Morphologic and Morphometric Study of Human Acetabulum and its Clinical Significance
KR Arunkumar1, U Delhiraj2, S Satish Kumar3
1 Associate Professor, Department of Anatomy, Dhanalakshmi Srinivasan Medical College and Hospital, Perambalur, Tamil Nadu, India.
2 Assistant Professor, Department of Anatomy, Dhanalakshmi Srinivasan Medical College and Hospital, Perambalur, Tamil Nadu, India.
3 Associate Professor, Department of Anatomy, Government Dharmapuri Medical College, Dharmapuri, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. KR Arunkumar, Associate Professor, Department of Anatomy, Dhanalakshmi Srinivasan Medical College and Hospital, Perambalur-621212, Tamil Nadu, India.
E-mail: drarunb4u@gmail.com
Introduction
The acetabulum is a cup shaped hemispherical depression which is present on the hip bone, contributed by ilium, ischium and pubis. It has a central depressed non-articular part called acetabular fossa, surrounded by a curved lunate articular surface which articulates with the head of femur to form hip joint. The knowledge of acetabular dimensions assists the radiologists in diagnosing acetabular dysplasia and aids the surgeon to determine the correct size of the acetabular cup during total hip arthroplasty and to realign the acetabulum back to normal position.
Aim
To measure and analyse the relationship between the depth and diameter of acetabulum and also to study the variations in the morphology of anterior acetabular ridge.
Materials and Methods
A cross-sectional study was done on 104 unpaired dry human adult hip bones from February 2017 to September 2019 after obtaining ethical clearance. The diameter and depth of acetabulum was measured using vernier calliper and a metallic strip and correlation between them were analysed using Pearson’s test. Student’s t-test was used to test the significance between the variables. The p-value <0.05 were considered as statistically significant. The different shapes of anterior acetabular ridge were noted. All the recorded data were analysed using Statistical Package for the Social Sciences (SPSS version 16.0).
Results
The average measurements of acetabular diameter and depth were 48.98±2.91 mm and 24.12±2.54 mm, respectively. A positive and a significant correlation was found between diameter and depth of the acetabulum (r=0.388, p<0.001). The mean values of diameter and depth of acetabulum in right side were 48.76±2.94 mm and 23.6±2.48 mm, respectively. The average values of diameter and depth in left side were 49.2±2.92 mm and 24.6±2.59 mm, respectively. Though the measurements of acetabular dimensions on left side were slightly greater than right side, they were not statistically significant (p>0.05). Four different shapes of anterior acetabular ridges were noted: angular (23.08%), curved (63.46%), straight (2.88%) and irregular (10.58%).
Conclusion
The present study showed weakly positive correlation between diameter and depth of the acetabulum and morphological variations in the shape of anterior acetabular ridge.
Femoracetabular impingement, Hip arthroplasty, Hip bones, Hip dysplasia, Prosthesis
Introduction
The hip bone, a component of pelvic girdle, is a large, irregular bone, constricted centrally and expanded above and below. The lateral surface of hip bone presents a deep, cup-shaped depression named acetabulum, which articulates with the femoral head forming hip joint [1]. The acetabulum is formed by the contributions of all the three components of hip bone: ilium, ischium and pubis [2]. The hip joint is formed by the articulation of acetabulum with head of femur. It was previously referred as multiaxial spheroidal type of ball and socket synovial joint but now it is described as rotational conchoids [3]. The articular surfaces of the head of femur and the acetabulum are reciprocally curved but neither co-extensive nor completely congruent [1]. The articular surface does not occupy the entire acetabular socket but is a C-shaped concavity called as lunate surface, which is broadest above where the body weight is transmitted in the erect posture [2]. The lunate surface is covered by a thick articular cartilage. The central non-articular area in the floor of the acetabulum known as acetabular fossa is devoid of cartilage and occupied by a pad of fat [2]. The acetabulum is deepened by a fibrocartilaginous rim, acetabular labrum which is attached to the peripheral margin of acetabulum [1].
Abnormalities in the acetabulum such as acetabular size, width, depth, orientation and the coverage of femoral head results in abnormal mechanical behaviour of hip joint which results in hip dysplasia [4]. This hip dysplasia produces instability of hip joint causing the rapid degeneration of articular cartilage which ultimately ends in osteoarthritis [4]. About 25.5% of osteoarthritis of hip joint is caused by acetabular dysplasia [5]. The shape of the acetabulum can be modified in the prenatal period due to disturbances in its development or in the postnatal period due to diseases damaging the cartilage of lunar articular surface of the acetabulum [6]. The normal depth of the acetabulum is 9 mm and less than that is considered as dysplasia [5]. In acetabular dysplasia, roof of the acetabulum is underdeveloped and remains vertically oriented and shallowed which results in the decreased surface area for weight bearing. This reduced weight bearing area receives a much larger force per unit area during walking and may result in early degenerative changes [7].
The key for diagnosing acetabular dysplasia is the accurate evaluation of quantitative parameters of the acetabulum. Hence, the knowledge of morphometric parameters of the acetabulum is essential for the radiologists in diagnosing congenital dysplasia of hip and for surgeons to identify the correct size of the acetabular prosthesis during hip arthroplasty to prevent the complications like prosthetic loosening or dislocation [8].
The details about the morphology of anterior acetabular ridge are of significance during total hip arthroplasty. Posterior acetabular ridge almost always remains similar at most times by forming a simple semicircle. But the morphology of anterior acetabular ridge varies, and these variations affect the amount of anteversion and may end in iliopsoas impingement after arthroplasty, as the prosthesis overlaps at the anterior acetabular ridge [9]. The iliopsoas impingement syndrome can occur with all implants, but it is reported more often in cases where the implant is oversized [10].
Many authors have studied the acetabular dimensions in India and worldwide [11-14]. Based on the available literature, there is no documented study on the variations in acetabulum conducted in the region of Tamil Nadu, India.
Hence, this study was undertaken with the aim of determining the diameter and depth of the acetabulum, identifying the relationship between diameter and depth of acetabulum and detecting the variations in the shape of anterior acetabular ridge.
Materials and Methods
This cross-sectional study was conducted on 104 dry human adult hip bones of unknown sex belonging to both sides (54 right and 50 left) in the Department of Anatomy of Dhanalakshmi Srinivasan Medical College and Hospital, Perambalur, Tamil Nadu and Government Dharmapuri Medical College, Dharmapuri, Tamil Nadu, India from February 2017 to September 2019 after obtaining ethical clearance from Institutional Ethics Committee of human studies (Project no. IECHS/DSMCH/026). Bones with evidence of wear and tear, congenital defects and fracture were excluded from the study.
Morphometric Parameters
The morphometric parameters taken in the present study were depth and diameter of the acetabulum. The procedures for measuring the depth and diameter were taken from previous studies [11,12]. The parameters were measured as follows:
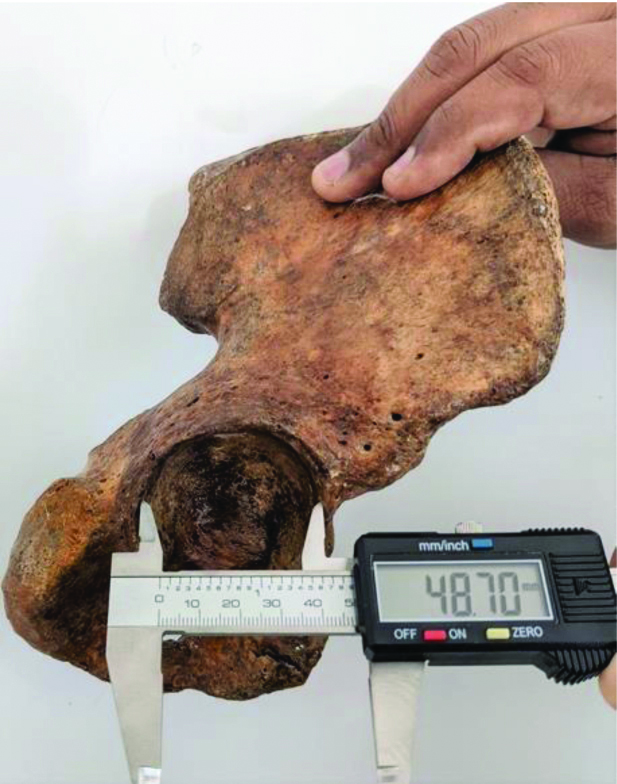
Diameter of the acetabulum- The distance between the acetabular ridge nearest to the body of ischium and anterior iliac margin intersecting the acetabular ridge was measured as acetabular diameter using digital vernier caliper [Table/Fig-1].
Measurement of diameter of acetabulum.
Depth of the acetabulum- Maximum vertical distance from the deepest point in the acetabular cavity to the brim of the acetabulum was taken as depth. A metallic strip was placed across the acetabular margin and depth of the acetabulum was measured in millimeters using digital vernier caliper from the deepest point in the acetabulum to metallic scale [Table/Fig-2].
Measurement of depth of acetabulum.

Morphologic Parameter
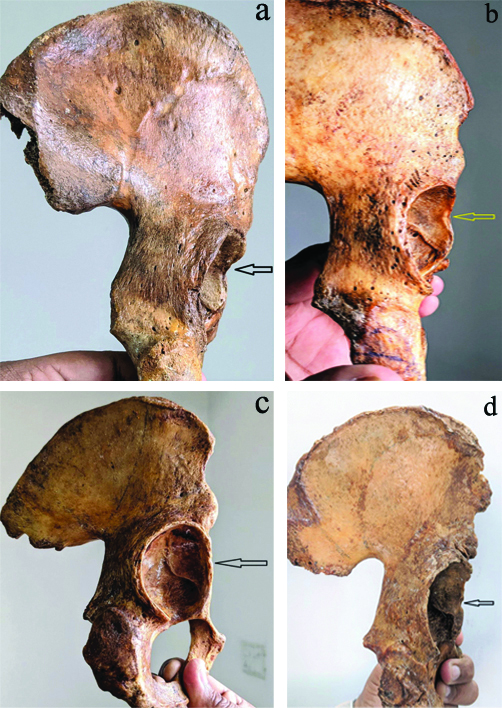
The morphology of anterior acetabular ridge in the study was evaluated. The shape of the anterior acetabular ridge was categorised into curved, angular, straight and irregular types [Table/Fig-3a-d] [11-14].
a) Angular shaped anterior acetabular ridge; b) Curved shaped anterior acetabular ridge; c) Straight shaped anterior acetabular ridge; d) Irregular shaped anterior acetabular ridge.
Statistical Analysis
The data collected for all parameters were entered in Microsoft Excel (version 2019) and analysed statistically to find range, mean, standard deviation and Student’s t-test was applied. Pearson’s test was used to evaluate the correlation between the diameter and depth of the acetabulum. The p-value <0.05 were considered as statistically significant. All data were analysed using statistical software SPSS version 16.0.
Results
The morphometric parameters (diameter and depth) of acetabulum presented in [Table/Fig-4] show the average values, standard deviation and maximum and minimum values of the parameters on right and left side. The average values of acetabular diameter and depth obtained in present study were 48.98±2.91 mm and 24.12±2.54 mm, respectively. The maximum and minimum diameter of acetabulum measured were 56 mm and 41 mm, respectively. The range of maximum and minimum acetabular depth in present study was from 30 mm to 20 mm. Range of maximum and minimum values of these parameters shows the variations in the normal population. Although the measurements of parameters on left side were slightly higher than the right side, there was no statistically significant difference between right and left side (p>0.05). There was a positive correlation between average dimensions of diameter and depth of the acetabulum (r-value -0.388; strength of correlation was weakly positive, p-value <0.001). Thus, it can be inferred that there is a possibility of increase in the depth of acetabulum, when diameter increases.
Depth and diameter of acetabulum in the present study.
| Parameters | Range | Mean±SD | p-value ‡between R and L |
|---|
| Right (n=54) | Left (n=50) | R+L (n=104) | Right (n=54) | Left (n=50) | R+L (n=104) |
|---|
| Diameter (in mm) | 41-56 | 43-55 | 41-56 | 48.76±2.94 | 49.2±2.92 | 48.98±2.91 | 0.283 |
| Depth (in mm) | 21-30 | 20-30 | 30-20 | 23.6±2.48 | 24.6±2.59 | 24.12±2.54 | 0.22 |
| Correlation between diameter and depth (R+L) | †r-value=0.388 | p-value <0.001** |
†Using Pearson’s correlation test; ‡Using Student’s t-test; **statistically highly significant; R: Right; L: Left
[Table/Fig-5] shows the frequency of different shapes of acetabular ridge. The most common shape of anterior acetabular ridge in present study was curved (63.46%) followed by angular shape (23.08%). The least common shape of acetabular margin observed in present study was straight type (2.88%).
Frequency of different shapes of anterior acetabular ridge in the present study.
| Shape of the anterior acetabular ridge | Frequency, n (%) |
|---|
| Angular | 24 (23.08%) |
| Curved | 66 (63.46%) |
| Straight | 3 (2.88%) |
| Irregular | 11 (10.58%) |
| Total | 104 (100%) |
Discussion
The primary objective of the study was to emphasise the significance of anthropometry of acetabulum. One of the essential preconditions for the normal biomechanics of hip joint is its normal shape. The abnormalities in the dimensions of acetabulum are important in understanding the pathology of hip joint diseases like primary osteoarthrosis [13]. The incongruous hip joint is more prone for degeneration than a joint having normal anatomy [5].
An effort has been made in the present study to examine the dry hip bones with the available data in relation to various parameters. The parameters were selected from the literature available in the previously published articles [11-14]. In order to get better insight on the results obtained, the present study was compared to some of the earlier investigations [Table/Fig-6] [12-19].
Comparison of depth and diameter of acetabulum with previous studies [12-19].
| S. No. | Authors | Year of publication | Population | Sample size | Diameter (mm) | Depth (mm) |
|---|
| 1. | Aksu F et al., [14] | 2006 | Turkey | 154 | 54.29±3.8 | 29.49±4.2 |
| 2. | Parmara G et al., [12] | 2013 | Indian | 100 | 42.54±3.6 | 19.07±2.47 |
| 3. | Devi TB and Philip CX, [13] | 2014 | Indian | 100 | 50.99±1.99 | 28.32±1.32 |
| 4. | Ukoha UU et al., [15] | 2014 | Nigerian | 100 | R-54.8±3.5L-53.9±3.0 | R-29.7±3.1L-30.2±3.1 |
| 5. | Khobragade L and Vatsalaswamy P, [16] | 2017 | Indian | 110 | - | 27.1±3.2 |
| 6. | Sreedevi G and Sangam MR, [17] | 2017 | Indian | 80 | R-49.4±3.52L-48.06±5.65 | R-24.09±2.84L-25.16±2.97 |
| 7. | Indurjeeth K et al., [18] | 2019 | Black African | 100 | 54.84±4.18 | 31.30±3.18 |
| 8. | Bahl I et al., [19] | 2020 | Indian | 73 | 48.6±3.5 | 27.1±3.2 |
| 9. | Present study | 2021 | Indian | 104 | 48.98±2.91 | 24.12±2.54 |
Aksu F et al., reported the average diameter of acetabulum in Turkish population as 54.29±3.8 mm [14]. In a study done by Ukoha UU et al., in the African population, the mean diameter was 54.8±3.5 mm and 53.9±3.0 mm on right and left side, respectively [15], closer to the results of Indurjeeth K et al., who also did study on African population [18]. But the studies done on Indian population by previous authors {Devi TB and Philip CX, Sreedevi G and Sangam MR, and Bahl I et al., [13,17,19]} revealed the average diameter around 49 mm which is similar to present study results. These differences in the results can be attributed to racial variations and Chauhan R et al., opined that smaller values of the acetabulum parameters are due to short stature of Indians when compared to Africans [11]. But Paramara G et al., reported average diameter as 42.54±3.6 mm in Indians which was lower when compared to present study [12]. Chauhan R et al., who measured the parameters on cadavers found the mean diameter as 47.10±2.90 mm (right side), 47.48±3.05 mm (left side) in males and 44.38±3.01 mm (right side), 46.0±2.28 mm (left side) in females which is more or less similar to present study findings on dry bones [11].
Acetabular depth is essential in maintaining normal hip mechanics and establishing a good range of movement. It acts as one of the contributing factors in component dislocation [16]. The acetabular depth has been considered by many investigators as an important measurement in defining acetabular dysplasia. The acetabulum with depth of less than 9 mm is regarded as acetabular dysplasia [20]. The average depth of acetabulum in present study was 24.12±2.54 mm which is similar to the findings of Sreedevi G and Sangam MR [17] but greater than the measurements done by Parmara G et al., as represented in [Table/Fig-6] [12]. Devi TB and Philip CX, Khobragade L and Vatsalaswamy P, and Bahl I et al., reported slightly higher values in Indian population when compared to the present study [13,16,19]. Aksu F et al., Ukoha UU et al., and Indurjeeth K et al., found higher values of mean depth of acetabulum but their studies were conducted on people from different races [14,15,18].
Chauhan R et al., after studying the diameter of both acetabulum and femoral head described that the average diameter of femoral head is smaller than the average diameter of acetabulum in North Indian cadavers so that the femoral head is snugly fitted into the acetabular depression which is one of the major reasons why primary osteoarthritis of hip joint is not so common in Indians [11].
The morphometric parameters measured in present study had a higher value on left side when compared to right side but were not statistically significant. According to Chhibber SR and Singh I, left limb was dominant [21]. More people use left lower limb for weight bearing, whether they are right-handed or left-handed. Hence, in order to bear greater loading force on femur on left side, the dimensions of the bones forming the hip joint of left side should be more than the right [21].
Thus, from the findings of the present study it can be inferred that, acetabular dimensions in Indian population were smaller when compared to other populations and measurements on left side were greater than right side since most people use left lower limb for weight bearing. The frequency of different shapes of anterior acetabular ridge in present study was in near coincidence with Devi TB and Philip CX, and Maruyama M et al., [13,22]. Present study observed curved type as the most common shape of anterior acetabular ridge similar to previous studies done on Indian population [12,13,17,19]. But Indurjeeth K et al., found angular shape to be the most common in African population [18]. This disparity in the findings could be attributed to racial variations [15]. Present study observed straight type as the least common shape of anterior acetabular ridge which is similar to Devi TB and Philip CX, and Bahl I et al., [13,19], whereas Sreedevi G and Sangam MR, and Pratibha K et al., noted irregular type in Indian population as the least common [Table/Fig-7] [12-15,17-19,22,23].
Comparison of shape of anterior acetabular ridge between present study and previous studies [12-15,17-19,22,23].
| Shape of anterior acetabular ridge (in percentage) | Maruyama M et al., 2001 [22] | Aksu F et al., 2006 [14] | Parmara G et al., 2013 [12] | Devi TB and Philip C, 2014 [13] | Ukoha UU et al., 2014 [15] | Pratibha K et al., 2015 [23] | Sreedevi G and Sangam MR, 2017 [17] | Indurjeeth K et al., 2019 [18] | Bahl I et al., 2020 [19] | Present study 2021 |
|---|
| Angular | 25.50 | 16.8 | Not found | 27 | 33 | 11.5 | 22.5 | 41 | 26 | 23.08 |
| Curved | 60.50 | 46.1 | 61 | 60 | 35 | 38.2 | 43.75 | 22 | 41.1 | 63.46 |
| Straight | 4.50 | 23.3 | 20 | 4 | 23 | 29 | 27.5 | 14 | 5.5 | 2.88 |
| Irregular | 9.50 | 13 | 19 | 9 | 9 | 21.3 | 6.25 | 23 | 27.4 | 10.58 |
The aetiopathogenesis of hip joint diseases like acetabular dysplasia and pincer femoro-acetabular impingement are often associated with variations in the morphology of acetabulum including the acetabular diameter, depth and orientation [24]. The total hip arthroplasty is one of the most common surgeries done now-a-days in the field of orthopaedics. The knowledge of anatomical parameters of hip joint reduces the complications arising from the mismatch of prosthesis in hip arthroplasty [13]. The significant information about the average dimensions of acetabulum and morphology of anterior acetabular ridge will help the surgeon to determine the ideal size of acetabular cup during total hip arthroplasty. Using acetabular cups that replicate the curvaceous acetabular profile could reduce the incidence of iliopsoas impingement and prevent prosthetic overlap and mechanical loosening [23].
Limitation(s)
Failure to discriminate between the genders of the bones was the major limitation of this study.
Conclusion(s)
The dimensions of acetabulum in Indians are smaller when compared to other populations and a weakly positive correlation between the mean values of acetabular diameter and depth was observed as per present study. Based on the findings of the current study, some amendments in the current knowledge of morphological and morphometric parameters of acetabulum were presented. Present study have provided a set of reference ranges for normal acetabular dimensions, which we believe, will be helpful for determining the safe position of acetabular implant during hip replacement surgery. Authors are hopeful that this study will also be valuable for the anthropologists in their racial and population studies.
†Using Pearson’s correlation test; ‡Using Student’s t-test; **statistically highly significant; R: Right; L: Left
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? No
For any images presented appropriate consent has been obtained from the subjects. No
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 04, 2020
Manual Googling: Jan 01, 2021
iThenticate Software: Jan 16, 2021 (14%)
[1]. Standring S, Gray’s Anatomy 2016 41st edNew YorkElsevier:1339-76. [Google Scholar]
[2]. Sinnatamby CS, Last’s Anatomy Regional and Applied 2006 11th edEdinburghChurchill Livingstone:169 [Google Scholar]
[3]. Menschik F, The hip joint as a conchoid shapeJ Biomech 1997 30(9):971-73.10.1016/S0021-9290(97)00051-1 [Google Scholar] [CrossRef]
[4]. Pun S, Hip dysplasia in the young adult caused by residual childhood and adolescent-onset dysplasiaCurr Rev Musculoskelet Med 2016 9(4):427-34.10.1007/s12178-016-9369-027613709 [Google Scholar] [CrossRef] [PubMed]
[5]. Murray RO, The aetiology of primary osteoarthritis of the hipBr J Radiol 1965 38:810-24.10.1259/0007-1285-38-455-8105842578 [Google Scholar] [CrossRef] [PubMed]
[6]. Hartofilakidis G, Stamos K, Karachalios T, Ioannidis TT, Zacharakis N, Congenital hip disease in adults. Classification of acetabular deficiencies and operative treatment with acetabuloplasty combined with total hip arthroplastyJ Bone Joint Surg Am 1996 78(5):683-92.10.2106/00004623-199605000-000078642024 [Google Scholar] [CrossRef] [PubMed]
[7]. Umer M, Thambyah A, Tan WTJ, Das DS, Acetabular morphometry for determining hip dysplasia in the Singaporean populationJ Orthop Surg 2006 14:27-31.10.1177/23094990060140010716598083 [Google Scholar] [CrossRef] [PubMed]
[8]. Tannast M, Siebenrock KA, Anderson SE, Femoroacetabular impingement: Radiographic diagnosis. What the radiologist should knowAJR 2000 188:1540-42.10.2214/AJR.06.092117515374 [Google Scholar] [CrossRef] [PubMed]
[9]. Vandenbussche E, Saffarini M, Taillieu F, Mutschler C, The asymmetric profile of the acetabulumClin Orthop Relat Res 2008 466(2):417-23.10.1007/s11999-007-0062-x18196426 [Google Scholar] [CrossRef] [PubMed]
[10]. Bricteux S, Benguin L, Fessy MH, Iliopsoas impingement in 12 patients with a total hip arthroplastyRev Chir Orthop Reparatrice Appar Mot 2001 87:820-25. [Google Scholar]
[11]. Chauhan R, Paul S, Dhaon BK, Anatomical parameters of North Indian hip joints- Cadaveric studyJ Anatomical Society of India 2002 51:39-42. [Google Scholar]
[12]. Parmara G, Rupareliab S, Patelc SV, Patelb SM, Jethvaa N, Morphology and morphometry of acetabulumInt J Biol Med Res 2013 4(1):2924-26. [Google Scholar]
[13]. Devi TB, Philip CX, Acetabulum- Morphological and morphometrical studyRes J Pharmaceutical, Biological and Chemical Sciences 2014 5(6):793-99. [Google Scholar]
[14]. Aksu F, Gulrizceri N, Arma C, Tetik S, Morphology and morphometry of acetabulumJournal of Dokuz Eylul University Medical Faculty 2006 20(3):143-48. [Google Scholar]
[15]. Ukoha UU, Umeasalugo KE, Okafor JI, Ndukwe GU, Nzeakor HC, Ekwunife DO, Morphology and morphometry of dry adult acetabula in NigeriaRev Arg de Anat Clin 2014 6(3):150-55.10.31051/1852.8023.v6.n3.14139 [Google Scholar] [CrossRef]
[16]. Khobragade L, Vatsalaswamy P, Morphometric study of depth of acetabulumInternational Journal of Research in Medical Sciences 2017 5(9):3837-42.10.18203/2320-6012.ijrms20173660 [Google Scholar] [CrossRef]
[17]. Sreedevi G, Sangam MR, The study of morphology and morphometry of acetabulum on dry bonesInt J Anat Res 2017 5(4.2):4558-62.10.16965/ijar.2017.395 [Google Scholar] [CrossRef]
[18]. Indurjeeth K, Ishwarkumar S, De Gama BZ, Ndlazi Z, Pillay P, Morphometry and morphology of the acetabulum within the black African population of South AfricaInt J Morphol 2019 37(3):971-76.10.4067/S0717-95022019000300971 [Google Scholar] [CrossRef]
[19]. Bahl I, Jyothi KC, Shetty S, Morphological and morphometrical study of the human acetabulum and its clinical implicationsInt J Current Res Rev 2020 12(10):01-04.10.31782/IJCRR.2020.12101 [Google Scholar] [CrossRef]
[20]. Saikia KC, Bhuyan SK, Rongphar R, Anthropometric study of the hip joint in northeastern region population with computed tomography scanIndian J Orthop 2008 42(3):260-66.10.4103/0019-5413.3957219753150 [Google Scholar] [CrossRef] [PubMed]
[21]. Chhibber SR, Singh I, Asymmetry in muscle weight and one-sided dominance in the human lower limbsJ Anat 1970 106(Pt 3):553-56. [Google Scholar]
[22]. Maruyama M, Feinberg JR, Capello WN, D’Antonio JA, Morphologic features of the acetabulum and femur: Anteversion angle and implant positioningClin Orthop Relat Res 2001 393:52-65.10.1097/00003086-200112000-00006 [Google Scholar] [CrossRef]
[23]. Pratibha K, Hema L, Devishankar Acetabulum of the hip bone: A morphometric study in south coastal regionInt J Recent Trends in Science and Technology 2015 17(2):136-39. [Google Scholar]
[24]. Zeng Y, Wang Y, Zhu Z, Tang T, Dai K, Qiu S, Differences in acetabular morphology related to side and sex in a Chinese populationJ Anat 2012 220:256-62.10.1111/j.1469-7580.2011.01471.x22233354 [Google Scholar] [CrossRef] [PubMed]