of adnexal torsion. For isolated tubal torsion, prompt diagnosis is essential. If the time of diagnosis after the occurrence of torsion is short and the tissue is not irreversibly changed, it may be possible to salvage the fallopian tube by releasing the torsion, which will resume blood flow [12]. However, it is not considered a standard treatment because it has not been studied in terms of future tubal function. In examinations of ovarian torsion, the maintenance of function by detorsion can reach up to 50% [13]. To improve the results, Philips K et al., proposed detorsion, as the time interval between the twisting and the irreversible damage is unclear [14]. In this case, a salpingectomy was performed because there was no need for fertility preservation.
Conclusion(s)
Although isolated tubal torsion is a very rare disease and difficult to diagnose before surgery, it is considered that laparoscopic surgery, which is a minimally invasive surgery, is an appropriate treatment for ovarian torsion. However, it is not possible to determine whether salpingectomy or detorsion is the more optimal procedure since the number of such cases is currently limited. Further studies of future cases are required to determine the optimal procedure.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 07, 2020
Manual Googling: Dec 23, 2020
iThenticate Software: Jan 21, 2021 (4%)
[1]. Rapkin AJ, Nathan L, Pelvic pain and DysmenorrheaIn Berek & Novak’s Gynecology 2012 15th edBaltimoreThe Williams & Wilkins Co:470-504. [Google Scholar]
[2]. Hansen OH, Isolated torsion of the fallopian tubeActa Obstet Gynecol Scand 1970 49:03-06.10.3109/000163470091575065519474 [Google Scholar] [CrossRef] [PubMed]
[3]. Lim WH, Roex AJ, Laparoscopic management of a fallopian tubal torsion complicated by a large hydrosalpinxInt J Womens Health 2011 3:381-84.10.2147/IJWH.S2463922140325 [Google Scholar] [CrossRef] [PubMed] [PubMed]
[4]. Comerci G, Colombo FM, Stefanetti M, Grazia G, Isolated fallopian tube torsion: A rare but important event for women of reproductive ageFertil Steril 2008 90(4):1198.e23-25.10.1016/j.fertnstert.2007.08.05717953952 [Google Scholar] [CrossRef] [PubMed]
[5]. Huang FJ, Chang SY, Lu YJ, Laparoscopic treatment of isolated tubal torsion in a premenarchal girlJ Am Assoc Gynecol Laparosc 1999 6:209-11.10.1016/S1074-3804(99)80105-4 [Google Scholar] [CrossRef]
[6]. Shukla R, Isolated torsion of the hydrosalpinx: A rare presentationBr J Radiol 2004 77:784-86.10.1259/bjr/3628828715447969 [Google Scholar] [CrossRef] [PubMed]
[7]. Orazi C, Inserra A, Lucchetti MC, Schingo PM, Isolated tubal torsion: A rare cause of pelvic pain at menarcheSonographic and MR findings. Pediatr Radiol 2006 36:1316-18.10.1007/s00247-006-0308-x17021718 [Google Scholar] [CrossRef] [PubMed]
[8]. Khan M, Amin SV, Srinivas SB, Shivananda RP, Patil N, Hydrosalpinx as a Rare Presentation of Synchronous Ovarian and Endometrial Carcinoma- A Case ReportJ Clin Diagn Res 2016 10(7):QD01-03.10.7860/JCDR/2016/18304.810227630913 [Google Scholar] [CrossRef] [PubMed]
[9]. Kim MY, Rha SE, Oh SN, Jung SE, Lee YJ, Kim YS, Imaging findings of hydrosalpinx: A comprehensive reviewRadiographics 2009 29(2):495-507.10.1148/rg.29208507019325061 [Google Scholar] [CrossRef] [PubMed]
[10]. Rezvani M, Shaaban AM, Fallopian tube disease in the nonpregnant patientRadiographics 2011 31(2):527-48.10.1148/rg.31210509021415195 [Google Scholar] [CrossRef] [PubMed]
[11]. Iraha Y, Okada M, Iraha R, Azama K, Yamashiro T, Tsubakimoto M, CT and MR Imaging of Gynecologic EmergenciesRadiographics 2017 37:1569-86.10.1148/rg.201716017028753380 [Google Scholar] [CrossRef] [PubMed]
[12]. Wang PH, Yuan CC, Chao HT, Shu LP, Lai CR, Isolated tubal torsion managed laparoscopicallyJ Am Assoc Gynecol Laparosc 2000 7:423-27.10.1016/S1074-3804(05)60492-6 [Google Scholar] [CrossRef]
[13]. Wang JH, Wu DH, Jin H, Wu YZ, Predominant etiology of adnexal torsion and ovarian outcome after detorsion in premenarchal girlsEur J Pediatr Surg 2010 20:298-301.10.1055/s-0030-125411020533130 [Google Scholar] [CrossRef] [PubMed]
[14]. Phillips K, Fino ME, Kump L, Berkeley A, Chronic isolated fallopian tube torsionFertil Steril 2009 92:394.e1-3.10.1016/j.fertnstert.2009.01.15219342021 [Google Scholar] [CrossRef] [PubMed]