A Rare Case of Cervical Fibroid in a Young Woman Managed by Uterus Conserving Surgery
Chandana Galidevara1, Dhivya Rajarajan2
1 Associate Professor, Department of Obstetrics and Gynecology, Sri Venkateswara Medical College Hospital and Research Institute, Puducherry, India.
2 Senior Resident, Department of Obstetrics and Gynecology, Sri Venkateswara Medical College Hospital and Research Institute, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dhivya Rajarajan, 57, Om Sakthi Nagar, 2nd Street, Kondur Post, Chavadi, Cuddalore-607006, Tamil Nadu, India.
E-mail: crdhivya2109@gmail.com
Cervical fibroid is a surgical challenge to the gynaecologist, more so when an attempt to conserve the uterus is made in young patients who want to preserve their fertility. The presenting complaint in cervical fibroids are mainly pressure symptoms due to compression on surrounding structures in the pelvis, which is an indication for surgical management. The mainstay of treatment in older patients who have completed family has been hysterectomy. Here authors report a case of 29-year-old young multiparous women, who underwent caesarean section in her second pregnancy because of cervical fibroid diagnosed antenatally elsewhere, presented to us postnatally with pain and pressure symptoms with abdominal distension due to that central cervical fibroid for 7 months in the postnatal period. She was managed by uterus conserving surgery with the involvement of a multi-disciplinary team.
Leiomyoma, Myomectomy, Pressure symptoms
Case Report
A 29-year-old multiparous women with previous Caesarean section presented postnatally with complaint of abdominal distension, dull aching lower abdominal pain and frequent micturition for seven months. She was diagnosed with a large cervical fibroid incidentally during her antenatal ultrasound in second trimester. Patient was asymptomatic during her antenatal period and delivered a 2.5 kg baby by caesarean section in view of cervical fibroid. There was no previous history of fibroid in pre-pregnancy period. She did not have nausea, vomiting, abnormal bleeding, decreased appetite and weight loss. Nobody in her family had fibroids.
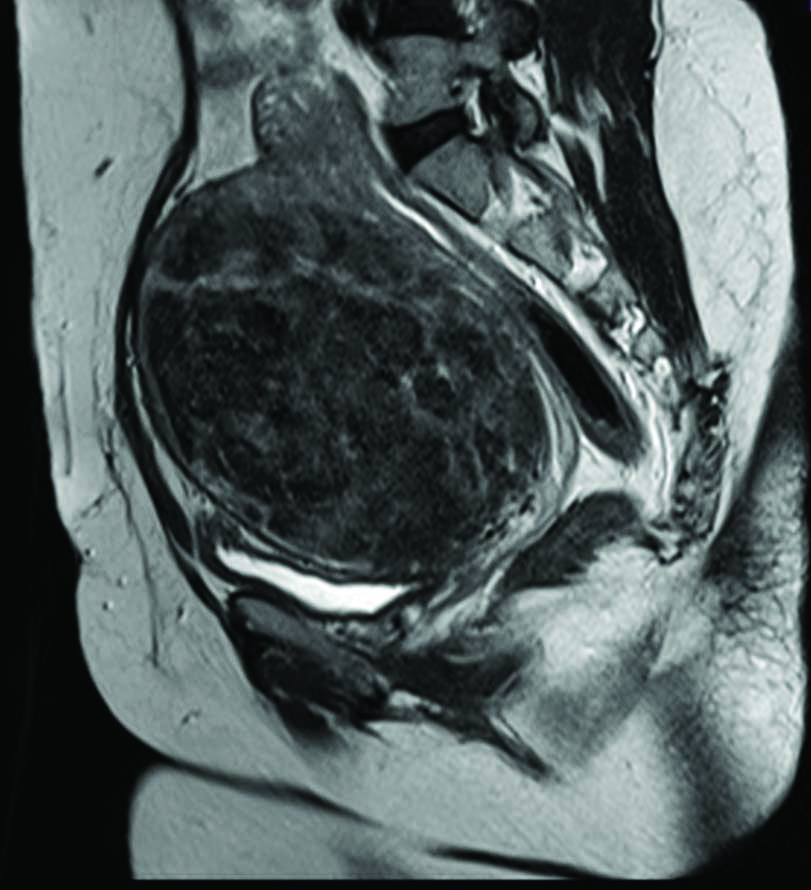
On abdominal examination, a pfannenstiel scar was noted and an 18 weeks irregularly enlarged, firm mass occupying hypogastrium and both iliac regions was palpable. The lower border of the mass was not palpable with restricted side to side mobility. Bimanual examination showed the cervix was drawn up, thinned out and effaced. The mass could be felt through all fornices giving rise to the clinical diagnosis of cervical leiomyoma. Rectal examination revealed a firm bulge through the anterior rectal wall. The above findings were confirmed by Magnetic Resonance Imaging (MRI) Pelvis [Table/Fig-1]. Intravenous pyelogram was done to study the course of ureter, which showed a pelvic mass compressing on the bladder with bilateral grade I hydro-ureteronephrosis and ureters displaced laterally with obstruction at the pelvic brim. Patient was not anaemic and all baseline investigations were within normal limits.
MRI pelvis revealing the sagittal section of the cervical fibroid.
A multidisciplinary team approach involving obstetrician, urologist, radiologist and anesthetist was planned. The decision for surgery was taken in view of pressure effects. Uterus conserving surgery or myomectomy was planned in view of the patient’s age with additional consent for hysterectomy in case of life threatening haemorrhage.
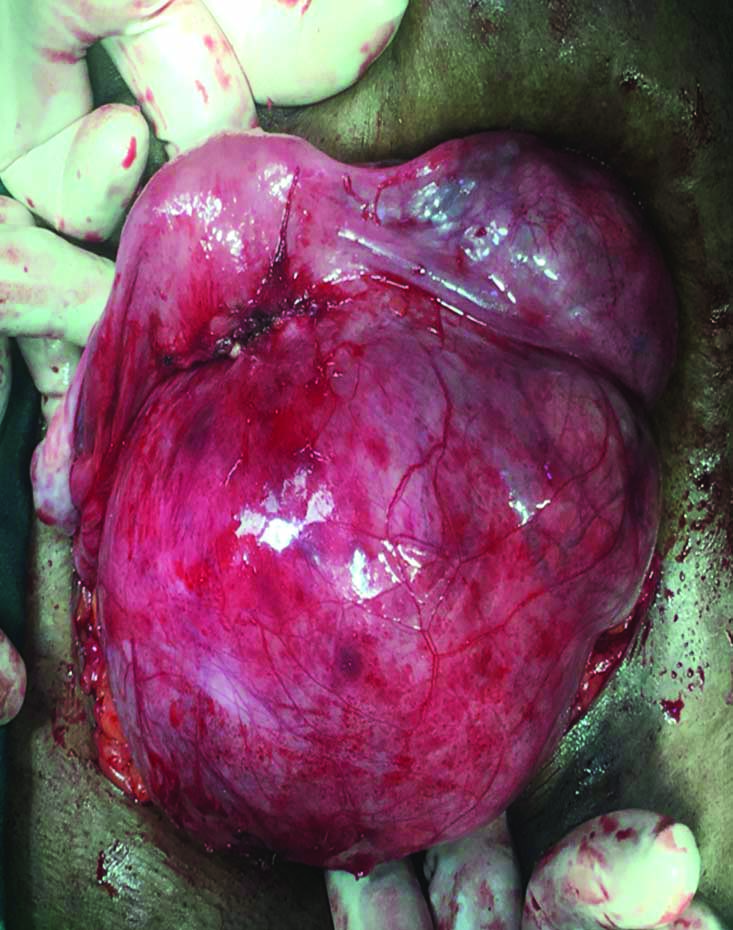
Intraoperatively, an anterior cervical fibroid of size 18×16 cm was noted, with the uterus perched on top and pushed superiorly and posteriorly giving a characteristic appearance of lantern on the dome of St. Paul’s cathedral [Table/Fig-2]. The cervical fibroid was extending into the broad ligament on either side. Bilateral ovaries and tubes were normal. Bladder along with the uterovesical fold was stretched and pulled over the fibroid. The stretched uterovesical fold was dissected and the bladder was pushed down. Vasopressin was injected (100 mL of 1: 20 dilution) all around the mass and the fibroid was enucleated by a longitudinal incision at the most prominent part. The endometrial cavity was accidentally breached while enucleating the upper part of the fibroid. The cavity was reconstructed with 2-0 vicryl. The fleshy, vascular pedicles at the base were ligated and haemostasis was secured meticulously. The uterine defect was repaired in two layers with 1-0 vicryl and the uterus was conserved. Posterior part of the uterus was examined and found to be intact. Bladder integrity was checked with methylene blue dye instillation. The fibroid specimen weighed 1020 g. Histopathology of the specimen confirmed benign leiomyoma.
Intraoperative finding of cervical fibroid with the uterus perched on top with a characteristic appearance of Lantern on St.Paul’s cathedral on the left.
Postoperatively, the patient recovered without any complications. On second postoperative day foley’s catheter was removed. A course of injectable depot medroxyprogesterone acetate 150 mg deep intramuscularly was given for contraception as patient did not consent for sterilisation. She was adequately counselled regarding complications in subsequent pregnancy and advised to avoid pregnancy atleast for two years and motivated for permanent sterilisation in the future. Till then, she was advised to follow temporary contraception. She was sensitised regarding the recurrence of fibroid too. Patient was discharged on seventh postoperative day. She was asked to come for review six weeks later. Patient came for follow-up as per advice. She was comfortable with no complaints. Abdominal wound healed well and physical examination was normal. She accepted for tubal sterilisation, but after six months due to social reasons. Till then, she wanted to continue with injectable contraception which she is presently using.
Discussion
Leiomyoma is a common benign solid tumour of uterus. But its occurrence in cervix is rare [1]. Uterine fibroids are a major cause of morbidity in women of a reproductive age (and sometimes even after menopause). There are several factors that are attributed to underlie the development and incidence of these common tumours. The most likely presentation of fibroids is by their effect on the woman’s menstrual cycle or pelvic pressure symptoms [2]. Cervical fibroids can have damaging consequences due to insidious pressure effects mainly affecting the urinary tract. The index patient presented with anterior pressure symptoms and grade I hydro-ureteronephrosis which was progressive in nature. The characteristic hallmark of cervical fibroid on vaginal examination is a ballooned out, effaced cervix. Imaging with ultrasound and MRI helps in clinching the diagnosis. As the ureteric course is distorted by a large pelvic mass, it is advisable to perform an intravenous pyelogram to detect any deviation of the course of ureter and consider pre-operative stenting of ureters if difficulty is anticipated. Enucleation of the cervical fibroid is preferred before performing hysterectomy as this technique prevents injury to the adjacent vital anatomical structures [3]. In a case study by Mendiratta S et al., a 38-year-old female patient was managed by myomectomy in piece meal followed by hysterectomy [4]. A single dose Gonadotropin-Releasing Hormone (GnRH) agonist was given prior to myomectomy to reduce blood loss. Another case report, a 10 kg cervical fibroid was enucleated followed by hysterectomy. The patient had iatrogenic ureteric injury which was repaired intraoperatively [3].
In our patient myomectomy was planned in view of her age, as it also helps in preserving future fertility and preventing premature menopause. A thorough counseling of risks and benefits of the procedure was undertaken and additional consent for hysterectomy was sought in case of life threatening haemorrhage or difficulty in removal of the fibroid. Additional consent for repair of ureter or ureteric reimplantation was also taken. In selected cases, pre-operative administration of GnRH analogues for three months reduced the fibroid size and minimised the intraoperative blood loss [5]. In our patient GnRH administration was contraindicated as she was lactating. However, steps to prevent blood loss were taken by using hypotensive anesthesia and injecting vasopressin prior to myomectomy. Also, an adequate back up of blood products was ensured. Surgery in case of cervical fibroid is complicated due to distorted pelvic anatomy, disruption of course of ureter thereby increasing the chance of injury to the bladder, ureters and uterine arteries [1]. Multidisciplinary team approach is the need of the hour when managing such cases. A meticulous closure of the defect in the myometrium after enucleation and good haemostasis should be ensured for achieving optimal repair. Since there is insufficient literature on the pregnancy outcome after cervical fibroid myomectomy, appropriate follow-up of such cases cannot be over emphasised.
In a case report by Keriakos R and Meher M, they reported 29-year-old nulligravida diagnosed with sessile cervical fibroid in the vaginal portion of the posterior lip of cervix, managed by vaginal myomectomy in the postnatal period after her first delivery which was by caesarean section due to fibroid [6]. They managed with conservative surgical treatment, which was similar to present case.
The incidence of cervical fibroid is around 0.5-2% [7]. Bhandiwad A et al., reported a similar central cervical fibroid in a perimenopausal lady with pressure symptoms and mass per abdomen [7]. She underwent total abdominal hysterectomy with bilateral salphingo oophorectomy. Since the patient’s presentation was similar to the above case report with the exception that the patient was a young postnatal mother, in whom uterus conservation is our priority.
Shah M and Laddad M, in their article reported three unusual cases of fibroid presentations [8]. Their three cases were perimenopausal ladies who underwent abdominal hysterectomy. Even then, they quoted that fibroids in relatively unusual locations such as within the cervix will be treated either by myomectomy or hysterectomy. They give rise to greater surgical difficulty due to their complex anatomy. Since our patient was a young mother, we proceeded with myomectomy in spite of greater surgical challenge. Prompt case selection and meticulous surgery with multi-disciplinary team approach was the strength of our case.
Conclusion(s)
Cervical fibroid must be treated meticulously with regard to the age of the patient, parity and symptoms. Our main aim was to conserve the uterus by myomectomy, since the patient was young and we could succeed in it. The only disadvantage being its possibility of recurrence.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 13, 2020
Manual Googling: Dec 22, 2020
iThenticate Software: Jan 15, 2021 (5%)
[1]. Jayashree V, Mahjabeen B, Thariq IA, A case of huge cervical fibroid with characteristic “Lantern on StPaul’s Cathedral” appearance. Indian Journal of Basic and Applied Medical Research 2015 4(3):455-58. [Google Scholar]
[2]. Khan AT, Shehmar M, Gupta JK, Uterine fibroids: current perspectivesInt J Womens Health 2014 6:95-114.10.2147/IJWH.S5108324511243 [Google Scholar] [CrossRef] [PubMed]
[3]. El-Agwany AS, Swelam MS, Unusual giant central cervical leiomyoma: A description of two casesArchives of Perinatal Medicine 2014 20(2):113-15. [Google Scholar]
[4]. Mendiratta S, Dash S, Mittal R, Dath S, Sharma M, Sahai RN, Cervical fibroid: An uncommon presentationInt J Reprod Contracept Obstet Gynaecol 2017 6:4161-63.10.18203/2320-1770.ijrcog20174084 [Google Scholar] [CrossRef]
[5]. Lethaby A, Vollenhoven B, Sowter M, Efficacy of pre-operative gonadotrophin hormone releasing analogue for women with uterine fibroids undergoing hysterectomy or myomectomy: A systematic reviewBJOG 2002 109:1097-108.10.1111/j.1471-0528.2002.01225.x12387461 [Google Scholar] [CrossRef] [PubMed]
[6]. Keriakos R, Meher M, Management of cervical fibroid during the reproductive periodCase Reports in Obstetrics and Gynaecology 2013 2013:9840303 pages, 2013. http://doi.org/10.1155/2013/98403010.1155/2013/98403024109537 [Google Scholar] [CrossRef] [PubMed]
[7]. Bhandiwad A, Gowda SL, Anupama NK, Central cervical fibroid with a typical Lntern on top of St.Pal’s cathedral appearanceInt J Reprod Contracept Obstet Gynaecol 2016 5:924-26.10.18203/2320-1770.ijrcog20160615 [Google Scholar] [CrossRef]
[8]. Shah M, Laddad M, Three cases of unusual presentation of fibroidJ Evolution Med Dent Sci 2018 7(35):3926-28.10.14260/jemds/2018/878 [Google Scholar] [CrossRef]