The automobile industry is a large and growing industry in India and this industry employs many workers as manufacturers, distributors, retailers, and automobile garage workers. An automobile garage is a place where cars are repaired by automobile mechanics and technicians. These are also known as automobile car care centre, automobile workshop, automobile service centre etc., [1]. The workers of the automobile garages usually involve in different kinds of jobs like repairing, replacement, painting and routine monitoring of various car parts. The literature review revealed that garage workers have various kinds of health problems like respiratory discomfort due to dust, fumes, MSD due to long working hours, awkward posture, skin related problems due to paints and chemicals used on cars and last but not the least accidents and injuries [1-3].
Among all the problems, MSD is most common among automobile garage workers. Some studies showed that 86% garage workers in Malaysia [4] and 77% in Bangladesh [5] suffered from MSD in one or more parts of their body. In India, a study by James C et al., showed 84% auto mobile garage workers had MSD [6]. The reason of huge burden of MSD among the garage workers is quite clear. These workers usually work in standing, sitting, and lying position for a long time in the uncomfortable posture of the body [1]. They use some heavy machines and tools on repetitive basis in their daily routine job. All these factors lead to different types of musculoskeletal problems like low back pain, neck stiffness, pain in the joints of upper and lower extremities etc., and these discomforts reduce their work capacity or productivity, create mental stress and sometimes even give rise to fatal accidents and injuries.
Most of the musculoskeletal morbidities are preventable with some work place based simple cost-effective interventions. The regular screening of MSD among garage workers with an appropriate tool has an important role in its prevention by timely detecting the mild to severe MSDs. According to Bureau of Labour Statistics, the automobile machinery mechanics and garage workers is projected to increase by 17% from 2012 to 2022 all over the world, more rapidly than the average of the other employments [7]. Today, MSD is one of the big health problems experienced by the workers in different working environments around the world and also in India. The financial loss because of such issues, can affect the individual as well as the society [8]. Regular screening, early diagnosis using a simple tool has a huge role to combat the situation. Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) [9] had been created and used by Dr. Alan Hedge. CMDQ is a freely available self-reported screening tool for detection of MSD. The questionnaire is very easy to administer among workers and it gives a picture of MSD in last seven days with detailed history of site and frequency of the discomfort [10]. The discomforts at multiple sites of a person can be reported in CMDQ.
Though, there are some studies among automobile garage workers on MSD is available in Southern region of India [11,12], in Eastern India, there are paucity of studies about the matter. But, the MSD is a preventable health problem [13-15]. Some affordable measures like the ergonomically designed machines, proper training about body posture, small breaks during duty hours, rotational duty, stretching exercises etc., [16-20], can prevent the progression MSD among automobile workers. So, the current study was conducted with the aim to find out the proportion of MSD among auto mobile garage workers in Chetla, Kolkata and to describe the factors associated with the musculoskeletal discomfort.
Materials and Methods
The study was an observational study with cross-sectional design. It was conducted in the automobile garages of Chetla under urban field practice area of All India Institute of Hygiene and Public Health, Kolkata. The duration of the study was four months (November 2018 to February 2019). All the workers in automobile garages for ≥6 months were included in the study. Those who did not give informed written consent were excluded from the study.
Permission was obtained from the automobile garage authorities to conduct the study among their workers. Approval from Institutional Ethics Committee of AIIH & PH was also obtained (11th November, AIIHPH/IEC/PSM/2017/07). All the ethical issues were addressed accordingly during the study period.
Sample size calculation and sampling technique: The prevalence of musculoskeletal morbidity was 62% among automobile garage workers in a study done in urban area of Bangalore, Karnataka in the year 2016 [11].
So, in the current study the minimum sample size was:
(Zα/2)2PQ/L2 =(1.96)2×62.0×38.0/(10.0)2=91(Here, P=40.0, Q=100-40.0=60.0, L=Allowable absolute error=10%)
Considering non response rate of 10%, the final sample size was=91+10=101.
Around 20 automobile garages are situated at Urban field practice area of AIIH & PH in Chetla. Nine garage authorities gave permission to conduct the study in their garages. All the workers of these garages that fulfilled the selection criteria were included in the study.
Study tool: The main study tool was a pre-designed, pre-tested, structured schedule containing:
Sociodemographic characteristics
Behavioural characteristics (substance abuse)
Occupational profile
Cornell Musculoskeletal Discomfort Questionnaires (CMDQ)
CMDQ is a screening tool for MSD. In this tool frequency, severity and ability of musculoskeletal pain or discomfort to interfere with work in last seven days are reported by the study participants.
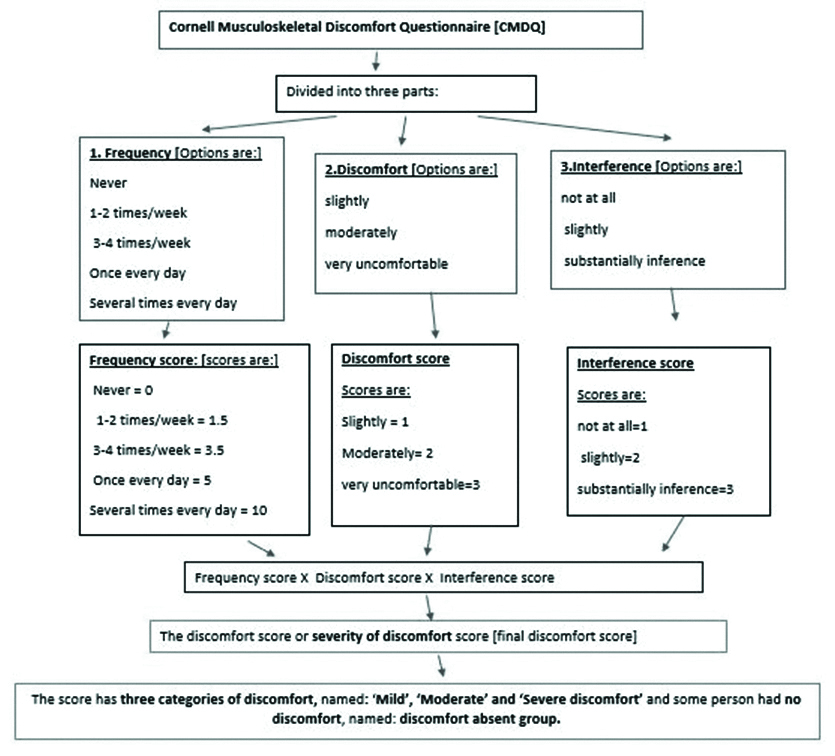
Discomfort was graded into three types: slightly, moderately and very uncomfortable and the score was 1,2,3 respectively. The interference with job was categorised into three groups: not at all, slightly, substantially inference and the score was 1,2,3 respectively for the three groups. The weightage was given to the frequency score (Never=0, 1-2 times/week=1.5, 3-4 times/week=3.5, Once every day=5, Several times every day=10) [10]. The discomfort or severity of discomfort score was calculated by multiplying the above frequency score (0, 1.5, 3.5, 5, 10) by the discomfort score (1,2,3) by the interference score (1,2,3). The range of total attainable score can be (0-35.50) [10].
For example, a person with frequency of discomfort ‘once every day’ would have a frequency score of 5, if discomfort is ‘slightly uncomfortable’ the score would be 1 and with ‘slight’ interference with job would score 2. The total discomfort or severity of discomfort score would be 10 (5×1×2=10) [Table/Fig-1].
Flow diagram showing Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) [9] and the scoring from the questionnaire in details [10].
Method of data collection: For data collection, workplace visit was done and face to face interview was conducted with the help of a pre-designed, pre-tested structured schedule. All the participants were explained about the purpose of the study. Anonymity and confidentiality were assured to the participants. After taking informed written consent, the participants were interviewed individually. In case of any disease or health problem reported by the study participant, appropriate advice was given by the researchers. The health check-up of all garage workers who were present on the day of data collection was done.
Study variables: Dependent Variable was MSD which is categorised as mild, moderate and severe discomfort (when discomfort was reported) and no discomfort (when no discomfort was reported) in CMDQ screening tool.
Mild discomfort: The CMDQ score 1.5 was considered as mild discomfort.
Moderate discomfort: The CMDQ score 1.6-10.5 was considered as moderate discomfort.
Severe discomfort: The CMDQ score>10.5 was considered as severe discomfort.
No discomfort or discomfort absent: The CMDQ score 0 was considered as no discomfort.
Independent variables were: Socio-demographic characteristics (age, education, per capita income, etc.,). Some of these variables were taken to logistic regression as independent variables. Age of the study participants were taken as a linear variable. The education variable was categorised into two groups (up to primary and above primary education) for final regression analysis. Per Capita Income (PCI) was also categorised into two groups {≤2000 and >2000 (RS)} based on median PCI for regression analysis. Occupational profile (duration of job, working hours per day, type of work etc.,).
Duration of work per week of the study participants were taken as a linear variable. The duration of job was categorised into two groups based on median value {≤18 and >18 (in years)} for final regression analysis. Working hours per day was also categorised into two groups (≤8 and >8) for regression analysis.
Statistical Analysis
Data analysis was done on IBM Statistical Package for the Social Sciences (SPSS) version 16 software. Descriptive and inferential statistics were analysed. Univariate logistic regression was done to find out the risk factors of musculoskeletal disorder. Moderate and severe discomfort were taken as dependent variable for logistic regression because the median of attainable CMDQ score was 1.5 and the CMDQ score of moderate and severe discomfort was ≥1.6. p-value ≤0.05 was taken as the statistical cut-off point.
Results
[Table/Fig-2] shows that, 30.7% of the study participants belonged to the age group 41-50 years and the mean age of the study participants was 43.35 years. All the study participants were males and 50.5% had primary school completion certificate.
Distribution of the study participants according to their background characteristics (N=101).
| Characteristics | n (%) | Mean (SD); Median; Range |
|---|
| Age (Years) |
| ≤20 | 7 (6.9) | Mean (SD): 43.35 (13.46) Median: 42.00 Range: (16-84) |
| 21-30 | 11 (10.9) |
| 31-40 | 22 (21.8) |
| 41-50 | 31 (30.7) |
| 51-60 | 21 (20.8) |
| ≥61 | 9 (8.9) |
| Religion |
| Hindu | 94 (93.1) | |
| Muslim | 7 (6.9) |
| Caste |
| General | 89 (88.1) | |
| SC | 11 (10.9) |
| OBC | 1 (1.0) |
| Marital status |
| Married | 86 (85.1) | |
| Never married | 15 (14.9) |
| Education |
| Up to primary (Primary school completion certificate, up to class VII) | 51 (50.5) | |
| Above primary (Middle school completion certificate and above, class VIII and above) | 50 (49.5) | |
| Per capita income (Modified BG Prasad Scale, 2018, Rupees/Month) |
| Class I (6574 and above) | 6 (5.9) | Mean (SD): 2366.17 (1448.61) Median: 2000.00 Range: (500-7000) |
| Class II (3287-6573) | 42 (41.6) |
| Class III (1972-3286) | 38 (37.7) |
| Class IV (986-1971) | 9 (8.9) |
| Class V (985 and below) | 6 (5.9) |
| Substance abuse |
| Absent | 39 (38.6) | |
| Present* | 62 (61.4) |
| *27 persons smoked, 22 persons consumed smokeless tobacco, 15 persons were addicted to alcohol. |
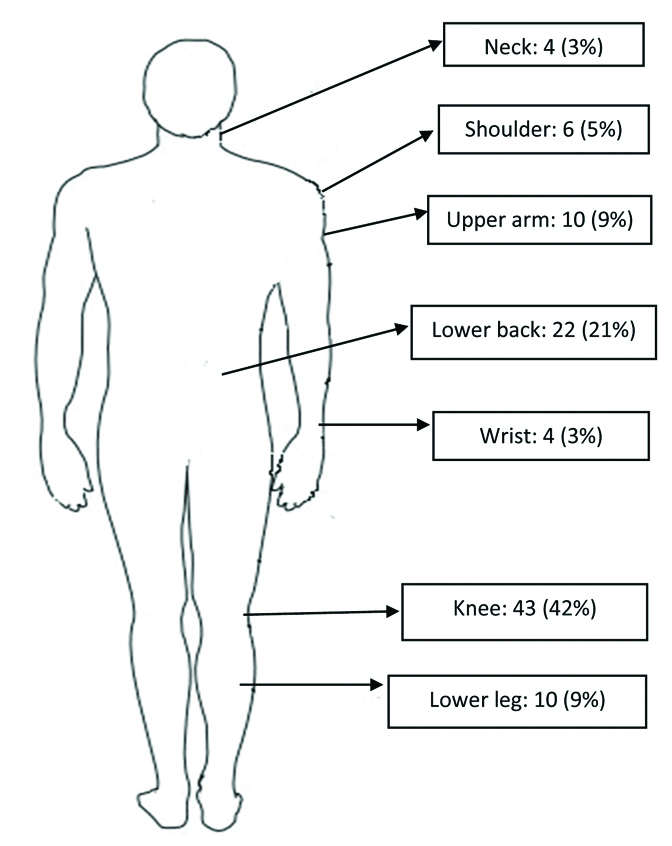
[Table/Fig-3] It can be seen that 31.8% study participants worked for 16 to 25 years. Around one third of the study participants were involved in machine handling and majority had no formal training. Around one fourth (26.7%) workers were working for all the seven days in a week. [Table/Fig-4] In the current study, 42% study participants had knee discomfort and 21% had lower back pain according to CMDQ tool.
Occupational differentials of automobile garage workers (n=101).
| Characteristics | n (%) | Mean (SD); Median; Range |
|---|
| Duration of job (Years) |
| ≤5 | 25 (24.7) | Mean (SD): 16.92 (12.50)Median: 18.00 Range: (0.50-50) |
| 6-15 | 22 (21.7) |
| 16-25 | 32 (31.8) |
| 26-35 | 15 (14.9) |
| ≥36-45 | 7 (6.9) |
| Type of work |
| Body repair | 35 (34.8) | |
| Machine handling | 38 (37.5) |
| Painting | 28 (27.7) |
| Formal training |
| Present | 11 (10.9) | |
| Absent | 90 (89.1) |
| Working days/Week |
| 5 | 5 (5.0) | Mean (SD): 6.21 (0.52) Median: 6.00 Range: (5-7) |
| 6 | 69 (68.3) |
| 7 | 27 (26.7) |
| Working hours/day |
| 7 | 4 (3.9) | Mean (SD): 9.15 (1.63) Median: 8.50 Range: (7-16) |
| 8-9 | 62 (61.4) |
| 10-11 | 19 (18.8) |
| ≥12-14 | 16 (15.9) |
| Duration of work (in hours) per week |
| 35-45 | 4 (3.8) | Mean (SD): 56.99 (11.69) Median: 54.00 Range: (35-96) |
| 46-55 | 48 (47.6) |
| 56-65 | 30 (29.9) |
| 66-75 | 10 (9.9) |
| ≥76 | 9 (8.8) |
| Overtime job |
| Yes | 3 (2.9) | |
| No | 98 (97.1) |
| Carrying heavy load |
| Yes | 38 (37.6) | |
| No | 63 (62.4) |
Distribution of body area wise musculoskeletal discomfort according to CMDQ tool (N=101) (multiple response).
From [Table/Fig-5] it can be seen that, 26.7% study participants had mild discomfort, 31.8% had moderate discomfort and 14.8% study participants had severe discomfort and all together 73.3% or 74 study participants among 101 study participants had discomfort. Around half of the workers (46.6%) had moderate and severe discomfort. The mean CMDQ score was 4.72 with a wide range of 0-35.50. [Table/Fig-6] It is observed that MSD was significantly associated with increasing age moderate to severe. It was also associated with increasing duration of working hours per week and substance abuse. But the moderate to severe MSD was not significantly associated with education, per capita income, duration of job and duration of working hours per day.
Distribution of the study participants according to attained Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) score (N=101).
| Discomfort | CMDQ score | n (%) | Discomfort or severity of discomfort | |
|---|
| Absent | 0 | 27 (26.7) | No discomfort | Mean (SD): 4.72 (6.59) Median: 1.50 Range: [00.00-35.50] |
| Present | 1.5 | 27 (26.7) | Mild discomfort |
| 1.6-10.5 | 32 (31.8) | Moderate discomfort |
| >10.5 | 15 (14.8) | Severe discomfort |
Univariate and multivariable logistic regression showing factors associated with moderate to severe musculoskeletal discomfort (N=101).
| Characteristics | Moderate to severe musculoskeletal discomfort present | OR (95% CI) | AOR (95% CI) |
|---|
| Number (%)# Median (IQR)$ |
|---|
| Age (Years) ← | | 42 (35, 55) | 1.03 (1.01-1.05)* | 1.042 (1.003-1.81)* |
| Education | Up to primary | 27 (54.7) | 1.69 (0.77-3.61) | |
| Above primary | 20 (42.6) | 1 | |
| Per capita income (Rs/month) | ≤2000 | 28 (59.6) | 1.09 (0.50-2.40) | |
| >2000 | 19 (40.4) | 1 | |
| Substance abuse | No | 13 (27.7) | 1 | |
| Yes | 34 (72.3) | 1.06 (1.03-1.83)* | 1.01 (0.34-3.89) |
| Duration of job (Years) | ≤18 | 22 (46.8) | 1 | |
| >18 | 25 (53.2) | 1.32 (0.61-2.89) | |
| Working hours/day | ≤8 | 21 (44.7) | 1 | |
| >8 | 26 (55.3) | 1.43 [0.65-3.15] | |
| Duration of work (hours per week) ← | | 56 (48,70) | 1.04 (1.001-1.09)* | 1.043 (1.01-2.01)* |
*p-value ≤0.05; ⊑: increasing
#Categorical variables were presented with number (%)
$Continuous variables were presented with median (IQR)
CI: Confidence interval; OD: Odds ratio; IQR: Interquartile range; AOR: Adjusted odds ratio
In multivariable logistic regression, the increasing age and increasing duration of working hours per week retained their significance. (Hoshmer and Lemeshow test was not significant so, the model fitting was good. Cox & Snell R Square were 0.10 and Nagelkerke R2 was 0.116 for the model. A 10% to 11.6% variability of dependent variable was explained by the model as revealed by Cox and Snell and Nagelkerke R2. So, the model fitting was satisfactory and the model was able to explain variability of dependent variable).
Discussion
The proportion of MSD among automobile garage workers was quite high in the current study and 73.3% study participants had MSD. Total 46.6% study participants had moderate to severe MSD according to CMDQ tool. Nearly half (42%) study participants had knee discomfort and 21% study participants had lower back pain. The discomfort was significantly associated with increasing age and increasing duration of working hours per week in univariate and multivariable logistic regression. A study was done by Thangaraj S and Shireen N, in Bangalore among 150 automobile workers. The proportion of MSD was 62% and no specific tool was used in the study for collection of data on MSD. In the current study, 73.3% study participants had discomfort in musculoskeletal system, which is higher than the findings by Thangaraj S et al., [11]. A study done by Philip M et al., among 106 automobile workers in Vellore showed that 44.3% participants reported muscle and joint pains and no specific tool was used to collect musculoskeletal data. Therefore, the finding is quite lower than the current study [12].
A study was done by James C and Kulkarni DVA, in Pune, among 100 automobile workers with ≥5 years of experience [6]. The proportion of MSD was 84%. Nordic questionnaire was used to collect data. The finding of MSD was higher than the current study. This may be due to different study settings like different inclusion criteria and exclusion criteria. A study done by Singh LP and Singh G, in Punjab reported MSD in 58% of the population and no specific tool was used to collect musculoskeletal data [1]. MSD was significantly associated with age and duration of the job of the study participants. The proportion of MSD was high (73.3%) and knee was the common site for MSD in the current study.
Akter S et al., in Dhaka, Bangladesh conducted a study among 100 automobile garage workers [5]. The short version of Dutch Musculoskeletal Questionnaire was used to determine the proportion of MSD. The proportion of MSD during the last 12 months was reported as 77%. The most affected body parts were lower back (67%) then the hip (53%). MSD was significantly associated with duration of job and working hours per day [5]. The findings were quite different from the current study. In the current study, knee (42%) was mostly affected MSD site and increasing age and working hours per week was significantly associated with MSD. These discordant findings were seen in this from the current study. A study by Sukhriah A et al., in Malaysia among 150 automobile garage workers found MSD in 86.0% of the population [4]. Nordic questionnaire was use to collect data. The proportion of MSD was 73.3% in the current study which was quite lower than the study in the discussion.
Limitation(s)
The study was cross-sectional in nature so the causal association between MSD and occupational determinants could not be established. The CMDQ was a self-reported questionnaire so there were the chances of over or under reporting of the MSD but the chance of recall bias was low with CMDQ because the recall period was seven days. There were no clinical examination or diagnostic procedure was done to confirm the MSD due to resource constrains. CMDQ is only a screening tool, not a diagnostic tool.
Conclusion(s)
The proportion of MSD among automobile garage workers was quite high in the current study and knee and low back was the most affected site. MSD showed a significant association with increasing age and increased duration of working hours per week. Though the current study could not establish the causal relationship between MSD and occupational exposure due to its cross-sectional design but application of the easy to administer CMDQ tool for early detection of MSD among auto mobile garages will definitely help occupational health specialists for timely screening of MSD among automobile workers. The CMDQ tool may be used during preplacement examination and periodic medical examination of automobile workers for screening of MSD, if possible. The awareness generation among all the stakeholders of automobile garage is very much needed to lead healthy MSD free life.
*p-value ≤0.05; ⊑: increasing
#Categorical variables were presented with number (%)
$Continuous variables were presented with median (IQR)
CI: Confidence interval; OD: Odds ratio; IQR: Interquartile range; AOR: Adjusted odds ratio