Fibular Aplasia, Tibial Campomelia, Oligo-Syndactyly Syndrome and Probable Femur Fibula Ulna Syndrome- Case Reports
S Prathyusha Kavipurapu1, Madhuri Maganthi2, LG Shyam Sundar3, S Ramya4
1 Postgraduate, Department of Paediatrics, Bangalore Baptist Hospital, Bangalore, Karnataka, India.
2 Consultant, Department of Paediatrics, Bangalore Baptist Hospital, Bangalore, Karnataka, India.
3 Consultant, Department of Orthopaedic, Bangalore Baptist Hospital, Bangalore, Karnataka, India.
4 Consultant, Department of Paediatrics, Bangalore Baptist Hospital, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prathyusha Kavipurapu, Department of Paediatric, Bangalore Baptist Hospital, Bellary Road, Hebbal, Bangalore-560024, Karnataka, India.
E-mail: prathyusha.ks8@gmail.com
One in two thousand neonates suffer from congenital limb deficiencies. Fibular hemimelia, a birth defect, has an estimated incidence of 5.7 to 20 cases per 1 million births. Fibular Aplasia, Tibial Campomelia and Oligo-Syndactyly (FATCO) syndrome is one such which is a triad of fibular hemimelia (aplasia/hypoplasia of fibula), tibial campomelia (bending of tibial bone) and oligo syndactyly. It is a syndrome of unknown genetic basis and inheritance. Very few cases on this condition have been reported so far. This article reports two cases on this condition, wherein the babies had considerable variability of limb malformations. The first is a newborn with FATCO, and the second is a two-month-old male infant with FATCO associated with right focal femoral deficiency. In view of paucity of the cases, there is a need to report every case which may help in creating awareness and a standardised management approach.
Femoral deficiency, Fibular hemimelia, Oligo-syndactly
Case Report 1
This case report shows a male new-born who was the, second born child of a consanguineously married couple of Indian lineage. There was no significant family history and the antenatal events and scans were normal. The child was delivered by normal vaginal delivery at term with a birth weight of 2.48 kg with no immediate neonatal complications.
Physical examination revealed 3,4,5 syndactyly in the right hand [Table/Fig-1] and oligodactyly in the left hand (3 finger) [Table/Fig-2]. Shortening and anterolateral bowing of the left lower limb at the distal third of the tibia with associated overlying soft tissue dimpling [Table/Fig-3] was noted, ankle was in equinus. Right leg, ankle and foot were normal. There was no facial dysmorphism.
Syndactyly of right upper limb.

Oligodactyly of left upper limb.

Shortening and bowing of left lower limb, with overlying skin dimpling.

Radiological findings reported fibular aplasia [Table/Fig-4] and tibial campomelia [Table/Fig-5] of left lower limb and ultrasonography of spine revealed spina bifida occulta. Parents refused further evaluation of the baby. It was reported that the baby died at six months. The cause of death is not known as the baby was lost to follow-up.
X-ray showing complete absence of fibula on the left lower limb (Fibular aplasia).
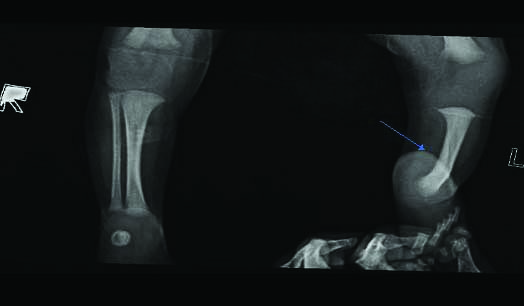
Lateral view X-ray showing bowing of the tibia in the left lower limb (Tibial campomelia).

Case Report 2
The second case is of a two-month-old male infant, born to nonconsanguineous couple of Iranian lineage. A right focal femoral deficiency was detected antenatally. There was no history of trauma, teratogenic exposure antenatally and family history was not significant. The child was delivered by Cesarean section (LSCS) at 33 weeks of gestation, with a birth weight of 2.1 kg. The baby had no immediate neonatal complications and was noticed to have grossly shortened right lower limb with anteromedial bowing, overlying skin dimple, equinovalgus foot with oligo-syndactyly (4 toes were present with fused 1,2 and 3,4 toes) [Table/Fig-6].
Shortening and bowing of right Lower limb, with overlying skin dimpling limb oligosyndactyly.

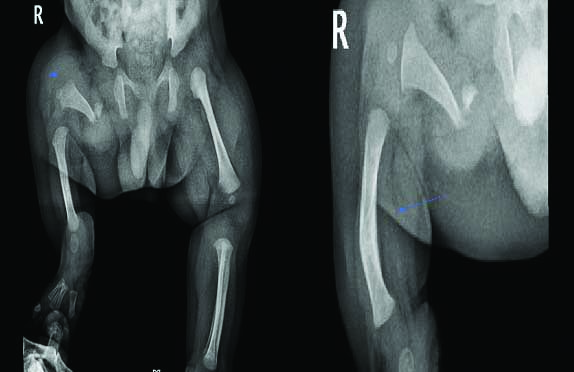
Oligodactyly was present in left foot (4 toes were present) [Table/Fig-7]. Both the upper limbs were normal. X-ray showed proximal focal femoral deficiency, total absence of fibula, anteromedial bowing of tibia (campomelia) of right lower limb [Table/Fig-8]. A written consent was obtained from the mother. Orthopaedic review was done, and parents were explained about the need for staged surgery at a later date. Summary of the clinical and radiological findings of the two cases is given in [Table/Fig-9].
Left lower limb showing oligodactyly.

X-ray showing proximal focal femoral deficiency, total absence of fibula, anteromedial bowing of tibia (campomelia) of right lower limb.
Summary of the clinical and radiological findings of the two cases.
| Age | Case 1Newborn | Case 22 months |
|---|
| Gender | Male | Male |
| Consangunity | Yes | No |
| Right upper limb | 3,4,5 Syndactyly | Normal |
| Right lower limb | Normal | Clinical:- oligo syndactyly (4 toes).fused 1,2 and 3,4 toes)- shortening and bowing of the limb with overlying dimpling of skinRadiograph:- short and dysplastic femur (focal femoral deficiency)- fibular aplasia- tibialcampomelia |
| Left upper limb | Oligodactyly (3 Fingered Hand With Thumb) | Normal |
| Left lower limb | Clinical:-Shortening and anterolateral bowing at the distal third of the tibia with associated overlying soft tissue dimpling - Limb length discrepancy- Radiograph: - Fibularaplasia- Tibia campomelia | Oligodactyly (4 Toes) |
| Other associations | Spina Bifida Occulta | Right Proximal Focal Femoral Deficiency (PFFD) |
| Antenatal detection of the skeletal deformity | No | Yes |
Discussion
With the above clinical and radiological evidence, two cases with a rare congenital limb defect, a characteristic triad of FATCO syndrome with other associated anomalies were reported.
Congenital limb deficiencies are common birth defects, with an incidence of 1 in 2000 neonates [1]. Fibular hemimelia comprises a spectrum of malformations ranging from fibular hypoplasia to fibular aplasia with an incidence of approximately 5.7 to 20 cases per one million births [2].
Three types of hemimelia are described in the literature [3]: Type I includes cases with unilateral or partial absence of the fibula with mild or no bowing of tibia (10% of cases). Type II includes cases with unilateral absence of the fibula, anterior bowing of the tibia with skin dimpling, and foot deformity with absent rays and marked shortening of the leg (35% of cases). Type III has unilateral or bilateral absence of the fibula, with same leg and foot deformities and multiple skeletal defects (55% of cases). Type II hemimelia is seen in both the index cases. Fibular hemimelia usually occurs unilaterally, isolated, and sporadic [4,5].
The exact aetiology is unclear, but the majority are found to be caused by nongenetic causes such as radiation and teratogens [5]. A proposed theory is that of a disruption of the lower limb developmental field during embryogenesis [5] due to interference with limb bud development at about the 5th or 7th week of intrauterine life.
Courtens W et al., reported the first ever case of a male baby with oligosyndactyly of the left hand and the right foot with absence of the right fibula [5], and anterior bowing of the ipsilateral tibia with associated overlying soft tissue dimpling and reviewed four other cases [4,6,7]. Since all the five reported cases had a triad of findings- fibular aplasia, tibial campomelia, and oligosyndactyly, the name FATCO syndrome was proposed.
Both the cases presented match the radiological description of classical FATCO syndrome, with other associated malformations. The close differentials of FATCO are Furhmann syndrome comprising of aplasia/hypoplasia of fibula, femur, ulna, oligo/poly dactyly and dysplastic nails and Al Awadi syndrome, with various degrees of limb aplasia/hypoplasia and joint dysplasis [8]. All previously reported cases of FATCO syndrome demonstrated a great clinical variability and male sex predilection as in the presented cases.
So far, two patients have been diagnosed prenatally [9,10]. Although, the usual occurrence is sporadic, autosomal dominance with reduced penetration or X-linked inheritance have been proposed by Biegansky T et al., [11]. Though autosomal recessive inheritance and gonodal mosaicism have been proposed by Hecht JT and Scott JR [6], the exact aetiology is not known. Molecular analysis could not be done in the current cases as parents were not willing. In addition, fibular hemimelia is often associated with other skeletal malformations like PFFD which is the most common, occuring in around 20% of patients [12].
Such syndromes having features of both PFFD and fibular hemimelia are described in the literature as the ‘Femur–fibula–ulna (FFU) syndrome’ or complex [13]. However, later femur and fibula defects with normal arms (without ulna involvement) were also included in the same category [13]. The second patient probably belongs to this category and amongst rare Indian cases to be reported as FFU syndrome. The main line of management is the preservation of the foot and equalisation of the limb length and is individualised from case to case.
Conclusion(s)
To conclude, reported here are two cases with FATCO syndrome, with a triad of fibular aplasia, tibial campomelia, oligo-syndactyly; a rare entity with very limited literature available from Indian subcontinent. Reporting every case may help in knowing the wide variation in the involvement of different bones and guides us in analysing the etiology to plan prevention and to optimize the management.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? No (parents lost to follow-up)
For any images presented appropriate consent has been obtained from the subjects. No (no identity was revealed in any form in the manuscript)
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Aug 01, 2020
Manual Googling: Dec 02, 2020
iThenticate Software: Jan 15, 2020 (23%)
[1]. Wilcox WR, Coulter CP, Schmitz ML, Congenital limb deficiency disordersClinics in Perinatology 2015 42(2):281-300.10.1016/j.clp.2015.02.00426042905 [Google Scholar] [CrossRef] [PubMed]
[2]. Florio I, Wisser J, Huch R, Huch A, Prenatal ultrasound diagnosis of a femur-fibula-ulna complex during the first half of pregnancyFetal Diagnosis and Therapy 1999 14(5):310-12.10.1159/00002094610529577 [Google Scholar] [CrossRef] [PubMed]
[3]. Parada S, Congenital absence of fibula2001-01-19-16. http://sonoworld.com/fetus/page.aspx?id=342.Google Scholar [Google Scholar]
[4]. Lewin SO, Opitz JM, Reynolds JF, Fibular a/hypoplasia: Review and documentation of the fibular developmental fieldAmerican Journal of Medical Genetics 1986 25(S2):215-38.10.1002/ajmg.13202506263146293 [Google Scholar] [CrossRef] [PubMed]
[5]. Courtens W, Jespers A, Harrewijn I, Puylaert D, Vanhoenacker F, Fibular aplasia, tibial campomelia, and oligosyndactyly in a male newborn infant: A case report and review of the literatureAmerican Journal of Medical Genetics Part A 2005 134(3):321-25.10.1002/ajmg.a.3044115754355 [Google Scholar] [CrossRef] [PubMed]
[6]. Hecht JT, Scott JR, Limb deficiency syndrome in half-sibsClinical Genetics 1981 20(6):432-37.10.1111/j.1399-0004.1981.tb01054.x7337959 [Google Scholar] [CrossRef] [PubMed]
[7]. Huber J, Volpon JB, Ramos ES, Fuhrmann syndrome: Two Brazilian casesClinical Dysmorphology 2003 12(2):85-88.10.1097/00019605-200304000-0000212868468 [Google Scholar] [CrossRef] [PubMed]
[8]. Ekbote AV, Danda S, A case report of fibular aplasia, tibial campomelia, and oligosyndactyly (FATCO) syndrome associated with Klinefelter syndrome and review of the literatureFoot & Ankle Specialist 2012 5(1):37-40.10.1177/193864001142259421965580 [Google Scholar] [CrossRef] [PubMed]
[9]. Capece G, Fasolino A, Monica MD, Lonardo F, Scarano G, Neri G, Prenatal diagnosis of femur-fibula-ulna complex by ultrasonography in a male fetus at 24 weeks of gestationPrenatal Diagnosis 1994 14(6):502-05.10.1002/pd.19701406167937589 [Google Scholar] [CrossRef] [PubMed]
[10]. Sezer O, Gebesoglu I, Yuan B, Karaca E, Gokce E, Gunes S, Fibular aplasia, tibial campomelia, andoligosyndactyly: A further patient with a 2-year follow-upClinical Dysmorphology 2014 23(4):121-26.10.1097/MCD.000000000000005125144151 [Google Scholar] [CrossRef] [PubMed]
[11]. Bieganski T, Jamsheer A, Sowinska A, Baranska D, Niedzielski K, Kozlowski K, Three new patients with FATCO: Fibular agenesis with ectrodactylyAmerican Journal of Medical Genetics 2012 158(7):1542-50.10.1002/ajmg.a.3536922628253 [Google Scholar] [CrossRef] [PubMed]
[12]. Schatz SL, Kopits SE, Proximal femoral focal deficiencyAmerican Journal of Roentgenology 1978 131(2):289-95.10.2214/ajr.131.2.28998010 [Google Scholar] [CrossRef] [PubMed]
[13]. Lenz W, Feldmann U, Unilateral and asymmetric limb defects in man: delineation of the femur-fibula-ulna complexBirth defects original article series 1977 13(1):269-85. [Google Scholar]