Shoulder pain leading to dysfunction is a significant health issue in younger as well as older population. In terms of most common areas of musculoskeletal pain, shoulder pain is next to pain in the low back and knee [1]. Subacromial impingement syndrome (SAIS) is a common disorder of shoulder, accounting for 44-65% of all complaints of shoulder pain during a pain clinic visit [2,3]. SAIS encompasses a spectrum of subacromial space pathologies ranging from tendinopathy to rotator cuff tears. The main consequences of SAIS are functional loss and disability [4]. Its challenging to find exact aetiology for early diagnosis and adequate pain relief along with functional restoration of shoulder movements. To exactly locate the underlying cause, numerous diagnostic clinical tests are available, but Imaging is required for non-responders to conservative modalities. Various modalities used for evaluation of shoulder pathologies are; Radiographs, Magnetic Resonance Imaging (MRI), MR Arthrogram and diagnostic ultrasound.
MRI is “the gold standard” imaging and crucial in guiding specific treatment modality. However, recently use of ultrasound has evolved as a promising tool for diagnosing extra-articular soft-tissue shoulder pathology. There are notable advantages of using ultrasound over MRI in diagnosis of subacromial pathologies like portability, easy availability, low cost and to plan an intervention. Ultrasonography (USG) is the modality which shall be used in both diagnostic and therapeutic purposes for management of subacromial shoulder pathologies [5].
Thus, the present study was conducted to estimate the spectrum of subacromial shoulder pain disorders in terms of frequency dictated by US- diagnosed findings. To use ultrasound as a diagnostic modality for evaluation of shoulder impingement and to determine the frequency of the specific US-diagnosed shoulder disorders in patients with subacromial shoulder pain referred from orthopaedics Outpatient Department (OPD). Additionally, we investigated which tendons (rotator cuff and longhead of the biceps) were affected, and type of ultrasound findings in individual tendons.
Materials and Methods
This was a retrospective observational study conducted on data of patients that visited the study institute from October 2018 to November 2019 at SHKM, GMC Nalhar, Mewat, Haryana. Total of 160 patients’ data with complaints of shoulder pain were screened. Out of these, 98 patients were clinically and radiologically diagnosed to have subacromial shoulder pain, were included in the present study.
Inclusion criteria
Age between 18 and 70 years.
Shoulder pain upon abduction with painful arc.
Symptoms lasting no longer than three months.
No previous history of shoulder surgery.
Exclusion criteria
History of fracture or dislocation of shoulder.
Gleno-humeral joint disease.
History of fractures of the proximal humerus or acromion, dislocation and/or surgery of the affected shoulder.
Shoulder complaints caused by suspected referred complaints or extrinsic cause.
Data Collection
Total of 98 patients record were assessed for demographic variables like age, gender along with affected shoulder. Relevant data of clinical and radiological examination and ultrasound based diagnosis were analysed.
Clinical and Imaging Algorithm
For suspected subacromial pathology following algorithm is followed and recorded at the institution. So, the case specific findings were observed from such records for the study purpose.
Step 1: Specific Clinical Test
Neer test and Hawkins kennedy test for sub acromial pain.
Jobe test and External rotation lag sign for the supraspinatus tendon pathology.
Gerber lift-off test and belly press test for subscapularis tendon pathology.
Hornblower’s Sign for infraspinatus and teres minor tendons.
Speed test and Yergusons test for biceps pathology .
Step 2: Diagnostic Ultrasound
Ultrasound examination of shoulder was done for supporting our clinical judgment. Findings of diagnostic ultrasound, and treatment plan were analysed.
Scanning Technique
Typically, a linear high frequency probe of Micromax Sonosite inc, USA portable ultrasound machine was used based on basic principles of musculoskeletal ultrasound that is examining each structure in two planes and maintaining perpendicularity to tendon fibers. Standardised US diagnostic criteria for pathology were used [6]. The long head of the biceps tendon (LHBT), rotator cuff, SASD bursa, deltoid muscle and Acromioclavicular (AC) joint were sequentially evaluated in every case.
Statistical Analysis
Descriptive statistics was performed through frequency and percentages using MS-Excel software.
Results
Out of 98 patients 57% were male. Majority of patients (61%) were in age group 31-50 years and US was performed in right shoulder in 67% of cases [Table/Fig-1].
Distribution of age, sex and shoulder dominance of shoulder Impingement syndrome (n=98).
| Variables | Frequency of shoulder impingement syndrome (%) |
|---|
| Age (Years) |
| 18-30 | 16 (16%) |
| 31-50 | 60 (61%) |
| 51-70 | 22 (23%) |
| Gender |
| Male | 56 (57%) |
| Female | 42 (43%) |
| Shoulder involvement |
| Right | 64 (67%) |
| Left | 34 (33%) |
Frequency of Ultrasound based Disorders
Most common ultrasound findings in subacromial shoulder pain patients were subacromial bursopathy 46 (46.93%) followed by Rotator cuff pathology including tear 38 (38.77%), mixed pathology 9 (9.18%) and AC joint pathology 5 (5.10%). Isolated biceps pathology was not seen in our study rather biceps pathology along with other tendon and joint involvement was observed. Among 46 patients with findings of subacromial bursopathy 26 (56.52%) patients had bursal effusion and 20 (43.47%) patients had findings of bursal thickening. Rotator cuff involvement was observed in 20 patients (43.47%) presenting with findings suggestive of bursopathy [Table/Fig-2]. As shown in [Table/Fig-3], Rotator cuff pathology was observed in 38 (38.77%) of patients with subacromial pain. Spectrum of findings among this category includes Tendinopathy including calcific (31%) and Partial thickness tear (PTT 31%) followed by Full thickness tear (FTT 28%) and intrasubstance tear (10%).
Subacromial bursopathy with or without RC tear.
| Pathology | Subacromial bursopathy only n (%) | Bursopathy with rotator cuff involvement n (%) |
|---|
| Number of patients | 26 (56%) | 20 (44%) |
Distribution of various types of anatomical involvement among shoulder impingement syndrome patients (N=98).
| Type of anatomical involvement | Frequency | Total |
|---|
| Subacromial bursopathy |
| Bursal effusion | 26 | 46 |
| Bursal thickening | 20 |
| Rotator cuff pathology |
| Tendinopathy Including calcific tendinopathy | 12 | 38 |
| FTT | 11 |
| PTT | 12 |
| Intrasubstance | 3 |
| Supraspinatus tendon pathology |
| Tendinopathy Including calcific tendinopathy | 12 | 36 |
| FTT | 12 |
| PTT | 9 |
| Intrasubstance | 3 |
| AC joint pathology |
| Effusion | 3 | 5 |
| Arthritis | 2 |
| Mixed pathology |
| Bursal effusion and FTT of supraspinatus and infraspinatus and GH joint effusion | 4 | 9 |
| Bursal effusion With FTT and bicipital effusion | 4 |
| FTT Supraspinatus with AC joint cyst | 1 |
PTT: Partial thickness tear; FTT: Full thickness tear; AC: Acromioclavicular; GH: Glenohumeral
Supraspinatus muscle was involved in 36, (94%) of cases in RC pathology and 2 (6%) of patients subscapularis tear was observed. Out of 98 patients only 5 (5%) patients had been diagnosed with AC joint pathology. Three patients had effusion while two patients had arthritis. Isolated biceps pathology was not seen in any patient in our study. Patients with more than one finding in ultrasound were categorised as mixed pathology group and were divided into three subgroups. Four (4%) patients with effusion had bicipital effusion and Similar percentage of patients had Glenohumeral (GH) joint effusion. One patient had AC joint cyst and later these cases were confirmed with MRI for further management.
Discussion
Mobility of shoulder comes at the cost of stability. The stability and concurrent multidirectional mobility of shoulder joint is dependent on various structures. Rotator cuff is one of the main structures essential for dynamic and static stability as well as mobility of the joint. Although rotator cuff tears are common cause of shoulder pain and disability but other subacromial structures may generate pain and treatment depends upon type of underlying pathology so clinical judgment alone is not sufficientenough to initiate interventional treatment. The ability of ultrasonogram to determine type of subacromial pathology is really helpful to go ahead with treatment. The present study is based on clinical and diagnostic ultrasound evaluation of 98 shoulder pain patients due to subacromial pathology. Patients were treated for shoulder impingement syndrome according to the pathology established by diagnostic ultrasound and followed in OPD. Treatment part was not included in this study.
In the present study all patients ranging from 18 to 70 years were included, with maximum patients in age group 31-50 years of age (61%). In study of Danielle A et al., found that peak age of shoulder pain and impingement was 45-64 years and subacromial impingement was most frequent diagnosis in this age group [7]. Shrestha M and Alam A, studied 50 patients of rotator cuff tear and found mean age was 41.6 years (range 15-80) [8]. Maximum patients were between 41-50 years (24%). Results of the present study are according to literature, there was increase incidence of shoulder impingement syndrome during late middle age and advance age. In the present study male and female were 56 (57%) and 42 (43%) as shown in [Table/Fig-1]. Milgrom C et al., found no statistically significant difference in the incidence of impingement findings between male and female gender [9]. In existing literature there are equivocal incidence of shoulder impingement syndrome in males and females.
There are numerous special tests that have been developed for ruling in or ruling out subacromial impingement. Authors have used specific clinical test for specific underlying pathology. Michener LA et al., examined the reliability and diagnostic accuracy of five such tests: Hawkins-Kennedy, Neer, painful arc, empty can, and external rotation resistance [10]. These tests have been found to have fair to substantial strength of interrater reliability.
Ultrasound Criteria
Ultrasonography and Magnetic Resonance Imaging (MRI) are both widely used investigations for Subacromial Impignment syndrome. Ultrasonography has several advantages over MRI scans as they tend to be more accessible, cheaper, and provide a dynamic assessment of the shoulder, but is highly operator dependent [11]. In the present study we have used ultrasound as a diagnostic modality to support our clinical findings. By using following ultrasound criteria patients were categorised into different groups and subgroups [12].
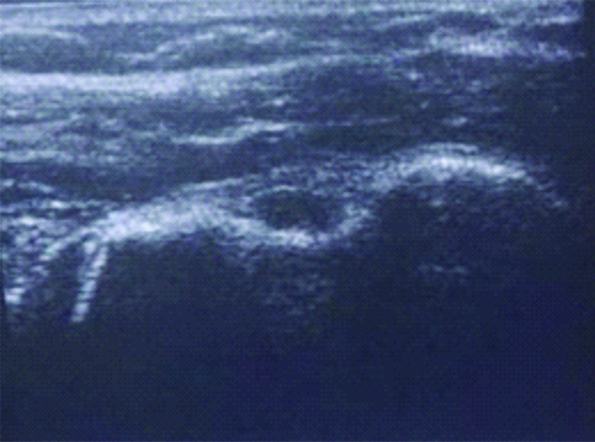
Subacromial bursopathy: A pathologic subacromial-subdeltoid bursa appears thickened (>2 mm), hypoechoic, and may be associated with hyperemia termed as subacromial bursopathy. Further categorised as bursal effusion as shown in and Bursal thickening [Table/Fig-4].
Subacromial subdeltoid Bursal effusion seen as hypoechoic collection below deltoid.
Rotator cuff pathology
Tendon calcification: Hyperechoic with or without an acoustic shadow (depending on the amount of calcification) within the rotator cuff.
Tendinopathy: Thick swollen tendon with hypoechoic. Partial interruption may occur inside the tendon. Irregularity of fibrillar pattern, fragmentation.
Tear:
Partial thickness tear: Hypoechoic zone or focus within the rotator cuff. Focal cuff thinning on the articular or deltoid located side.
Intramural tear: Hypoechoic zone or focus within the rotator cuff.
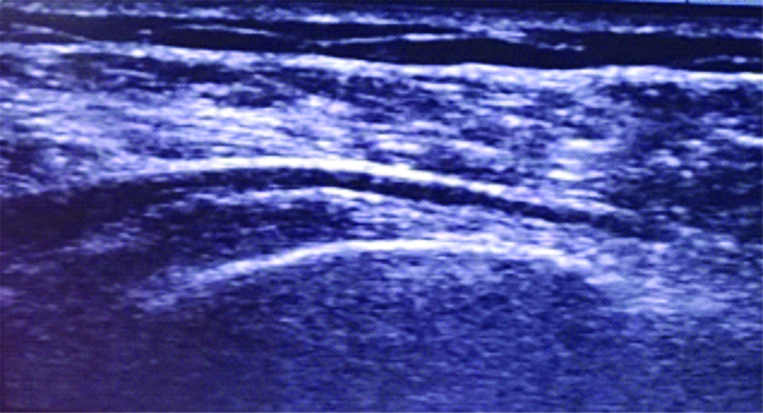
Full thickness tear: Tear extending from bursal to articular side [Table/Fig-5,6].
Long axis view of supraspinatus tendon with full thickness tear.
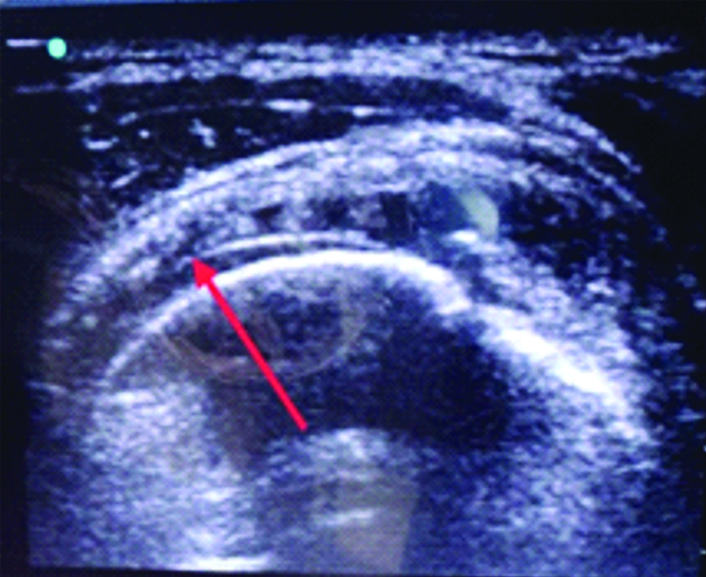
Short axis view of supraspinatus tendon showing cortical irregularity in full thickness tear
AC joint pathology:
Joint space narrowing: Narrowing of the space of the two articular forming bones.
Osteophytes: A bony prominence seen at joint line.
Effusion: Extension of the joint capsule filled with anechoic fluid.
Long head of biceps:
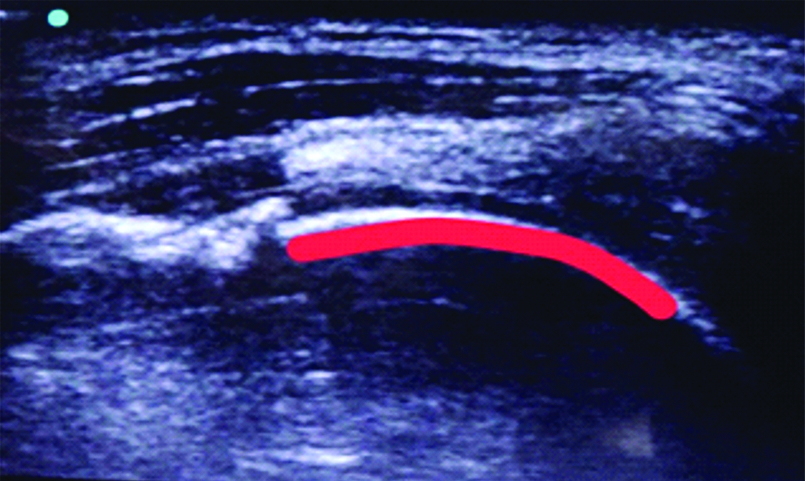
Tendon sheath effusion: Extension of the joint capsule filled with anechoic [Table/Fig-7].
Biceps tendon sheath effusion in a patient with full thickness Rotator cuff tear.
Subluxation: Visualisation of a subluxated long biceps tendon.
Sub Acromial Impigenment and Structures Involved
A) Subacromial bursopathy: In the present study, among subacromial bursopathy based upon ultrasound criteria bursal effusion (56%) was most common finding followed by bursal thickening (44%) and Ultrasound really helped in targeted injections in such findings in the present study.
The study on 104 patients by Kvalvaag E et al., with subacromial impingement pain found 65 patients (56.4%) with subacromial bursal inflammation [13]. According to this study bursitis is a common cause (46%) of shoulder impingement syndrome.
B) Rotator cuff pathology: Ultrasound based disorders of Rotator cuff causing impingement ranges from Tendinopathy including calcific tendinopathy and partial and full thickness rotator cuff tears. In present study among rotator cuff pathology, out of 38 patients only two patients had subscapularis tear and rest of patients had supraspinatus pathology. Supraspinatus tendon evaluation was done to reveal the underlying pathology.
C) Supraspinatus tendon pathology: In this study Authors have found 12 (32%) patients had supraspinatus involvement. Spectrum of findings among this category includes Tendinopathy including calcific (31%) and PTT (31%) followed by FTT (28%) and intrasubstance tear (10%). Freygant M et al., analysed 137 shoulder MRI, examinations rotator cuff and confirmed by this study, injury was diagnosed in 106 (82%) patients, including 100 (94%) patients with isolated supraspinatus tendon injury or together with the remaining rotator cuff muscles, which is concordant with literature data indicating that supraspinatus muscle tendon is damaged in 95% of rotator cuff pathologies [14]. This study shows partial supraspinatus tendon tear in 86 (81%) subjects with diagnosed rotator cuff pathology, while complete tear was diagnosed in 11 (10%) patients. The same applies to infraspinatus muscle tendon (where partial tear occurred in 34 patients, while three patients suffered complete tear) and subscapularis muscle tendon (where 40 patients were diagnosed with partial tear and only one with complete tear). Out of total 38 patients, 2 (3%) patients with subscapularis involvement. Codman EA et al., reported 3.5% isolated injury of subscapularis and 8% of rotator cuff injuries had tears of the subscapularis tendon [15].
D) AC joint pathology: Out of 98 patients only 5 (5.10%) patients had been diagnosed with AC joint pathology. Three patients had effusion while two patients had arthritis [Table/Fig-3]. In literature study done on diagnostic ultrasound reports of 240 patients of shoulder pain, incidence of AC joint pathology was found to be 0.4% [16]. Incidence of AC joint pathology increases with increasing population of elderly people so there are variation in incidence of AC joint pathology in different population coharts [17].
E) Bicep tendon pathology: In this study isolated biceps pathology was not seen in any patient rather in 4 (4%) patients out of 98 mixed pathology was observed and confirmed with MRI for further management. These patients were found to have biceps effusion along with FTT of supraspinatus and subscapularis and bursal effusion. Literature suggest 5%-35% cases of shoulder impingement have bicep tendinitis features [18]. High range value can be explained by literature data which suggest bicep tendon rarely involves, who do not involved in sports like throwing/swimming, and bicep tendon commonly involve in sports person. In this study data results have been obtained from general population of shoulder impingement syndrome not from population of athletes. In another study of Patton WC et al., found 5% patients of shoulder pain and impingement had Biceps tendinitis [19].
F) Mixed pathology and SAIS: In literature, Authors could not find detailed frequency of factor combinations in multifactorial origin of shoulder impingement syndrome. Literature suggest origin of shoulder impingement remains multifactorial. Freygant M et al., analysed 137 shoulder MRI [14], 37 (27.01%) patients of shoulder impingement syndrome were diagnosed of infraspinatus involvement. Among 37, 34 patients with partial thickness tear and three patients with full thickness tear of infraspinatus muscle tendon. In the present study 4 (8%) shoulder pain patients out of 98, had findings of infraspinatus and GH joint effusion in older age group.
Limitation(s)
There are some limitations in this study. This study was conducted in one medical center only. In future related studies, shoulder pain patients from multicenters will be recruited as well. In India, patients with shoulder pain can visit any department freely. These patients may not have the opportunity to receive ultrasound imaging evaluation first. Another limitation of this study is use of ultrasound based diagnosis in tailoring treatment has not been documented and lack of confirmation of ultrasound based findings with MRI which is gold standard imaging modality.
Conclusion(s)
Present study shows that subacromial shoulder pain patients can be categorised into different groups and subgroups based upon diagnostic ultrasound findings. Ultrasound is really helpful in understanding the underlying pathology and initiating treatment. Future research should be done based on cost effectiveness of ultrasonogrpahy as primary imaging modality in subacromial shoulder pain patients. In addition to static study dynamic evaluation of shoulder pain patients will help to understand disease better. Moreover, with increased use of diagnostic ultrasound as outpatient diagnostic modality, number of MRIs needed can be minimised thus reducing the health care cost which in turn helps in preventing treatment delay.