Population based cancer assessment provides statistics about incidence, mortality, risk factors and disease burden associated with various diseases within a defined population of a specific area, over a fixed period of time [1,2]. An increased incidence of cancer cases in southern Punjab had been reported which led to the initiation of population based cancer registry and Punjab cancer atlas like projects under National Cancer Registry Program [3,4]. As per cancer atlas Punjab state data for year 2012-2013, age adjusted rates of cancer incidence per 1,00,000 population in males in Punjab was 41.5-91.5 compared to other regions of India (other than Punjab) where the rate was 43.7-273.4. In females, adjusted rates of cancer incidence per 1,00,000 population was 59.3-128.8 compared to other regions of India (other than Punjab) where the rate was 51.6-227.8 [5]. Incidence of disease over a period of time, disease pattern and site and its burden on community are important factors in management of cancer [4]. The projected incidence of patients with cancer for the year 2020 in India in males is 679,421 and in females is 712,758 [6]. The current study was done at a tertiary care hospital in Punjab catering a large part of Punjab to know about the disease burden of cancer and find out the leading cause.
Materials and Methods
A retrospective observational study was conducted to assess the incidence of various malignancies diagnosed on histopathology in patients coming to Government Medical College and Rajindra Hospital, Patiala, Punjab, a tertiary level hospital catering a large area of Punjab from January 2006 to December 2015. A careful scrutiny of the ten years record of the histopathologically diagnosed cases of various malignancies was done. All cases diagnosed to be of a malignant disease on histopathology over the above mentioned time period were included in the study. The data gathered was compiled and tabulated on the yearly basis and analysed in detail to calculate the accurate incidence of each and every malignant disease diagnosed in patients presenting to our hospital by the measure of relative frequency.
Statistical Analysis
All the data was compiled in microsoft excel sheet and discriptive statistics were tabulated and analysed.
Results
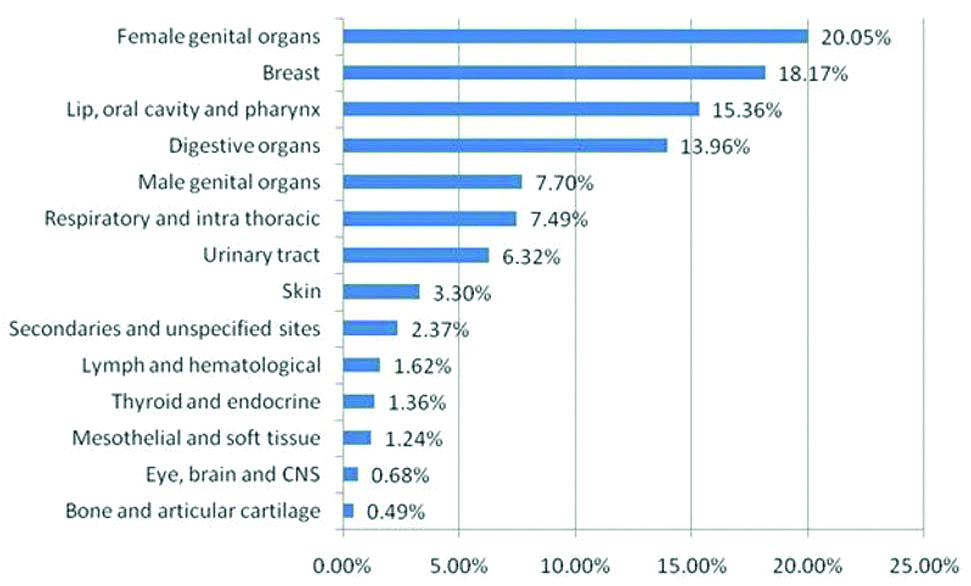
A total of 4270 cases were included in the study. This was the total number of patients of various malignancies detected over a period of ten years on histopathology. Percentage wise various malignancies seen on the histopathology report have been tabulated below as [Table/Fig-1].
Incidence of histopathologically diagnosed malignancies at a tertiary hospital over a period of ten years 2006-2015.
Gender wise change in trends of malignancies in patients over the period of ten years showed that out of the total 1929 were males i.e., 45.18% and 2341 were females i.e., 54.82% [Table/Fig-2].
Gender wise change in trends of malignancies in patients.
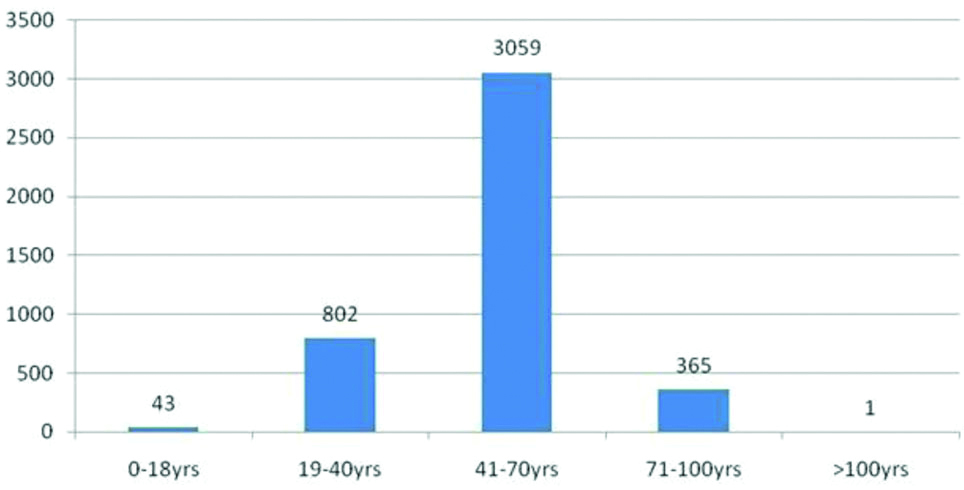
In age group 0-18 there were 43 (1.01%) patients. In age group 19-40 years, there were 802 (18.78%) patients. In age group 41-70 years, there were 3059 (71.65%) patients while in age group 71-100 years, there were 365 (8.55%) patients. Only 1 (0.0002%) patient was seen in age group above 100 years [Table/Fig-3].
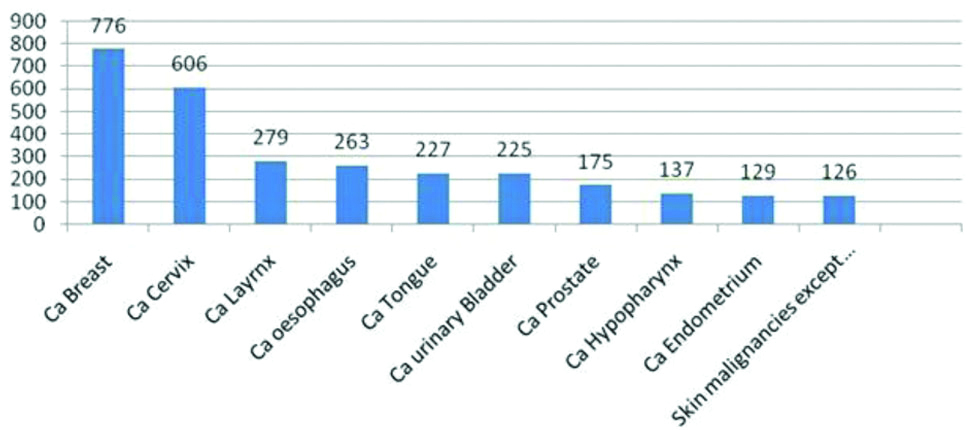
Age group wise total No. of cases of malignancies. Malignancies with maximum no. of incidence in ten years.
Maximum number of incidence in ten years was seen in carcinoma breast followed by carcinoma cervix and carcinoma larynx. This was followed by carcinoma oesophagus, carcinoma tongue, carcinoma urinary bladder and carcinoma prostate. Carcinoma hypopharynx, carcinoma endometrium and carcinoma of skin other than melanoma were next in line [Table/Fig-4].
Incidence of various malignancies over ten years.
Ca: Carcinoma
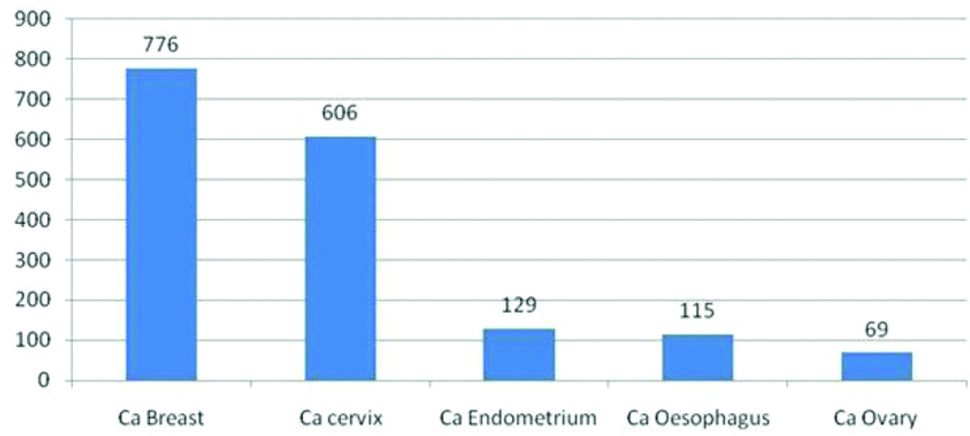
Malignancies with maximum incidence in females in ten years was Ca Breast followed by Ca Cervix, Ca endometrium, Ca oesophagus and Ca ovary [Table/Fig-5].
Maximum incidence of malignancies in females in ten years.
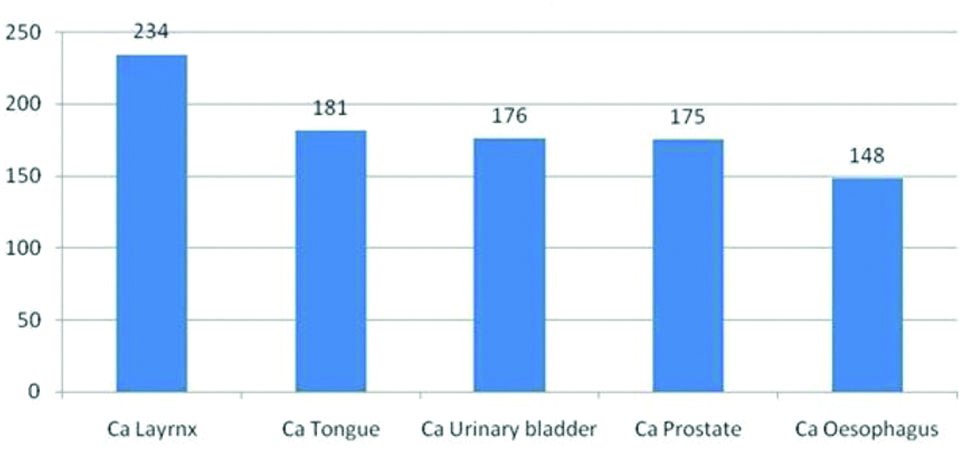
Malignancies with maximum incidence in males were Ca Larynx, Ca tongue followed by Ca urinary bladder, Ca prostate and Ca oesophagus [Table/Fig-6].
Maximum incidence of malignancies in males in ten years.
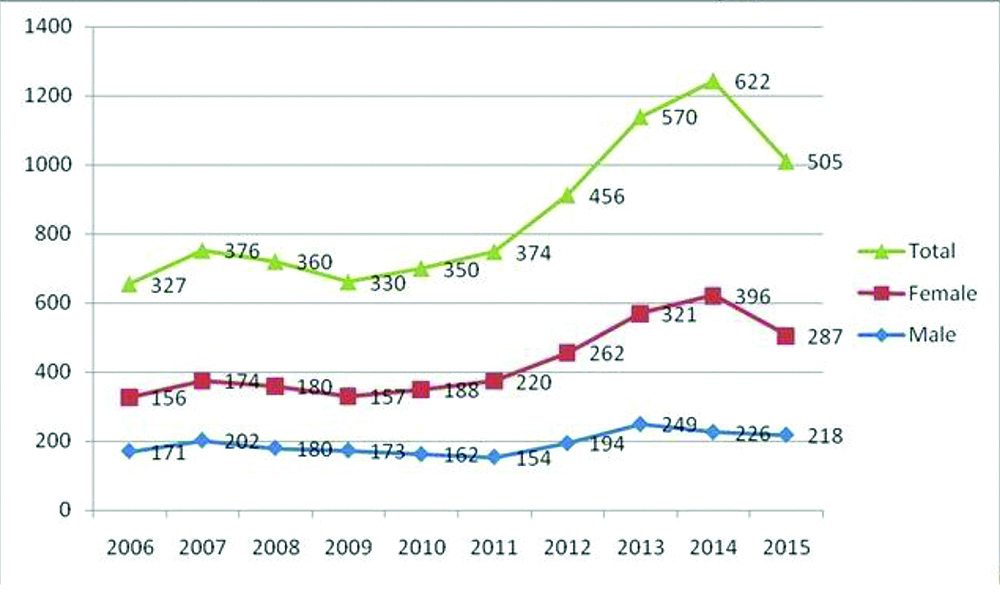
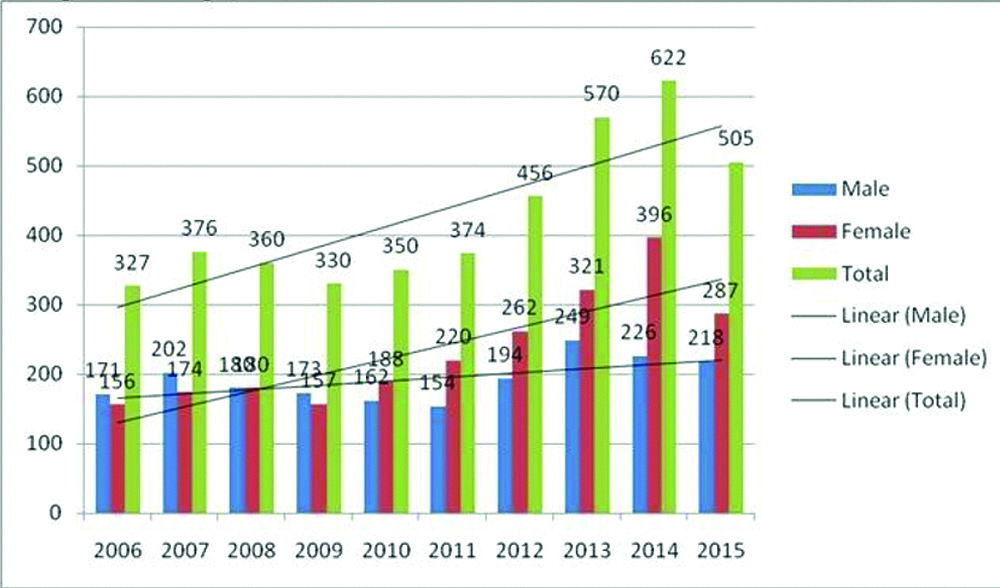
Over the ten years there was seen an increase in number of cases of malignancies in both males and females has been seen and hence, increase in total number of malignancies [Table/Fig-7].
Year wise total number of cases of malignancies and sex wise change in trends in malignancies over the years. Year wise trends of various malignancies.
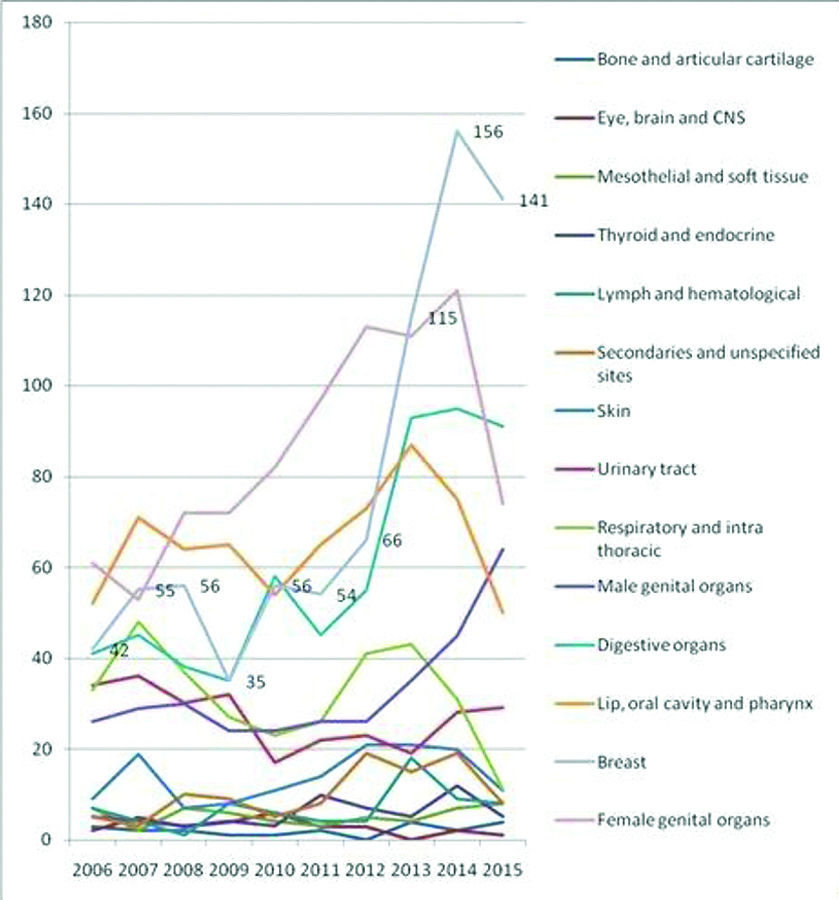
Among all the malignancies, the maximum increase has been seen in breast cancer, cancers of male and female genital organs, cancers of digestive organs and cancers of lip, oral cavity and pharynx [Table/Fig-8].
Year wise trends of various malignancies.
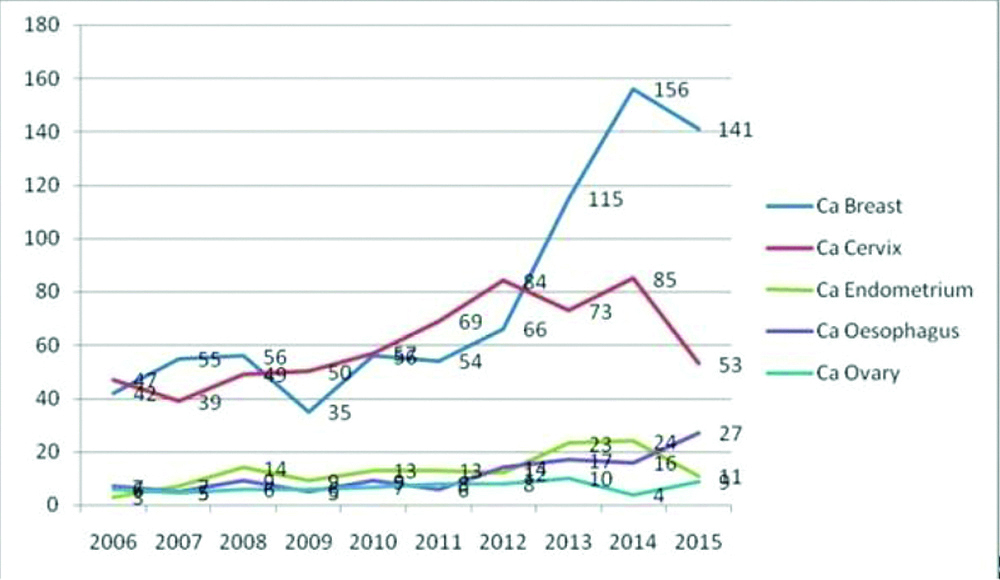
There has been an increase in the number of malignancies in females namely Ca breast, Ca Cervix, Ca endometrium, Ca oesophagus and Ca ovary. A trend of sharp increase in the number of Ca breast cases has been observed over the period of ten years [Table/Fig-9].
Trends in increase in malignancies in females over ten years.
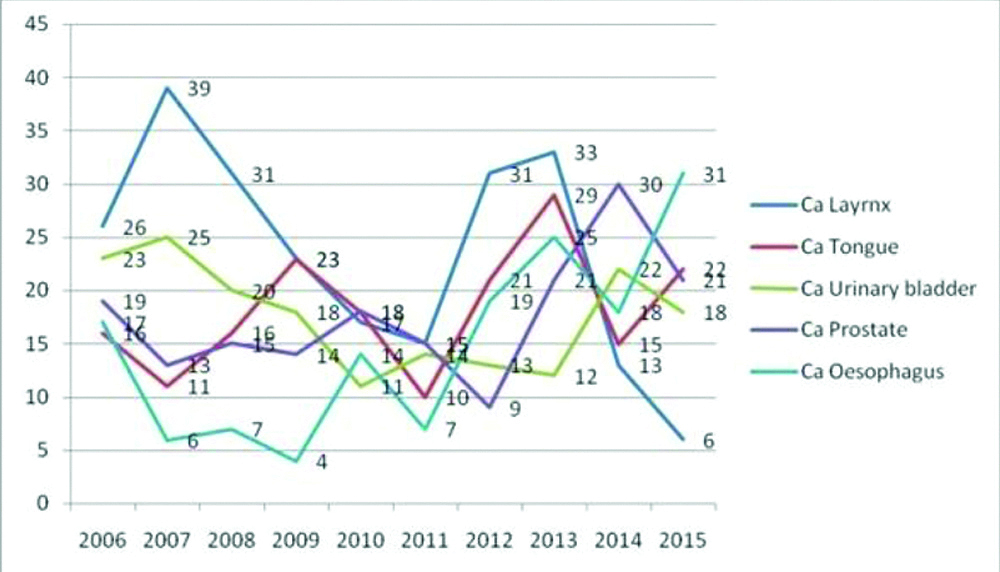
There has seen an increase in the number of malignancies in males namely Ca larynx, Ca tongue, Ca urinary bladder, Ca prostate and Ca oesophagus. Number of cases of Ca oesophagus and Ca prostate has been in an increasing trend over the period of ten years but number of cases of Ca larynx has been observed to be in decreasing trend during the same time period [Table/Fig-10].
Trends in increase in malignancies in males over ten years.
Discussion
The incidence of estimated cancer cases in India were 548000 in 1990 which increased to 1069000 in 2016 India State level disease burden initiative cancer collaborators [7]. Based on the National Cancer Registry Programme (NCRP) data, an increase in the new cancer cases from 936908 in 2010 to 1044650 by 2020 is expected. This may be due to expanding population and increase in life expectancy of the people. Tobacco being the upfront identified cause of cancer Takiar R et al., [8]. Alcohol, tobacco, toxic industrial waste, pesticides and radiation are the major cause of high incidence of cancer in Punjab, Indian Council of Medical Research (ICMR) [9]. Ten years lifetime prevalence had been estimated in cancer patients after the incidence according to a study by Kaur G et al., [10]. Cancer lead to 5% of the total disability adjusted life years and 8.3% of total deaths in India in 2016, which is an increase of 90.9% and 11.2%, respectively since 1990 GBD 2016 Cancer collaborators, Aggarwal R et al., [11,12].
In this study, out of 4270 histopathologically diagnosed cases of various malignancies, there was an increase in the total number of cases in both males as well as females. There were 1929 males i.e., 45.18% and 2341 were females i.e., 54.82% thus, showing more incidence in females which is comparable with results with study by Bal MS et al., [4] but in contrast to study by Samvasivaiah K et al., in Andhra Pradesh where 53.99% were males and 46.01% were females [13].
Leading causes of malignancy were the cancers of the female genital organs (ICD 10 C51-C58) i.e., 20.05%, followed by breast (ICD 50) cancer i.e., 18.17% and cancers of lip, oral cavity and pharynx (ICD 10 C00-C14) i.e., 15.36%. The fourth and the fifth on list are the malignancies of the digestive organs (ICD 10 C15-C16) and respiratory and intra-thoracic organs (ICD 10 C30-C39) i.e., 13.96% and 7.49%, respectively. These were followed by the malignancies of the male genital organs (ICD 10 C60-C63) i.e., 7.70% and the malignancies of the urinary tract i.e., 6.32% as seen in [Table/Fig-1]. As per India state level disease burden initiative cancer collaborators article [7] the leading types of cancer in India in 2016 were stomach cancer, breast cancer, lung cancer, lip and oral cavity cancer, pharynx cancer, colon and rectum cancer. Breast, cervical and stomach cancer were the leading cancers in females while, lung cancer, lip and oral cavity, pharynx cancer and stomach cancer were the leading cancers in males [6]. The results of this study are comparable with the present study.
In this study, malignancy with maximum incidence in females was Ca breast followed by Ca cervix, Ca endometrium, Ca oesophagus and Ca ovary in the present study which is comparable with the article by India state level disease burden initiative cancer collaborators [7] where breast, cervical and stomach cancer were responsible for highest disability adjusted life years in 2016, with review of evidence from Punjab cancer atlas by Labani S et al., cancers of breast, cervix, ovary and oesophagus were the most common in females [5] while article by Bal MS et al., showed Ca breast, cervix and ovary were the leading cause in females [4]. As per study by Puri S et al., females had carcinoma breast followed by carcinoma cervix and carcinoma ovary as the most common cancers [14]. Findings in all these studies are comparable with this study.
In this study, malignancies with maximum incidence in males were Ca Larynx, Ca tongue followed by Ca urinary bladder, Ca prostate and Ca oesophagus. Study by India state level disease burden initiative cancer collaborators [7] showed cancers of lung, lip and oral cavity, other pharynx and stomach cancer were responsible for highest disability adjusted life years in 2016. In review of evidence from Punjab cancer atlas by Labani S et al., carcinoma of lung, oesophagus, mouth, tongue, prostate were the most common causes of cancer [5] while study by Bal MS et al., showed carcinoma of colon, oesophagus and tongue were the leading causes of cancer [4]. As per article by Puri S et al., males had carcinoma lung, followed by carcinoma secondaries and carcinoma oesophagus as the most common cancers [14]. The results in all these studies are comparable, though not completely which may be because of variation in eating habits, geographical distribution, socio-economic status, prevalence of infectious diseases in that region, practice of use of smoking, tobacco chewing, alcohol intake, opiods and other and substance abuse in different regions.
Maximum number of patients i.e., 3059 (71.65%) were from the age group 41-70 years in this study. This is comparable with articles by Bal MS et al., and article by RD Smith and MK Mallath [4,15].
A trend of sharp increase in the number of Ca breast cases has been observed over the period of ten years which may be because of decrease in total number of cumulative lactational years due to one/two child norm in Punjabi families which is protective against breast cancer, and increased awareness created by the government through various cancer screening programmes. Number of cases of Ca oesophagus and Ca prostate have been in an increasing trend over the period of ten years which may be due to increased incidence of obesity, increased intake of western diet and fatty food, increased longevity, but number of cases of Ca larynx has been observed to be in decreasing trend during the same time period may be due to more awareness about effects of smoking and tobacco chewing and early detection.
Limitation(s)
In the present study some malignancies involving brain, heart have not been included as histopathology specimen were not received due to lack of functional superspeciality departments/infrastructure at the facility where the study had been conducted. Only those patients in whom the cancer was diagnosed at our hospital were included in the study.
Conclusion(s)
Cancer leads to heavy emotional and economic burden for an individual and for the state as a whole. Educating people about lifestyle changes, healthy eating habits, reducing the use of pesticides and exposure to toxic chemicals is required. Creating awareness and promoting the public about physical activities, exercise and yoga in daily routine and restraining the use of smoking and alcohol and maintaining sexual health is very important. On the other hand improving cancer screening, early detection, diagnosis and treatment of cancer for all individuals from all parts of the society is the utmost need of the hour. Regular scrutiny of the records like in this study is required to raise an alarm to curb, cure and manage the deadly disease such as cancer in a satisfactory and cost-effective manner to decrease the economic burden of state.