An Infrequent Adenosarcoma Mimicking other Uterine Rhabdoid Tumours
B Archana1, Sandhya Sundaram2, Lawrence D Cruze3, KS Rajeshwari4
1 Demonstrator, Department of Pathology, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India.
2 Professor, Department of Pathology, Sri Ramachandra Institute of Higher Education and Research, Porur, Tamil Nadu, India.
3 Associate Professor, Department of Pathology, Sri Ramachandra Institute of Higher Education and Research, Porur, Tamil Nadu, India.
4 Professor, Department of Obstetrics and Gynaecology, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Sandhya Sundaram, Professor, Department of Pathology, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai-600116, Tamil Nadu, India.
E-mail: sandsrid@gmail.com
Uterine sarcomas are relatively rare and account for only 1-3% of all malignancies in the Female Genital Tract (FGT). Adenosarcomas of the uterus are uncommon accounting for only 5% of uterine sarcomas. They are considered less recurrent and less metastatic. However, those with sarcomatous overgrowth and heterologous differentiation are very rare, considered aggressive and need to be differentiated histologically from other sarcomas that mimic the same clinically and histologically. In the index case, a 50-year-old female presented with symptoms of pain in the abdomen and bleeding per vagina. Magnetic Resonance Imaging (MRI) showed a large polypoid solid mass in the endometrium, suggestive of a sarcoma. Positron Emission Tomography (PET) scan showed an Fluorodeoxyglucose (FDG) avid lesion in the endometrial cavity (SUV max-13.33). Total abdominal hysterectomy and salpingooophorectomy was performed. Histology showed a biphasic tumour (benign glands and malignant mesenchymal component) with rhabdomyoblastic differentiation and sarcomatous overgrowth. Presence of rhabdoid cells raises the possibility of other sarcomas with these features making the diagnosis challenging. Immunohistochemistry (IHC) confirmed it to be a high grade adenosarcoma with sarcomatous overgrowth. Desmin positivity was noted in the rhabdoid cells. Majority cases of adenosarcoma are low grade, the index case was however high grade with presence of heterologous elements and sarcomatous overgrowth. Neither radiology nor clinical features can reliably differentiate adenosarcomas from other uterine sarcomas. A definitive diagnosis can be made by understanding the overlapping morphological features and correlate it with IHC to reliably differentiate it with other similar looking uterine sarcomas.
Biphasic, Sarcoma, Uterus
Case Report
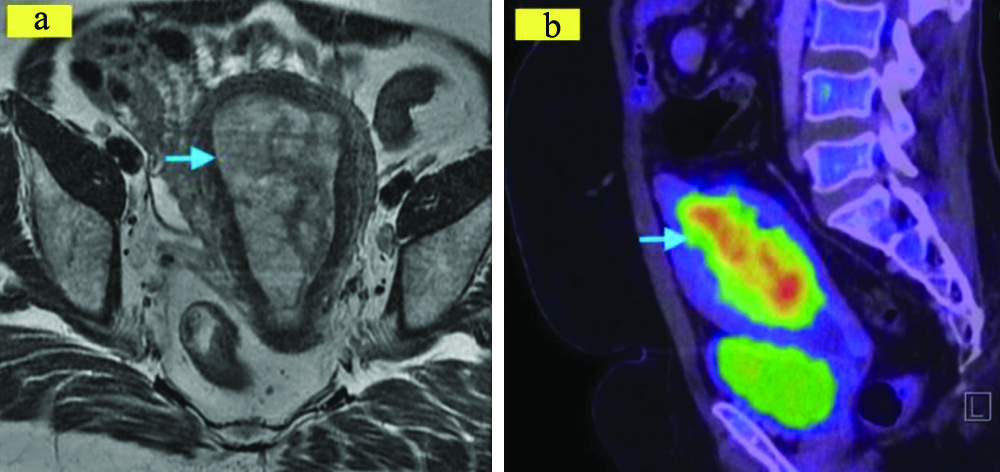
A 50-year-old female presented to the Gynaecology Out-Patient Department with symptoms of pain abdomen associated with bleeding per vagina for one month. She had a known history of diabetes and hypertension since three years. She had a past history of four normal vaginal deliveries and sterilisation and no significant family history. On general examination, her vitals were stable, abdomen soft and nontender. On per vaginal examination, the exact size of the uterus could not be made out and fornices were free. MRI suggested an irregular mass lesion occupying the entire endometrial cavity extending into the upper part of the cervix [Table/Fig-1a]. Myometrium and serosa showed normal signal intensity. Endometrial biopsy done suggested a sarcoma with rhabdoid features. PET scan revealed an FDG avid lesion in the endometrial cavity measuring 86 mm/40 mm with an SUV max of 13.33 with no evidence of peri-serosal extension [Table/Fig-1b]. Few enlarged lymph nodes were seen involving left external iliac, para aortic and aortocaval locations which were however not significant. The clinical and radiological diagnosis was that of an Endometrial sarcoma.
a) MRI showed large polypoid mass with heterogeneous solid component; b) PET scan showing FDG avid lesion in the endometrial cavity (SUV max-13.33).
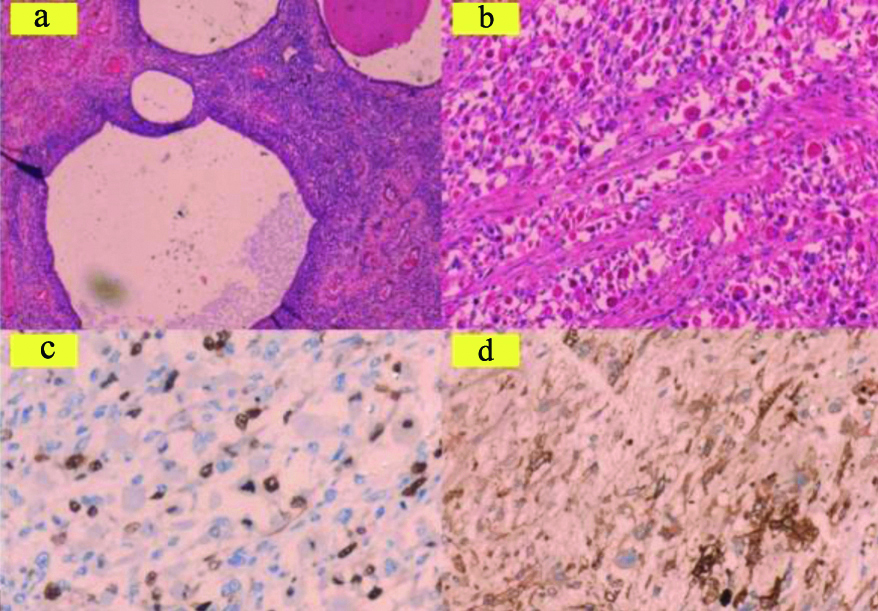
The patient underwent total abdominal hysterectomy with bilateral salpingooophorectomy and pelvic node dissection. Grossly, a large polypoidal grey white soft mass was seen measuring 9/5/4 cm in the endometrial cavity extending into the lower uterine segment [Table/Fig-2]. The lesion seemed to involve less than 50% of the myometrium. It was soft, fleshy with areas of haemorrhage and necrosis (corresponding to sarcomatous overgrowth). Microscopically, the lesion was made up of entrapped, few, benign glands in a malignant stroma [Table/Fig-3a]. The sarcoma component comprising of more than 25% of the tumour with no associated epithelium indicated a ‘sarcomatous overgrowth’. Scattered throughout in the stroma was heterologous component consisting of numerous atypical rhabdoid cells composed of abundant eosinophilic cytoplasm and peripherally pushed nucleus with visiblecross striations in the cytoplasm [Table/Fig-3b]. Lympho-vascular invasion was noted, no nodal metastasis was seen. A differential diagnosis of adenosarcoma with rhabdoid features, Leiomyosarcoma (LMS) with rhabdoid features, rhabdomyosarcoma and carcinosarcoma was considered. IHC was done to rule out other tumours of the uterus that show rhabdoid differentiation. IHC showed positivity for vimentin, focal positivity for desmin and smooth muscle actin. Myogenin was positive in the rhabdoid cells [Table/Fig-3c], CD10 was focally positive in the intervening stromal cells [Table/Fig-3d], cytokeratin 7 was positive in the entrapped glandular epithelium. A final diagnosis of uterine adenosarcoma with sarcomatous overgrowth was made. The patient has been on regular follow-up for a period of six months postsurgery and is doing well currently.
Gross image of the uterus showing a large polypoidal mass lesion involving the entire uterus projecting into the cervical canal. The lesion was solid, soft, tan colour with focal areas of haemorrhage and necrosis.

a) H&E,200x, Benign entrapped glands in adenosarcoma; b) H&E,100X, Sarcomatous stroma with rhabdomyoblastic cells (heterologous component); c) IHC,100X, Myogenin positive in the rhabdoid cells; d) IHC,100X,CD 10 positive in the stroma.
Discussion
Uterine sarcomas account for 1-3% of all malignancies in the FGT [1] and 3-7% tumours of the endometrium. Globally adenosarcomas comprise to less than 8% of the uterine sarcomas [2]. Even rarer are adenosarcomas with sarcomatous overgrowth characterised by presence of sarcomatous component in at least 25% of the tumour area. Mullerian adenosarcomas are rare malignancies of the FGT characterised by admixture of benign glands and malignant mesenchymal component [3]. They occur commonly in perimenopausal and postmenopausal women [4], similar to what authors observed in present case. Patients present commonly with symptoms of abnormal uterine bleeding. Although the uterus is the most frequently affected site, they may arise in the cervix, vagina, ovary and fallopian tube [4,5].
Theories about their histogenesis have been proposed and suggest that epithelial and mesenchymal components arise independently from common stem cells [3]. Rarely, adenosarcomas following tamoxifen treatment for breast cancer have been reported as well as radiation induced sarcomas [6]. Macroscopically, they are usually exophytic polypoidal, solid and cystic ranging from 5-50 cm. Microscopically, they are biphasic tumours with a benign glandular and malignant mesenchymal component. Majority tumours have low grade mesenchymal component and present at stage 1 disease. Fewer cases, like the index case, have reported high grade grade histology with a sarcomatous overgrowth pattern that carries a poorer prognosis [7]. A case of adenosarcoma with ovarian sex cord like differentiation has been reported in the literature [1]. It is important for a pathologist to excise caution in reporting uterine sarcomas, frame a differential diagnosis, understand the therapeutic implications and make a definitive diagnosis. The presence of sarcomatous overgrowth is associated with higher staged tumours and a high recurrence rate of up to 70% [8].
Prognosis of adenosarcomas is dependent on various factors like sarcomatous overgrowth, presence of heterologous elements (rhabdomyoblastic, osseous differentiation), deep myometrial invasion and extrauterine extension [5,7]. The International Federation of Gynaecology and Obstetrics (FIGO) staging is adopted for adenosarcomas based on extent of myometrial invasion, extrauterine spread, nodal and distant metastasis [4,7]. Adenosarcomas have to be differentiated microscopically with other stromal sarcomaslike endometrial stromal sarcoma, LMS and Rhabdomyosarcomas (RMS) (all have only stromal component) and carcinosarcoma (malignant epithelial and mesenchymal components). CD10 is a common immunophenotypic feature of neoplastic mesenchymal cells of Mullerian origin, its significance needs to be validated by further studies for differentiating sarcomas [3].
Similar to that seen in the index case, rhabdoid differentiation may also be seen in LMS, RMS, carcinosarcomas and adenosarcomas [9]. Their differentiation may be difficult and misleading. Presence of rhabdoid features indicates the aggressive nature of the tumour. These tumours can be differentiated by morphology and the pattern of IHC expression. Desmin and myogenin are known to be positive in rhabdoid cells. In LMS, diffuse Smooth Muscle Actin (SMA) positivity is noted, RMS shows dense myogenin positivity in all cells. Adenosarcomas demonstrate a mixed positivity of desmin and myogenin intermixed with CD10 positivity in the neoplastic stromal cells. Rhabdoid features need to be documented in the report as treatment may have to be aggressive [10].
Multiple genetic abnormalities have been observed in the mesenchymal component of the tumour. The PI3K-AKT-PTEN pathway mutation have been reported in the literature. ATRX, TP53, TERT mutations have also been noted [8]. Overall survival is 100% with standard of care treatment for adenosarcomas while it is 20% for adenosarcoma with sarcomatous overgrowth which has increased propensity to recur [4,11]. Chemotherapy is proven to be effective in cases with sarcomatous overgrowth, however limited evidence exists for the role of hormonal therapy [4].
Conclusion(s)
Uterine adenosarcomas are histological diverse sarcomas that continues to interest the pathologist. Presence of rhabdomyoblastic differentiation is seen in other sarcomas that challenges the pathologist in making a definitive diagnosis. Presence of sarcomatous overgrowth with rhabdoid features in adenosarcomas must alert the clinician to institute aggressive treatment as it indicates a worst outcome. The lack of consensus in risk factors and adjuvant treatment in high grade adenosarcomas warrant further studies in this area.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 28, 2020
Manual Googling: Jan 06, 2021
iThenticate Software: Jan 23, 2021 (7%)
[1]. Ulker V, Yavuz E, Gedikbasi A, Numanoglu C, Sudolmus S, Gulkilik A, Uterine adenosarcoma with ovarian sex cord-like differentiation: A case report and review of the literatureTaiwan J Obstet Gynecol 2011 50(4):518-21.10.1016/j.tjog.2011.10.02222212329 [Google Scholar] [CrossRef] [PubMed]
[2]. Prat J, Mbatani ’Nomonde, Uterine sarcomasInt J Gynecol Obstet [Internet] 2015 131:105-10.10.1016/j.ijgo.2015.06.00626433666 [Google Scholar] [CrossRef] [PubMed]
[3]. Mikami Y, Hata S, Kiyokawa T, Manabe T, Expression of CD10 in malignant müllerian mixed tumours and adenosarcomas: An immunohistochemical studyMod Pathol 2002 15(9):923-30.10.1097/01.MP.0000026058.33869.DB12218209 [Google Scholar] [CrossRef] [PubMed]
[4]. Pinto A, Howitt B, Uterine AdenosarcomaArch Pathol Lab Med 2016 140(3):286-90.10.5858/arpa.2014-0523-RS26927725 [Google Scholar] [CrossRef] [PubMed]
[5]. Seagle BLL, Falter KJ, Lee SJ, Frimer M, Samuelson R, Shahabi S, Mullerian adenosarcoma of the cervix: Report of two large tumours with sarcomatous overgrowth or heterologous elementsGynecol Oncol Reports 2014 9:7-10.10.1016/j.gynor.2014.04.00525426405 [Google Scholar] [CrossRef] [PubMed]
[6]. Carvalho FM, Carvalho JP, Motta EV, Souen J, Müllerian adenosarcoma of the uterus with sarcomatous overgrowth following tamoxifen treatment for breast cancerRev Hosp Clin Fac Med Sao Paulo 2000 55(1):17-20.10.1590/S0041-8781200000010000410881074 [Google Scholar] [CrossRef] [PubMed]
[7]. Wang B, Yang HD, Shi XH, Li H, Advanced uterine adenosarcoma with sarcomatous overgrowth in a young woman: A case reportMedicine 2019 98(47)10.1097/MD.000000000001811931764852 [Google Scholar] [CrossRef] [PubMed]
[8]. Piscuoglio S, Burke KA, Ng CK, Papanastasiou AD, Geyer FC, Macedo GS, Uterine adenosarcomas are mesenchymal neoplasmsJ Pathol [Internet] 2016 238:381-88.10.1002/path.467526592504 [Google Scholar] [CrossRef] [PubMed]
[9]. Anh Tran T, Holloway RW, Metastatic leiomyosarcoma of the uterus with heterologous differentiation to malignant mesenchymomaInt J Gynecol Pathol 2012 31(5):453-57.10.1097/PGP.0b013e318246977d22833086 [Google Scholar] [CrossRef] [PubMed]
[10]. Levine PH, Mittal K, Rhabdoid epithelioid leiomyosarcoma of the uterine corpus: A case report and literature reviewInt J Surg Pathol [Internet] 2002 10(3):231-36.10.1177/10668969020100031412232582 [Google Scholar] [CrossRef] [PubMed]
[11]. Togami S, Kawamura T, Fukuda M, Yanazume S, Kamio M, Kobayashi H, Clinical management of uterine cervical mullerian adenosarcoma: A clinicopathological study of six cases and review of the literatureTaiwanese J Obstet Gynecol 2018 57(4):479-82.10.1016/j.tjog.2018.04.03230122564 [Google Scholar] [CrossRef] [PubMed]