Mixed dentition period is marked with the beginning of second window of infectivity. It includes age group in which children leave primary school. Thus, it is the last age at which data can be easily gathered through a reliable sample of the school system. Caries pattern is multifactorial in context to type of diet, tooth structure, time of insult, microflora and salivary contents (salivary pH, buffering action, salivary flow, etc.). Factors like parent education, inadequacy of resources for dental treatment, lack of awareness, motivation and socio-economic status also influence the caries dynamics [1,2]. Caries pattern may provide insight on the aetiology of the disease like the pit and fissure (occlusal) surfaces which are the most susceptible, and the smooth surfaces (labial and lingual) being the least susceptible. In first and second permanent molars the frequently attacked sites are the occlusal surfaces [3,4]. In addition, proximal surfaces also have high caries susceptibility [3].
There exists a strong correlation between caries and developing occlusion among school children [5]. Malocclusion affects aesthetics and further occurrence of caries leads to negative effect on self-esteem. Unacceptable dental appearance has increased demand for orthodontic and restorative treatments among the population. Development of caries may be associated with malocclusion as it is difficult for patients to maintain good oral hygiene [6,7]. Good oral health is crucial for proper mastication; appearance and speech. However, the differences may be due to inadequate oral hygiene, variable access to dental care and other disability-related factors [8,9].
Craniofacial relationship may be a contributing factor in site of occurrence of caries i.e., mesial, distal, occlusal, palatal/lingual and buccal surfaces of primary and permanent molars [10,11]. Unfavourable tooth positions may lead to altered spillways, plunger cusp and trauma from occlusion. This may lead to food impaction, development of nidus for bacterial proliferation and prone sites for demineralisation. Tooth orientations, spillways and freeway spaces vary according to the type of terminal planes (flush, mesial, distal terminal plane) in primary molars and Angle’s molar relationship (Class I, Class II, Class III molar relationship) for permanent teeth. Other reasons for development of carious lesions specific to inter-molar relationship in different malocclusion groups may be the presence of functional and non-functional cusps and hence, resultant effect of retention of sticky food may vary with type of occlusion which may or may not be affected by flushing action of saliva as well. For instance, non-functional teeth in children with anterior open bite leads to accumulation of plaque and debris thereby causing caries [12-14].
Materials and Methods
This was a pilot study conducted by Department of Pedodontics and Preventive Dentistry, SGT University, in three Government and three Private schools of district Gurugram, Haryana, after obtaining an informed consent from parents of children to be enrolled in this study. This study was done in the month of November, 2019 after obtaining ethical clearance number i.e., SGTU/FDS/MDS/24/1/519.
This pilot study was a cross-sectional undergoing at multi-centric level. A 25% of the sample was initially screened. Hundred children between 3-5 years of age with primary dentition and hundred children between 8-10 years of age in mixed dentition period with erupted first permanent molar (which is the key to developing occlusion) were examined intraorally with low to moderate risk as per inclusion and exclusion criteria as follows:
Inclusion criteria: Children between 3-5 years of age with primary dentition, those between 8-10 years of age in mixed dentition phase with erupted first permanent molar and in low to moderate risk, i.e., with DMFT/dmft ≤3 [15] were included in the study.
Exclusion criteria: The children with high caries risk, high DMFT/dmft, developmental defects of enamel, carious due to developmental anomalies and those with systemic conditions and physically or mentally challenged were excluded from the study.
Sample size calculation: Sample size for this pilot study was calculated based on the literature available [16] on the prevalence of dental caries. The power of the study is 80% and based on the formula n=4pq/d2 (d square) with alpha value=5% and beta value=20% (Power is 1-beta=80%).
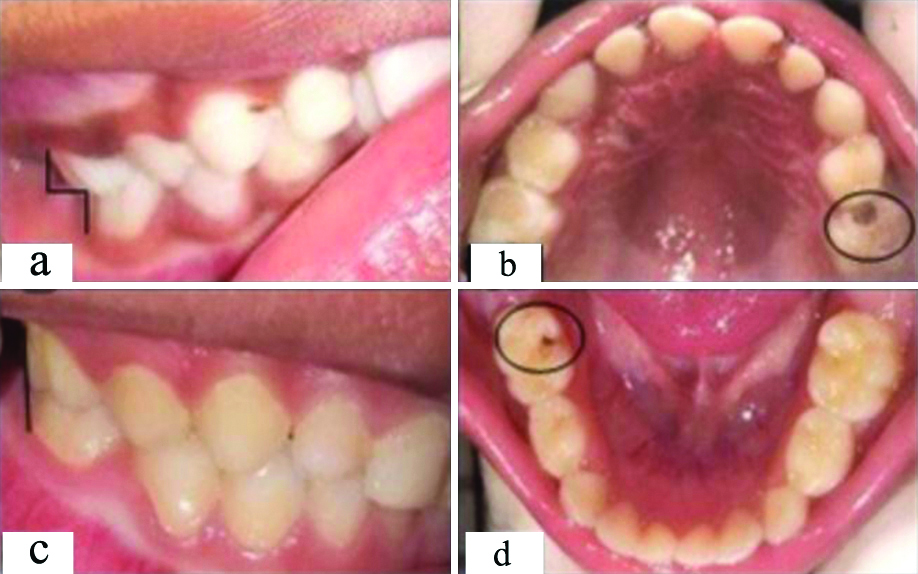
The examination was carried out by residents of Department of Pedodontics and Preventive Dentistry, SGT University. Before evaluation, the examiners underwent core-training for World Health Organisation (WHO) (decayed/missing/filled teeth-DMFT index) [17] and they evaluated 10 individuals from each group clinically and took their photographic records selected randomly for inter-examiner reliability. The inter-examiner reliability score of 0.9 was found using kappa statistics. In primary dentition (n=100, 3-5 years), collection of data after intraoral examination regarding type of occlusion (using Baume’s classification) [18] i.e., mesial step, distal step, flush terminal plane and their association with carious site (i.e., mesial, distal, occlusal, buccal and lingual/palatal) in primary right/left, maxillary/mandibular, first and second molars was done [Table/Fig-1].
Site of caries on the basis of Baume’s Classification of occlusion in primary molars: a) Mesial step terminal plane relationship; b) Caries on distal and occlusal aspect of 65; c) Flush terminal plane relationship; d) Caries on occlusal aspect of 85.
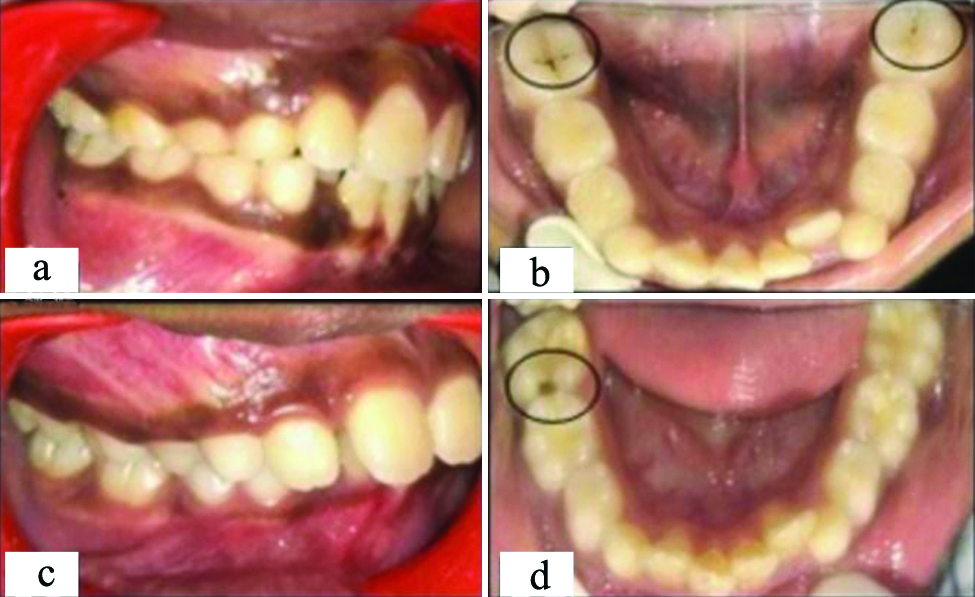
Similarly in mixed dentition (n=100, 8-10 years), collection of data regarding type of malocclusion (i.e., Angle’s Class I, Angle’s Class II and Angle’s Class III) and their association with carious site (i.e., mesial, distal, occlusal, buccal and lingual/palatal) in right/left, maxillary/mandibular, first permanent molar was done [Table/Fig-2] [19]. The intraoral photographs were taken only for positive findings in both groups. The children were examined according to WHO 2013 examination technique for the presence of dental caries using dmft/dmfs and DMFT/DMFS index using a CPI probe [15].
Site of caries on basis of Angle’s Classification of malocclusion in each permanent first molar: a) Angle’s Class I malocclusion; b) Caries on occlusal aspect of 36,46; c) Angle’s Class II malocclusion; d) Caries on mesial and occlusal aspect of 46.
Also, from obtained data, carious involvement as per scores of DMFT/dmft (i.e., dmft=0-1, 1-2, ≤3 and DMFT+dmft (DMFT+dmft=0-1, 1-2, ≤3) was analysed in both groups, respectively [15].
Statistical Analysis
Data was entered in Microsoft excel and analysed using SPSS (version 12). Qualitative data was presented as frequency and percentages. The results were subjected to statistical analysis using chi-square test and the level of significance was set at p≤0.05.
Results
The age group included for the study was 3-5 years and 8-10 years. In the sample of 100 school children of 3-5 years of age, the mean age was 4.59 (0.969) years, 4.60 (1.140) years and 4.00 (1.414) years in mesial, flush and distal step terminal plane malocclusion, respectively. In the age group 8-10 years, the mean age was 9.56 (0.546) years, 9.62 (0.506) years and 9.33 (0.577) years in Angle’s Class I, Angle’s Class II and Angle’s Class III malocclusion, respectively.
The number of males in the 3-5 years age group were 54 (93.1%), 3 (5.2%) and 1 (1.7%) in mesial, flush and distal step terminal plane malocclusion, respectively whereas the number of females were 39 (92.9%), 2 (4.8%) and 1 (2.4%), respectively. In the age group 8-10 years, the number of males were 47 (83.9%), 8 (14.3%) and 1 (1.8%) in Angle’s Class I, Angle’s Class II and Angle’s Class III malocclusion, respectively whereas the number of females were 37 (84.1%), 5 (11.4%) and 2 (4.5%), respectively.
As shown in [Table/Fig-3], in primary dentition (n=100) the number of individuals with mesial step terminal plane were highest i.e. 93% (n=93) compared to distal step terminal plane 2% (n=2) whereas that of flush terminal plane was found to be 5% (n=5).
Type of malocclusion in primary and permanent dentition and caries affected individuals.
| I. Type of malocclusion and caries affected individuals in 3-5-year-old school children |
|---|
| Type of malocclusion | No. of individuals N=100 | No. of caries affected individuals n=18 | % of caries affected individuals |
|---|
| Flush terminal | 5 | 1 | 20% |
| Mesial step | 93 | 17 | 18% |
| Distal step | 2 | 0 | 0 |
| II. Type of malocclusion and caries affected individuals in 8-10-year-old school children |
| Type of malocclusion | No. of individuals N=100 | No. of caries affected individuals n=22 | % of caries affected individuals |
| Class I | 84 | 17 | 20% |
| Class II | 13 | 5 | 38% |
| Class III | 3 | 0 | 0 |
Further in primary dentition, caries affected individuals with flush terminal plane were 20% (n=1/5) and in mesial step terminal plane, caries affected individuals were 18% (n=17/93).
In mixed dentition (n=100), number of Angle’s Class I malocclusion individuals were highest i.e., 84% (n=84) compared to individuals with Angle’s Class II i.e., 13% (n=13) and Angle’s Class III i.e., 3% (n=3) malocclusion.
Further in mixed dentition, caries affected individuals were highest in Angle’s Class II maloccusion i.e., 38% (5/13) compared to Angle’s Class I i.e., 20% (17/84) and no caries affected individual was found in children with Angle’s Class III malocclusion.
In context to carious surface involvement in mesial step terminal plane amongst caries affected individuals were 17 (18%), [Table/Fig-4] reveals that in maxillary right first primary molar (54), 24% mesio-occlusal, 12% disto-occlusal, 35% occlusal, 6% palatal and 18% buccal surfaces were involved. In context to maxillary right second primary molar (55), 12% mesio-occlusal and 12% occlusal surfaces were involved. In maxillary left first primary molar (64), 6% mesio-occlusal, 6% disto-occlusal, 12% occlusal and 6% buccal surfaces were involved each. The caries affected individuals with respect to mandibular arch included 18% mesio-occlusal,18% disto-occlusal and 35% occlusal surfaces in left first primary molar (74) whereas in right first primary molar (84), 12% mesio-occlusal, 12% occlusal, 6% lingual and 12% buccal surfaces were involved. In right second primary molar (85), 12% mesio-occlusal, 18% disto-occlusal, 29% occlusal, 6% lingual and, 6% buccal surfaces were involved. The site of caries on tooth number 54, 55, 64, 74, 84, and 85 were statistically insignificant in relation to type of malocclusion with p-values 0.874, 1.000, 1.000, 1.000, 1.000, 1.000, respectively.
Site of caries on the basis of type of malocclusion in primary molars.
| Tooth No. | Site of caries | Type of malocclusion | p-value |
|---|
| Flush terminalTotal=5Caries affected, 1, 20% | Mesial step Total=93Caries affected, 17, N%=18% |
|---|
| N (%) | N (%) |
|---|
| 54 | MO | 1 (100%) | 4 (24%) | 0.874 |
| DO | 0 (0%) | 2 (12%) |
| O | 1 (100%) | 6 (35%) |
| P | 0 (0%) | 1 (6%) |
| B | 0 (0%) | 3 (18%) |
| 55 | MO | 0 (0%) | 2 (12%) | 1.000 |
| DO | 0 (0%) | 0 (0%) |
| O | 0 (0%) | 2 (12%) |
| P | 0 (0%) | 0 (0%) |
| B | 0 (0%) | 0 (0%) |
| 64 | MO | 0 (0%) | 1 (6%) | 1.000 |
| DO | 0 (0%) | 1 (6%) |
| O | 0 (0%) | 2 (12%) |
| P | 0 (0%) | 0 (0%) |
| B | 0 (0%) | 1 (6%) |
| 65 | MO | 0 (0%) | 0 (0%) | NA |
| DO | 0 (0%) | 0 (0%) |
| O | 0 (0%) | 0 (0%) |
| P | 0 (0%) | 0 (0%) |
| B | 0 (0%) | 0 (0%) |
| 74 | MO | 0 (0%) | 3 (18%) | 1.000 |
| DO | 0 (0%) | 3 (18%) |
| O | 0 (0%) | 6 (35%) |
| P/L | 0 (0%) | 0 (0%) |
| B | 0 (0%) | 0 (0%) |
| 75 | MO | 0 (0%) | 0 (0%) | NA |
| DO | 0 (0%) | 0 (0%) |
| O | 0 (0%) | 0 (0%) |
| P/L | 0 (0%) | 0 (0%) |
| B | 0 (0%) | 0 (0%) |
| 84 | MO | 0 (0%) | 2 (12%) | 1.000 |
| DO | 0 (0%) | 0 (0%) |
| O | 0 (0%) | 2 (12%) |
| P/L | 0 (0%) | 1 (6%) |
| B | 0 (0%) | 2 (12%) |
| 85 | MO | 0 (0%) | 2 (12%) | 1.000 |
| DO | 0 (0%) | 3 (18%) |
| O | 0 (0%) | 5 (29%) |
| P/L | 0 (0%) | 1 (6%) |
| B | 0 (0%) | 1 (6%) |
MO: Mesio-occlusal; DO: Disto-occlusal; O: Occlusal; P/L: Palatal/Lingual; B: Buccal
Further in context to carious involvement in mixed dentition period, [Table/Fig-5] shows that in Angle’s Class I malocclusion (20% caries affected out of 84 individuals), 18% disto-occlusal and 18% occlusal surfaces of right maxillary first permanent molar (16) were caries affected whereas in left maxillary first permanent molar (26), 24% occclusal surfaces, 6% mesio-occlusal and 18% disto-occlusal were affected. In mandibular arch, left first permanent molar (36) showed 24% occlusal surfaces, 12% mesio-occlusal, 12% disto-occlusal and 12% lingual surfaces affected whereas in right first permanent molar (46), 29% occlusal, 6% lingual and 12% buccal surfaces were affected.
Site of caries on basis of type of malocclusion in each permanent first molar.
| Tooth No. | Site of caries | Type of malocclusion | p-value |
|---|
| Class ITotal=84Caries affected=17, 20% | Class IITotal=13Caries affected=5, N %=38% |
|---|
| N (%) | N (%) |
|---|
| 16 | MO | 0 (0%) | 0 (0%) | 0.989 |
| DO | 3 (18%) | 1 (20%) |
| O | 3 (18%) | 1 (20%) |
| P | 0 (0%) | 0 (0%) |
| B | 0 (0%) | 0 (0%) |
| 26 | MO | 1 (6%) | 0 (0%) | 0.999 |
| DO | 3 (18%) | 0 (0%) |
| O | 4 (24%) | 2 (40%) |
| P | 0 (0%) | 0 (0%) |
| B | 0 (0%) | 0 (0%) |
| 36 | MO | 2 (12%) | 0 (0%) | 0.998 |
| DO | 2 (12%) | 0 (0%) |
| O | 4 (24%) | 3 (60%) |
| L | 2 (12%) | 0 (0%) |
| B | 0 (0%) | 0 (0%) |
| 46 | MO | 0 (0%) | 0 (0%) | 1.000 |
| DO | 0 (0%) | 0 (0%) |
| O | 5 (29%) | 2 (40%) |
| L | 1 (6%) | 0 (0%) |
| B | 2 (12%) | 0 (0%) |
In Angle’s Class II malocclusion (38% caries affected out of 13 individuals), 20% disto-occlusal and 20% occlusal surfaces were caries affected in right maxillary first permanent molar (16), 40% occlusal surfaces were affected in left maxillary first permanent molar (26), 60% occlusal surfaces were affected in left mandibular first permanent molar (36) and 40% occlusal surfaces were affected in right mandibular first permanent molar (46).
The sites of caries on tooth number 16, 26, 36 and 46 were statistically insignificant with p-values 0.989, 0.999, 0.998 and 1.000, respectively in relation to type of malocclusion.
In [Table/Fig-6] caries affected molar (n=1) of flush terminal plane out of 5 individuals were in the range of dmft >2 ≤3, whereas in mesial molar relationship (n=17/93) 12%, 59%, 29% primary molars were in range of dmft=0-1, dmft=1-2 and dmft >2 ≤3, respectively. The caries occurrence according to dmft index in primary dentition was not associated with any type of malocclusion i.e., p-value=0.349.
Relation of caries in primary molars to dmft in different types of malocclusion.
| Type of malocclusion | Caries occurence in primary first and second molars | dmft=0-1 | dmft=1-2 | dmft>2≤3 | p-value |
|---|
| N | N (%) | N (%) | N (%) |
|---|
| Flush terminal plane | 1 | 0 (0 %) | 0 (0%) | 1 (100%) | 0.349 |
| Mesial step | 17 | 2 (12%) | 10 (59%) | 5 (29%) |
Similarly in [Table/Fig-7], the caries affected individuals in Angle’s Class I (n=17) out of 93 individuals showed that 29%, 41% and 29% permanent molars were in range of DMFT+dmft=0-1, DMFT+dmft=1-2 and DMFT+dmft >2 ≤3, respectively whereas 100% caries affected molars of Angle’s Class II (n=5) out of 13 individuals were in the range of DMFT+dmft >2 ≤3. The caries occurrence according to DMFT+dmft index in mixed dentition was significantly (p-value=0.020) associated with Angle’s Class II malocclusion.
Relation of caries in first permanent molars to DMFT+dmft in different types of malocclusion.
| Type of malocclusion | Caries occurence in permanent first molars | DMFT+dmft=0-1 | DMFT+dmft=1-2 | DMFT+dmft>2 ≤3 | p-value |
|---|
| N | N (%) | N (%) | N (%) |
|---|
| Class I | 17 | 5 (29%) | 7 (41%) | 5 (29%) | 0.020* |
| Class II | 5 | 0 (0%) | 0 (0%) | 5 (100%) |
p-value less than 0.05 to be considered siginificant
Discussion
Unfavourable tooth positioning is related to high incidence of caries which not only leads to poor diet habits and oral hygiene but also affects the anatomical characteristics of tooth structure. The decreased or asymmetric mastication and changes in the distribution of functional occlusal contact is known to be associated with carious lesions. Interproximal decay of primary molar results in decreased mesiodistal crown width leading to migration of adjacent teeth toward the affected area, which may reduce the dental arch length. This loss of arch length further cause tooth displacement, occlusal instability, dental crowding, and chewing disabilities [20]. Furthermore retentive food and intermolar relationship results in varying pattern of caries cavitation in primary as well as permanent dentition. The occurrence of caries in various types of molar inter arch relationships varies and so does the pattern of caries. The distribution of pattern of caries is helpful to understand the aetiology and also helps in opting for a suitable preventive treatment modality to save the dentition [3,21,22].
In the present study, various forms of malocclusion in both primary and mixed dentition were analysed, in a group of children aged between 3-5 and 8-10 years, respectively and its relationship with site of caries occurrence in molars in order to know about the frequently attacked sites of molars. Also, the relationship of dmft and DMFT+dmft in primary and mixed dentition with the caries occurrence in different types of malocclusion was evaluated.
In context to terminal plane in present study, [Table/Fig-3] represents that majority of individuals in 3-5 years age were having mesial step molar relationship (93%) followed by flush terminal plane (5%) and distal step molar relationship (2%), respectively. The prevalence of a flush terminal plane decreases with age, and the prevalence of a mesial step increases with age, most likely due to combination of mesial migration of the lower arch and a mesial shift of the mandible, which is probably caused by forward growth of the mandible and in in the present study, the children were mostly in the age group of 4-5 years [23]. This is concurrent with the survey by Kumar D et al., which concluded that the mesial step molar relationship was most common in 3-6-year-old children followed by flush terminal and distal step relationship [24]. It was further seen in our study that the caries affected individuals were maximum in flush terminal (20%) and mesial step (18%) plane. Lochib S et al., conducted a study in 2014 which was not in accordance with our study in which 1,000 pre-schoolers showed that most prevalent molar relationship was the flush terminal plane (66.0%) followed by mesial step (12.8%), distal step (2.4%) [25]. The reason for this result could be the range of population being mostly in the age group of 3 and 4 years. Similar results were seen in primary dentition of school children below 6 years in Davangere, in a study conducted by Shavi GR et al., [26].
In context to Angle’s malocclusion, majority of individuals in 8-10 years age, had Angle’s Class I malocclusion (84%) followed by Angle’s Class II (13%) and Angle’s Class III (3%) respectively which was in concurrence with Disha P et al., and Narayanan RK et al., [27,28]. Caries in permanent first molar was more associated with Angle’s Class II malocclusion in the present study (38%).
[Table/Fig-4] shows that occlusal, mesio-occlusal and disto-occlusal surfaces were the most caries affected sites in mesial step and flush terminal plane. This suggests that occlusal and proximal surfaces were most commonly affected. The reasons for development of interproximal carious lesions are contacting proximal surfaces of two adjacent teeth, limited salivary access and interproximal plaque accumulation [28]. The caries susceptibility of occlusal surfaces of primary molars are due to the fissure topography which is conducive for caries occurrence. Moreover, the children lack motor dexterity in the age group of 3-5 years which affects their brushing techniques [29]. The children should therefore be assisted while tooth brushing by their parents or guardians so that mechanical control of biofilm can be done thereby preventing faster progression of carious lesions in dentition.
[Table/Fig-5] shows that in mixed dentition, highly affected were occlusal surfaces of first permanent molars in Angle’s Class I as well as Angle’s Class II malocclusions because of various reasons such as the deep pits and fissures on the occlusal aspect, the large dimensions of crown which leads to accumulation of acid produced by microorganisms in oral cavity, and the early eruption of the tooth [30]. The early preventive measures such as application of fissure sealants and the use of fluoride varnishes among primary school children could help reduce the prevalence of caries in these teeth [31]. Sánchez-Pérez L et al., also stated in his study that complex surface morphology and inadequate access to oral hygiene measures as the reason for high prevalence of occlusal caries [32].
[Table/Fig-6,7] showed that caries affected molars were majorly in dmft/DMFT and dmft range 1-2. Result was significant when relation of caries in first permanent molars was compared to DMFT+dmft in different types of malocclusion (p-value=0.020*). In a study conducted by Farooqi FA et al., mean dmft/DMFT value was found to be 3.66±3.13 among 6-9-years-old and 1.94±2.0 among the 10-12-years-old children. Therefore, dmft is one of the prediction factor of increased caries risk both in primary and permanent dentition which ultimately affects the occlusion [33]. For a given DMFT, there is a specific pattern of caries within a population according to which as caries in the population declines, caries in the other susceptible surfaces (approximal) decreases considerably more than in the most susceptible surfaces (pits and fissures) [34].
Limitation(s)
The shortcomings of the present study are the small sample size which cannot be descriptive of an entire population. Larger sample size is required for better correlation of type of molar relationship and site of caries in the molar. Also, caries is a multifactorial disease, so the results maybe affected by diet and other individual habits of the patient.
Conclusion(s)
The study concludes that mesial step molar relationship was the most common malocclusion in primary dentition whereas in mixed dentition Angle’s Class I was the most common malocclusion. The type of malocclusion does not affect the surface pattern of caries on molars in primary and mixed dentition period. Decayed missing and filled caries index may be significantly associated with Angle’s Class II malocclusion according to present study. This study suggested that special preventive procedures may be planned for developing Angle’s Class I malocclusion in mixed dentition period for better oral health quality of life in developing years and later.
MO: Mesio-occlusal; DO: Disto-occlusal; O: Occlusal; P/L: Palatal/Lingual; B: Buccal
p-value less than 0.05 to be considered siginificant