Palliative Management of Sarcomatoid Buccal Carcinoma by Laser Ablation
Rusy S Bhalla1, Seemantini Bhalla2
1 Consultant, Department of Oncology, Orchid Center for Laser Surgery, Mumbai, Maharashtra, India.
2 Laser ENT Surgeon, Department of Oncology, Orchid Center for Laser Surgery, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Rusy S Bhalla, 803, Tripoli Skyline Oasis, Premier Road Vidyavihar West, Mumbai, Maharashtra, India.
E-mail: rusybhalla@gmail.com
Sarcomatoid change in buccal carcinoma is a rare and aggressive variant of Squamous Cell Carcinoma (SCC) and most often a diagnostic dilemma. There are some reports of second primary sarcomatous tumours in the oral cavity and nasopharynx post irradiation. Synchronous and metachronous lesions in this category in the oral cavity and neck have also been reported. Spindle cell neoplasms comprise a diverse collection of benign and malignant tumours. These tumours are uncommon in the oral cavity, accounting for <1% of all tumours of oral region. It is an unusual aggressive variant that frequently recurs and metastasises. Herein, the author present a case report of a 45-year-old Indian male with a sarcomatoid lesion according to his previous reports in the oral cavity of five months duration at presentation. The patient presented late as he was not willing for surgery and hence a very extensive 9×5 cm lesion was observed. In addition, he had trismus, multiple, firm, fixed lymph nodes in the ipsilateral neck. The biopsy of the oral cavity tumour showed a histological appearance of spindle shaped cells with penetration of basement membrane suggestive of sarcomatoid carcinoma. He was treated with repeated ablative laser technique for the primary and metastatic nodes in the neck disease and chemotherapy. The patient resumed normal activities 14 days after the laser ablation.
Laser in oral cancer, Oral carcinoma, Sarcomatoid carcinoma, Squamous cell carcinoma
Case Report
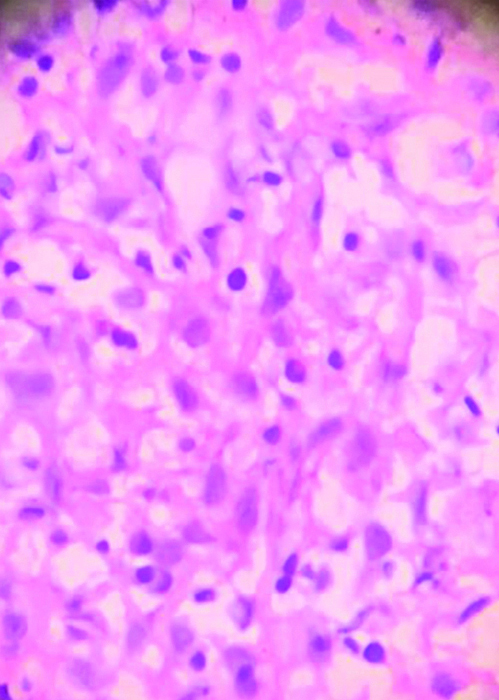
A 45-year-old male reported to the Department of Oral Cancer with an ulcerated and prolypoidal growth in the oral cavity for five months which was diagnosed as sarcomatoid lesion in the oral cavity on biopsy [Table/Fig-1,2]. There was a history of tobacco chewing in the form of gutka several times a day for 15 years prior to presentation. There was no history of smoking. He presented late after five months of diagnosis as he was not willing for surgery and hence a very extensive 9×5 cm lesion was observed. Oral hygiene was unsatisfactory. In addition, he had multiple lymph nodes in the ipsilateral neck.
H&E sections showing sarcomatoid carcinoma (X400).
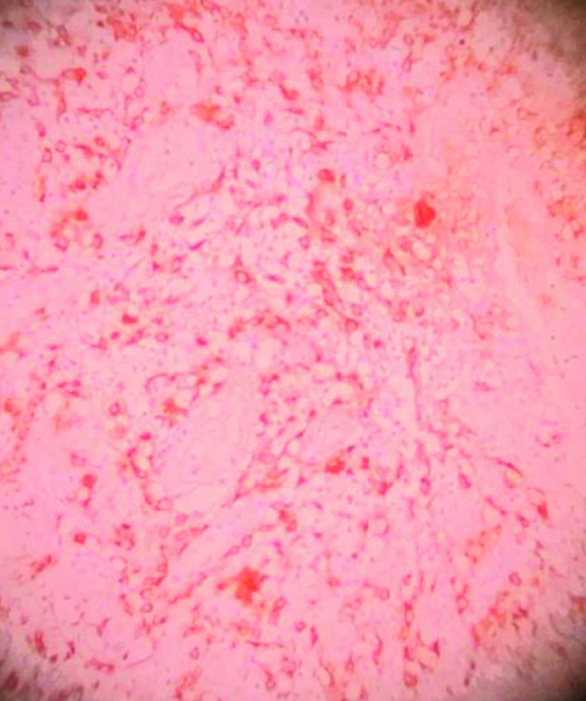
Single and spindle cells expressing pan Cytokeratin (CK) on Immunohistocytochemistry (IHC) (X100).
This patient presented with a gradual increasing swelling on left side of face. He had a huge tumour 9×5 cm inside his left buccal cavity with extension on the lip and angle of mouth. On examination he showed an ulceroproliferative and polypoid reddish-brown lesion extending from retromolar area to angle of mouth. He had trismus (less than 1 cm mouth opening). There was a loss of weight of 8 kg in last two months [Table/Fig-3,4].
Showing swollen left side of the face with involvement of angle of mouth.

Showing full extension of the lesion.

The patient had a history of frequent bleeding from mouth for two weeks at presentation. There was a clear difference in appearance between the anterior reddish firm part and the posterior brownish spongy part [Table/Fig-4].
Patient had nasotracheal intubation under general anaesthesia. The tumour and the lymph nodes were ablated using the 980 nm surgical diode by Gigaa lasers under sonography guided imaging.
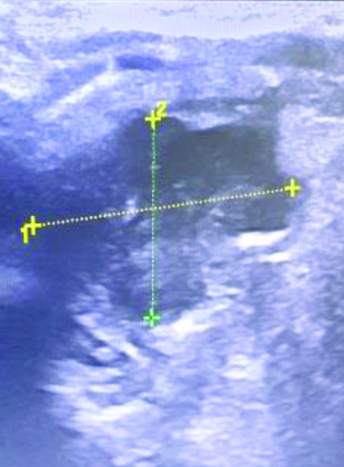
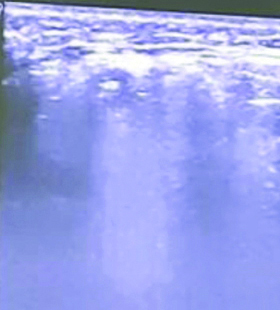
Repeated laser ablations were carried out on a weekly basis under local anaesthesia and sonography guided imaging for a period of three months (making a total of 12 sessions). The first laser procedure was of two hours duration while subsequent procedures under local anaesthesia ranged from 5 to 10 minutes. The completeness of laser ablation was seen by the tumour becoming hyperechogenic from hypoechogenic in observation on real time basis [Table/Fig-5,6]. Concurrent chemotherapy sessions with Cisplatin, Paclitel and 5 FU in standard dose were administered every three weeks for a period of six months. MRI study was carried out every two months after primary procedure to detect regression of the disease.
Pre laser figure shows a hypoechoic malignant area.
Post laser ablation area is hyperechoic.
Patient was pain free within 24 hours of primary laser procedure. No bleeding seen after 24 hours. Within 24 hours he was on soft diet and full diet within a week. He was discharged in three days. His speech improved considerably. Swelling reduced gradually in two months. He got back to his work in four weeks and had 20 kg weight gain in one year.
The intraoral tumour regressed by necrosis and detachment. Small areas of recurrence/residual tumour showed regression after repeat laser and concurrent chemotherapy. The lymph nodes were not palpable after two months of primary laser procedure.
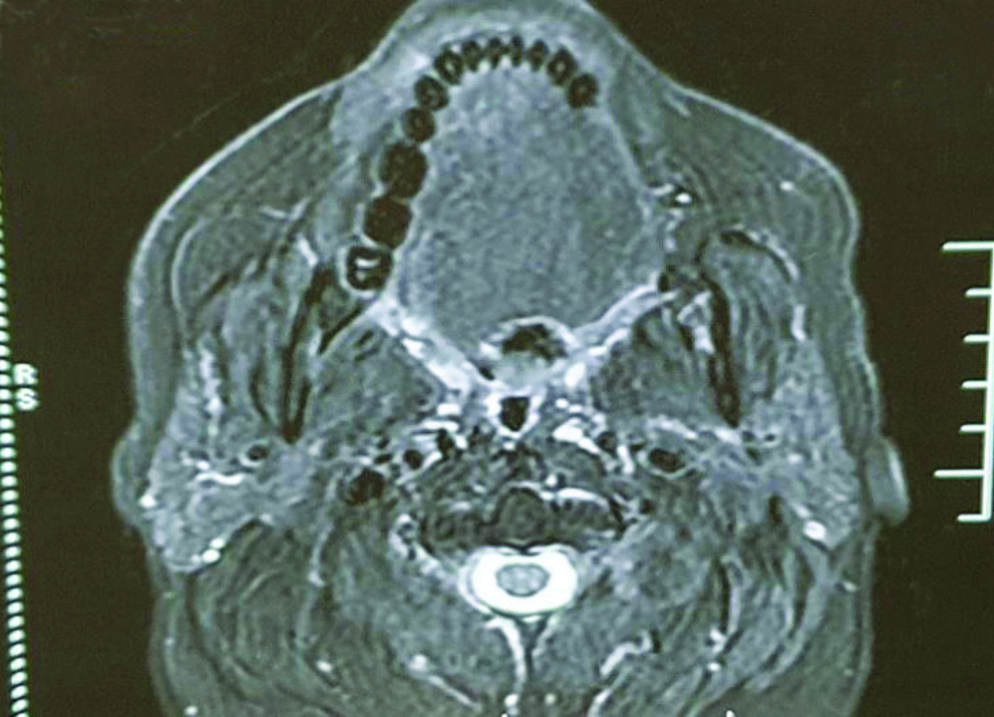
Serial MRI findings were consistent with gradual regression of the disease in the oral cavity and the neck [Table/Fig-7,8].
MRI Pre laser shows a large lesion extending from angle of mouth to Retromolar Trigone Area.
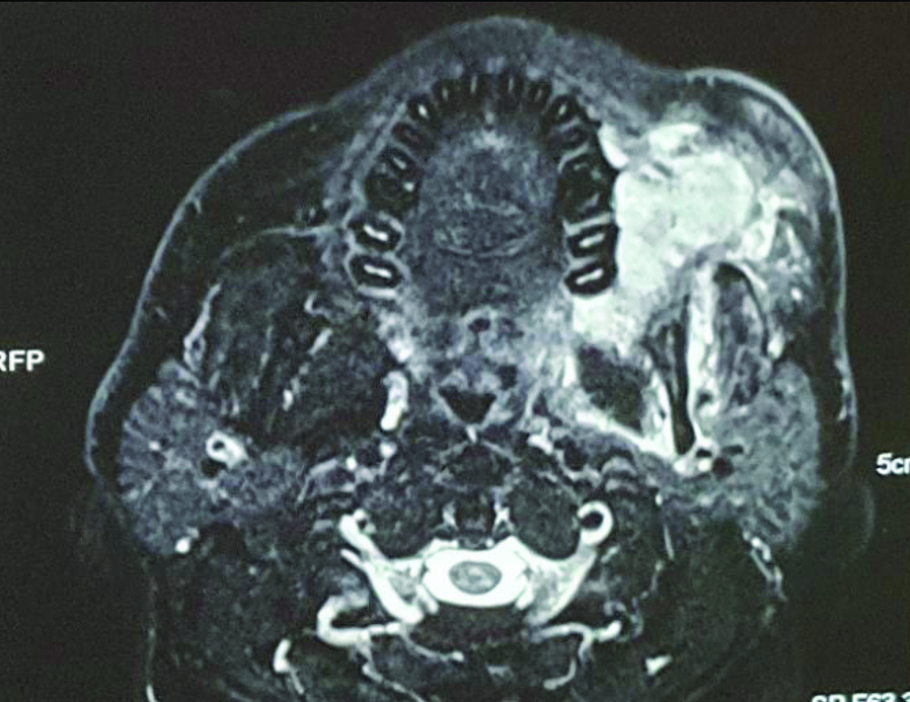
MRI post laser after one year shows total resolution of the lesion.
Discussion
Tobacco plays an important part in causation of oral cancers. Oral cancer is the leading cancer in males in India [1]. The carcinogens in tobacco belong to multiple chemical classes, including Polycyclic Aromatic Hydrocarbons (PAHs), N-nitrosamines, aromatic amines, aldehydes, volatile organic hydrocarbons, and metals. In addition to these well-established carcinogens, others have been less thoroughly investigated. These include alkylated PAHs, oxidants, free radicals, and ethylating agents [2].
Spindle cell neoplasms comprise a diverse collection of benign and malignant tumours. These tumours are uncommon in the oral cavity, accounting for <1% of all tumours of oral region.
Sarcomatoid Squamous Cell Carcinoma (SSCC), also known as spindle cell carcinoma or Lane’s tumour, is a rare and peculiar biphasic malignant neoplasm that occurs mainly in the upper aerodigestive tract. It is a variant of SCC which has spindled or pleomorphic tumour cells which simulate a true sarcoma, but are epithelial in origin. They undergo metaplasia to change into spindle cell sarcomas. Sarcomatoid carcinoma is an aggressive disease and recurrence and early metastasis are common [3,4]. They have a worse prognosis than standard SCCs. They are more aggressive and have a tendency to metastasise early [3]. It has a different gross appearance from normal SCC. Sarcomatoid carcinoma develops in existing SCC and has a reddish brown, polypoid and fleshy appearance. The tumour has surface ulceration with necrosis and areas of bleeding [5]. It is a rare variant and very often a diagnostic dilemma [6]. In addition to it being a challenge in terms of diagnostic dilemma management of sarcomatoid carcinoma is equally tricky and controversial [5].
Conventional treatment includes surgery in early stages and chemotherapy with or without radiotherapy [7,8]. Radiation though sometimes used as treatment can add to a poor prognosis [9]. This may be since it has a probability of increasing the aggressiveness of the lesion [10].
Different treatment regimens have been proposed for this condition. In late cases, chemotherapy and immunotherapy is the treatment of choice. The prognosis has been bad for patients presenting late. Poor prognosis has been reported in patients treated with radiotherapy, which is considered to be ineffective although adjuvant irradiation may be beneficial in patients who have positive surgical margins or who have nodal metastasis at the time of diagnosis [11]. Chemotherapy is also an important adjuvant primary treatment as well as treatment of metastasis. The mean survival time of the patients who died of sarcomatoid cancer was 1.9 years. This is generally dependent on size and site of the tumour [12]. Immunotherapy has been used with some success in metastasis of sarcomatoid tumours in sites outside oral cavity by Salati M et al., [8].
Laser ablation is now recognised as an alternative to excision in many soft tissue tumours. In our extensive research we could not find any instance of laser ablation being used for sarcomatoid tumours, though it is routinely used for Oral Carcinomas [13,14]. Prognosis is better for small sized lesions and is obviously poor for large unresectable lesions [10]. Laser ablation works by heat induced destruction of cancer cells as well as vascular thrombosis and protein denaturation of cellular proteins of heat affected cells [15].
Judicious use under sonography control can be used to kill a majority of the tumour. This can be followed by chemotherapy for a good palliation and remission [Table/Fig-3,4,9,10].

No sign of cancer after 14 months.

The present patient presented a dilemma for management as we had not handled a sarcomatoid lesion of this size previously. Our previous attempts at single session of laser had not suceeded. In this patient we decided on a repeated weekly approach, followed by chemotherapy for a total of six cycles.
Here the author believe that multiple laser ablation sessions can be employed as an alternative in unresectable carcinoma and sarcomatoid lesions of oral cavity. More research is needed to establish this as a routine alternative to standard palliation of chemotherapy and radiotherapy in other oral cancers also.
Conclusion(s)
Laser is an additional modality which is gradually being accepted in management of soft tissue tumours. The ability of laser to burn and necrose the tumour mass helps in decreasing the tumour load. The procedure has to be repeated in large tumours for a good result.
Sarcomatoid carcinoma in late stages is a bad prognosis. The addition of laser ablation and chemotherapy has been an important factor in a good remission in this case.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 07, 2020
Manual Googling: Nov 07, 2020
iThenticate Software: Jan 15, 2021 (15%)
[1]. National Centre for Disease Informatics and Research. https://ncdirindia.org/ncrp/All_ncrp_reports/Pbcr_report_2012_2014/All_content/Printed_Version.htm. Bengaluru; 2016 [Google Scholar]
[2]. Centers for Disease Control and Prevention (US); National Center for Chronic Disease Prevention and Health Promotion (US); Office on Smoking and Health (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention (US); 2010. 5, Cancer. Available from: https://www.ncbi.nlm.nih.gov/books/NBK53010/4 [Google Scholar]
[3]. Shah BJ, Tupkari JV, Joy T, Sarcomatoid squamous cell carcinoma of mandible: A report of two casesJ Oral Maxillofac Pathol 2019 23(1):163 [Google Scholar]
[4]. Bavle RM, Govinda G, Gundappanayakanahalli P, Venkataramanaiah Muniswamappa S, Venugopal R, Fallacious carcinoma-spindle cell variant of squamous cell carcinomaJ Clin Diagn Res 2016 10(7):ZD05-08.10.7860/JCDR/2016/16400.809927630965 [Google Scholar] [CrossRef] [PubMed]
[5]. Kwon GY, Chol YJ, Song MS, Yun KI, Sarcomatoid carcinoma of the mandible: Report of a caseJournal of the Korean Association of Oral and Maxillofacial Surgeons 2010 36(3):228-30.10.5125/jkaoms.2010.36.3.228 [Google Scholar] [CrossRef]
[6]. Mahajan A, Mohanty S, Ghosh S, Urs AB, Khurana N, Gupta S, Sarcomatoid carcinoma of the oral cavity: A diagnostic dilemmaCase Rep Dent 2017 2017:7495695Epub 2017 Dec 1710.1155/2017/749569529527362 [Google Scholar] [CrossRef] [PubMed]
[7]. Reyes M, Pennacchiotti G, Valdes F, Montes R, Veloso M, Angélica M, Sarcomatoid (Spindle Cell) carcinoma of tongue: A report of two casesCase Rep Dent 2015 2015:78085610.1155/2015/78085625785207 [Google Scholar] [CrossRef] [PubMed]
[8]. Salati M, Baldessari C, Calabrese F, Rossi G, Pettorelli E, Grizzi G, Nivolumab-induced impressive response of refractory pulmonary sarcomatoid carcinoma with brain metastasisCase Rep Oncol 2018 11:615-21.10.1159/00049266630323751 [Google Scholar] [CrossRef] [PubMed]
[9]. Leventon GS, Evans HL, Sarcomatoid squamous cell carcinoma of the mucous membranes of the head and neck: A clinicopathologic study of 20 casesCancer 1981 48:994-1003.10.1002/1097-0142(19810815)48:4<994::AID-CNCR2820480424>3.0.CO;2-M [Google Scholar] [CrossRef]
[10]. Berthelet E, Shenouda G, Black MJ, Picariello M, Rochon L, Sarcomatoid carcinoma of the head and neckAm J Surg 1994 168:455-58.10.1016/S0002-9610(05)80098-4 [Google Scholar] [CrossRef]
[11]. Sumida T, Otawa N, Kamata YU, Yamada T, Uchida K, Nakano H, A clinical investigation of oral sarcomas at multi-institutions over the past 30 yearsAnti cancer Research 2015 35(8):4551-55. [Google Scholar]
[12]. Iqbal MS, Paleri V, Brown J, Greystoke A, Dobrowsky W, Kelly C, Spindle cell carcinoma of the head and neck region: Treatment and outcomes of 15 patientsEcancermedicalscience 2015 9:594Published 2015 Nov 1810.3332/ecancer.2015.59426635898 [Google Scholar] [CrossRef] [PubMed]
[13]. Schena E, Saccomandi P, Fong Y, Xu B, Laser ablation for cancer: Past, present and futureJ Funct Biomater 2017 8(2):1910.3390/jfb802001928613248 [Google Scholar] [CrossRef] [PubMed]
[14]. Azma E, Safavi N, Diode laser application in soft tissue oral surgeryJ Lasers Med Sci 2013 4(4):206-11. [Google Scholar]
[15]. Lanzafame RJ, Laser/Light Applications in General Surgery. In: Nouri K. (eds)Lasers in Dermatology and Medicine 2018 ChamSpringer10.1007/978-3-319-76220-3_7 [Google Scholar] [CrossRef]