Cholesteatoma Masquerading as Cerumen
S Prabakaran1, RB Namasivaya Navin2, R Guna Keerthana3, S Rajasekaran4, K Priya5
1 Assistant Professor, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
2 Senior Resident, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
3 Junior Resident, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
4 Professor and Head, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
5 Professor, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. S Prabakaran, 3/286, Pachaiyappar Street, Periyar Salai, Palavakkam, Chennai-41, Tamil Nadu, India.
E-mail: somu.prabakaran@gmail.com
Cerumen is composed of glandular secretions and desquamated epithelial cells. It protects and lubricates the external auditory canal. Impacted cerumen causes canal occlusion and pressure over the tympanic membrane, causing ear discomfort, conductive hearing loss, itching, etc. Up to 6% of the general population are affected with impacted cerumen, which includes 10% of children, more than 30% of the elderly and people with cognitive impairment. Persistent symptoms despite resolution of impaction and patient repeatedly should raise suspicion of alternative diagnosis and prompt for further evaluation. A 20-year-old female patient came with complaints of decreased hearing and ear discharge. On otoscopic examination of left ear, impacted cerumen was seen in the attic region. On removal of wax with the aid of oto-endoscopy, attic region was found to be filled with cholesteatoma debris. On pure tone audiometry, patient had mild conductive hearing loss of 30db and computed tomography of left temporal bone revealed ill-defined soft tissue density in the middle ear (epitympanum) with erosion of head of malleus and short process of incus. Blunting of scutum was also seen. Attic reconstruction and type III tympanoplasty was performed. On histopathological examination, the section showed keratin flakes with bacterial colonies which were consistent with cholesteatoma. In conclusion, any case of impacted cerumen should not be ignored by otorhinolaryngologist. Further evaluation with thorough examination under otomicroscope/otoendoscope has to be done which can lead to different diagnosis and treatment plan.
Attic cholesteatoma, Atticotomy, Bony erosion, Impacted wax, Scutum, Tympanomeatal flap
Case Report
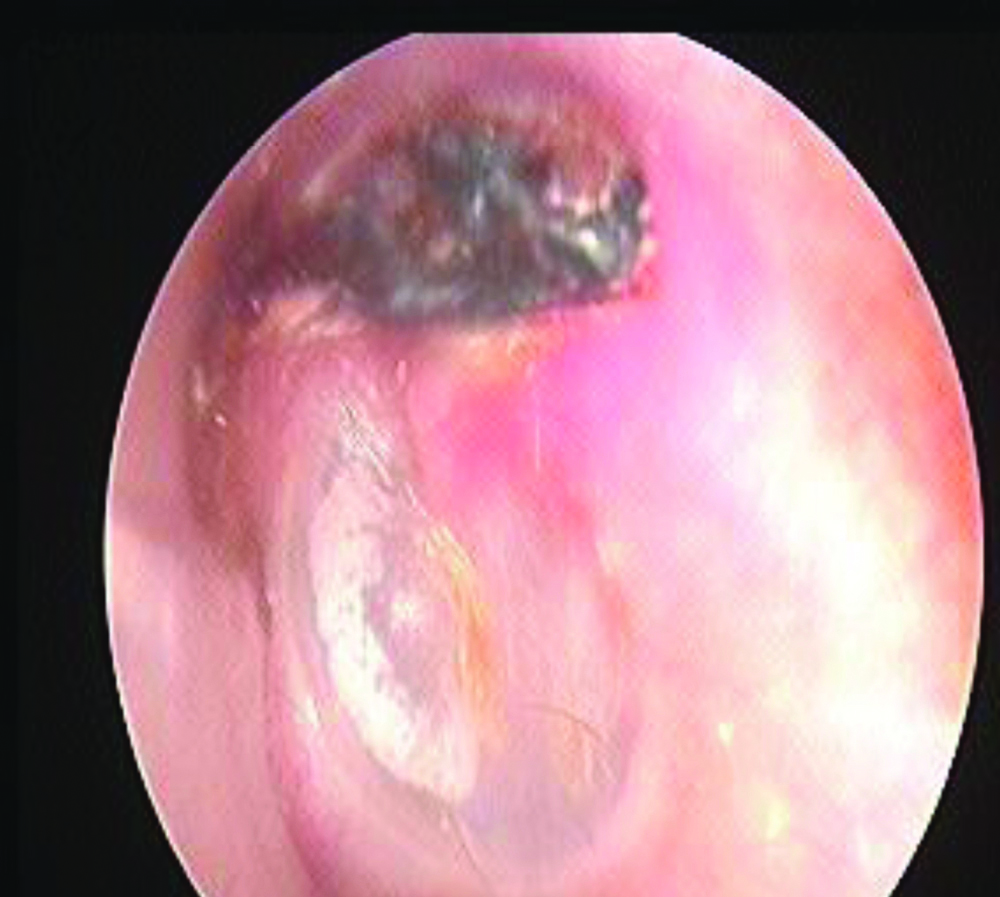
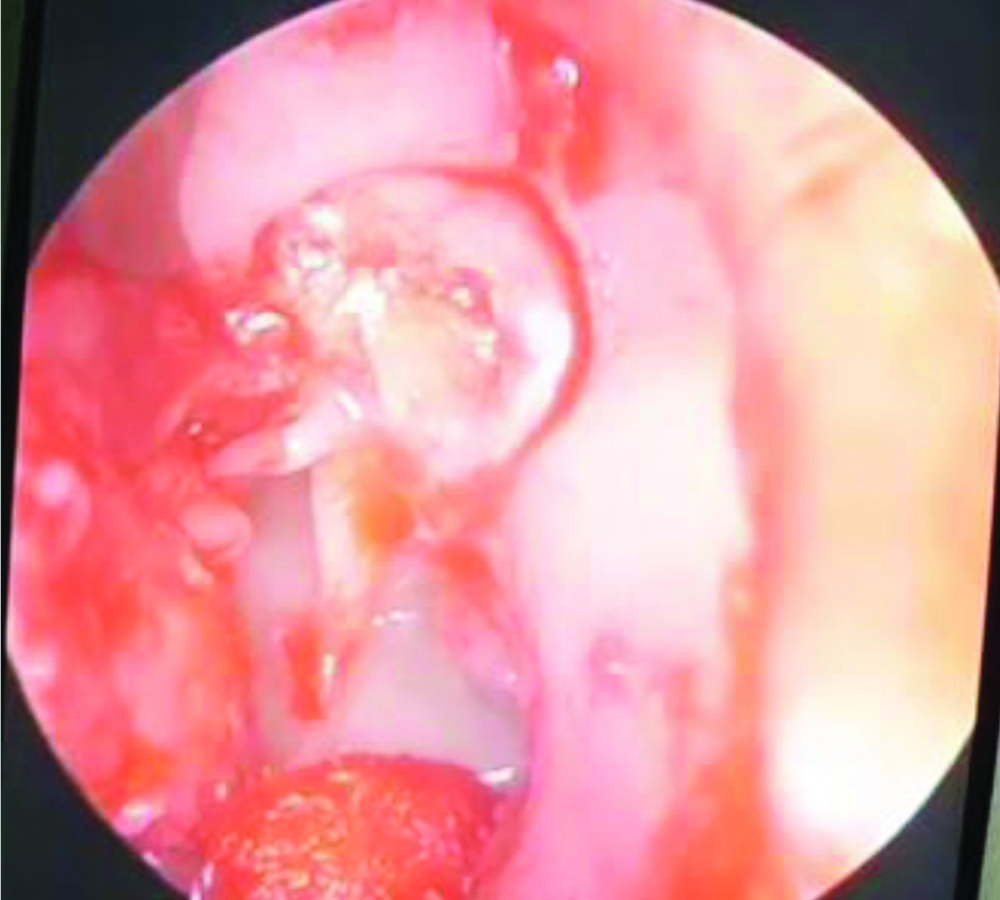
A 20-year-old female patient came with complaints of decreased hearing in left ear with occasional tinnitus. Patient also had history of left ear discharge, which was occasional and scanty. On otoscopic examination of left ear, impacted cerumen was seen in the attic region. Pars tensa showed mild retraction with tympanosclerotic patch in the anterosuperior and anteroinferior quadrant [Table/Fig-1]. On removal of wax with the aid of otoendoscopy, attic region was found to be filled with cholesteatoma debris.
Otoendoscopy-pars tensa showed mild retraction with tympanosclerotic patch in the anterosuperior and anteroinferior quadrant and impacted cerumen in the attic.
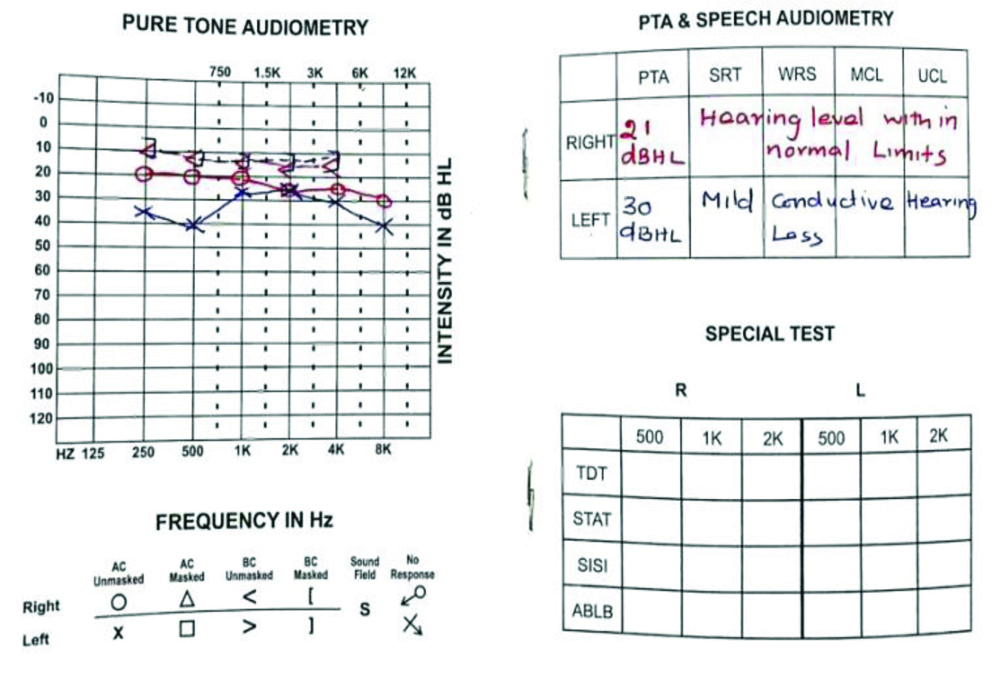
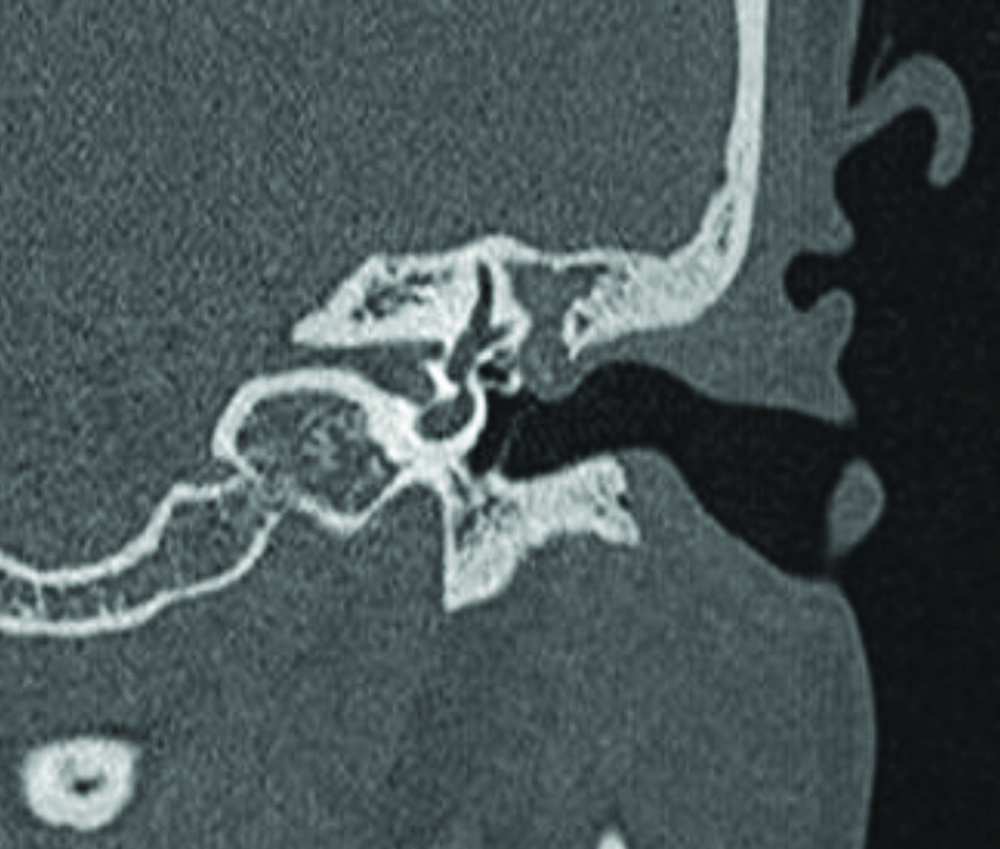
On pure tone audiometry, patient had mild conductive hearing loss of 30db [Table/Fig-2] and computed tomography of left temporal bone revealed ill-defined soft tissue density in the middle ear (epitympanum) with erosion of head of malleus and short process of incus. Blunting of scutum was also seen [Table/Fig-3].
Blunting of scutum in coronal section.
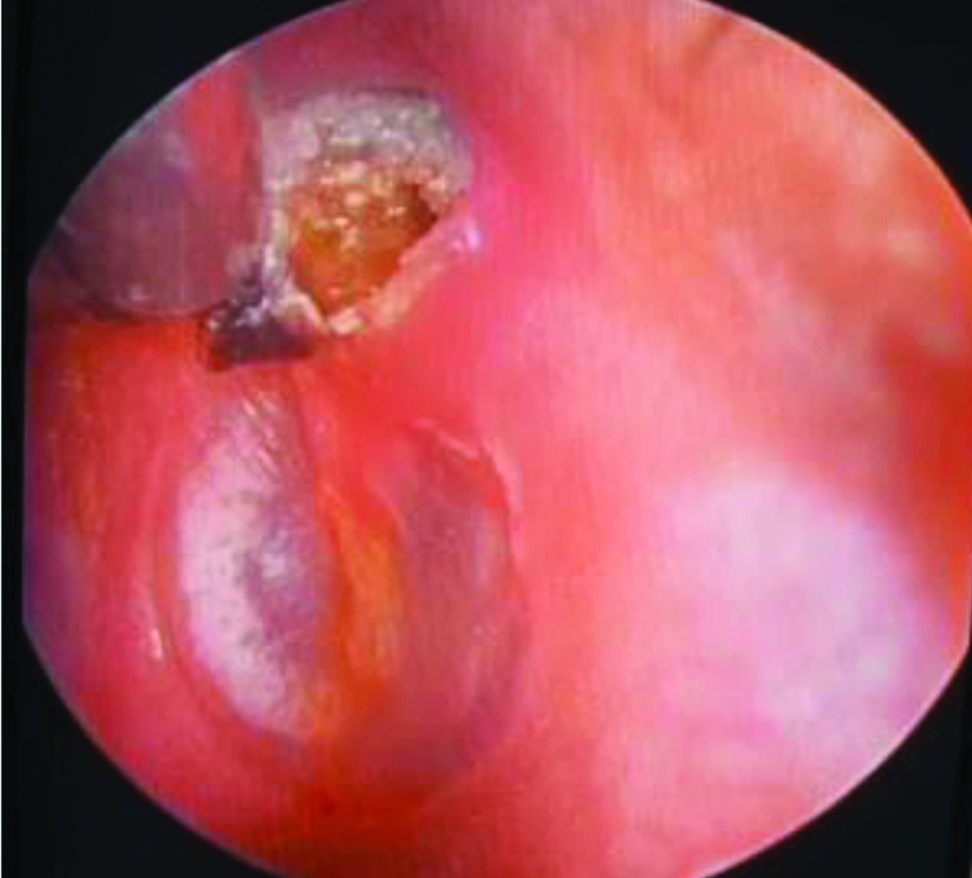
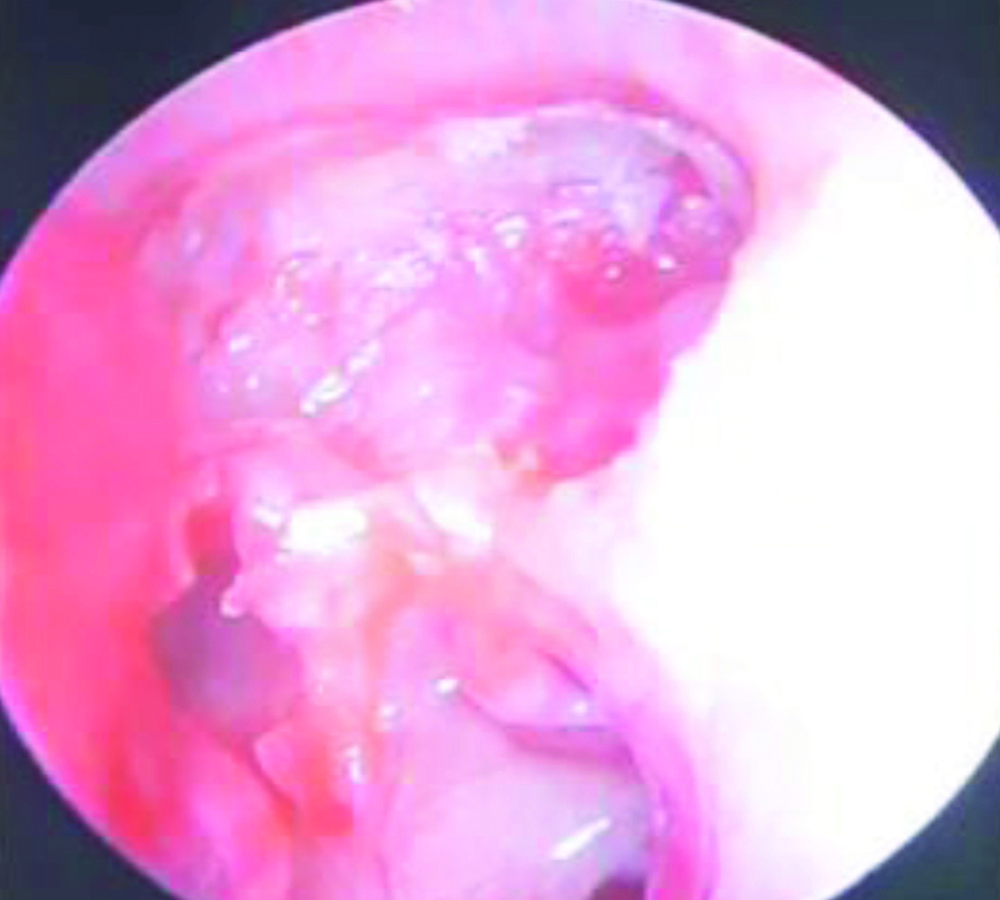
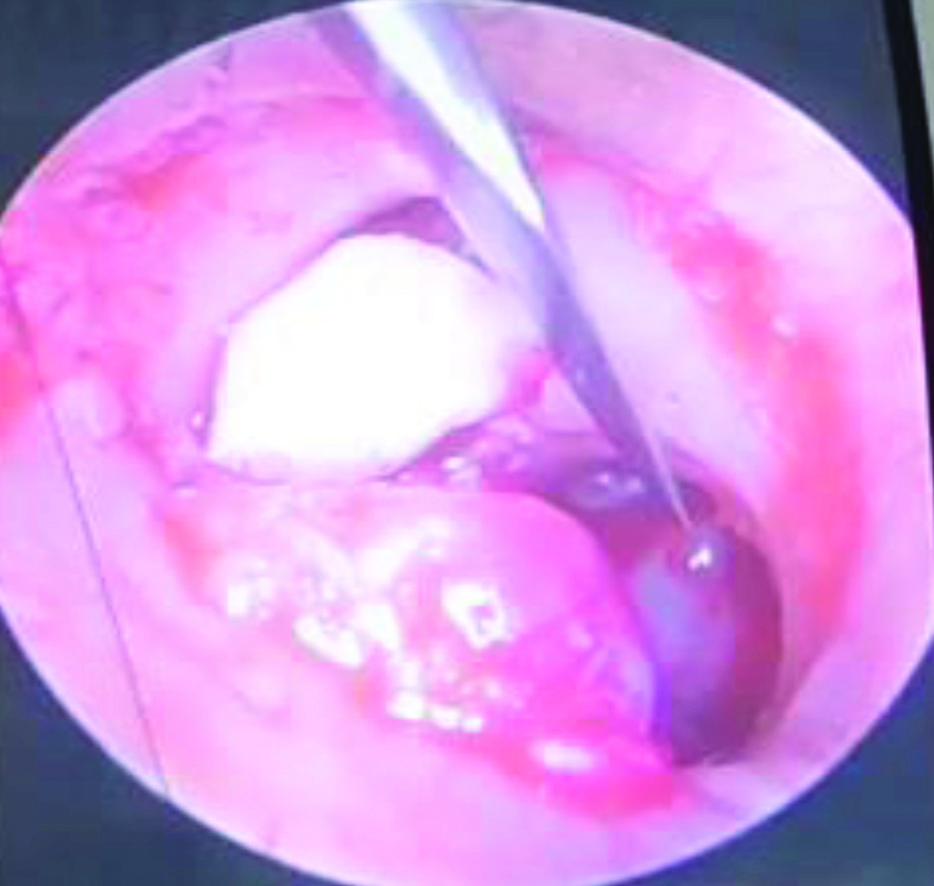
After doing necessary investigations, patient was taken for surgery under general anaesthesia, four quadrant infiltration was given in the external auditory canal, cholesteatoma debris was found to occupy the attic region with erosion of scutum [Table/Fig-4]. Rosen’s trans-canal incision was made and tympanomeatal flap was elevated from 2’o clock to 10’o clock position, handle of malleus was skeletonised and tympanomeatal flap was pushed anteriorly to expose the entire attic area [Table/Fig-5]. Posterior and superior attic wall was curetted out meticulously to delineate the cholesteatoma sac boundaries and the same was removed in toto [Table/Fig-6]. Head of malleus, body and short process of incus were eroded. Incudostapedial joint was disarticulated and remnant of incus was removed. Attic reconstruction was done using tragal cartilage [Table/Fig-7] and type III tympanoplasty was performed. Temporalis fascia graft was placed and tympanomeatal flap was repositioned.
Attic cholesteatoma and scutum erosion.
After elevation of tympanomeatal flap.
After removal of cholesteatoma debris.
Attic reconstruction with tragal cartilage.
On histopathological examination, the section showed keratin flakes with bacterial colonies which were consistent with cholesteatoma. On follow-up, patient had no further episodes of ear discharge. Neotympanum was healthy. Patient had improvement in hearing. Postoperative pure tone audiometric evaluation revealed 28 dBHL in left ear.
Discussion
Cholesteatoma is a cystic non-malignant lesion with well-demarcation which is derived from keratinised squamous epithelium which grows abnormally inside the temporal bone [1-3], often referred to as “skin in the wrong place” [4,5]. Cholesteatoma formation occurs due to proliferation of the matrix of cholesteatoma which results due to increased enzymatic activity. The annual incidence is 3 per 100,000 in children while it is 9.2 per 100,000 in adults [6]. Bony erosion is observed in majority of mature cholesteatomas. Initially, bony erosion is confined to the ossicular chain and scutum. As the cholesteatoma expands in size, it may lead to erosion of the otic capsule, fallopian canal and tegmen. The main goal when performing surgery for attic cholesteatoma is complete removal of cholesteatoma with prevention of residual or recurrent disease and restoration of hearing.
Cholesteatomas usually do not exist in an aggressive state. Often they remain undetected for years until dangerous presentations manifest [7]. Cholesteatomas often progress and remain undiscovered until they grow larger, invading intra-temporal structures. This can lead to various intracranial and extracranial complications [8].
Less invasive surgical measures can be implemented if cases were diagnosed early. This helps in preventing hearing loss, especially in children.
Early detection and prompt intervention (i.e., removal of cholesteatoma) are the cornerstones of successful treatment. A limited surgery performed on a small cholesteatoma sac with intact ossicular chain will result only in a small surgical defect with hearing preservation, so the end result will be more satisfactory than a canal wall down mastoidectomy. This is more helpful in young adults. Although there is better visualisation of the cholesteatoma in canal wall down mastoidectomy, it results in enlarged auditory meatus externally and shallow cavity in middle ear. Pertaining to these problems, postoperative patients usually require repeated and frequent follow-up postoperatively for a long term, water exposure should be avoided and fitting of hearing aids may be difficult in such cases. Atticotomy proves to be a better alternative to modified radical mastoidectomy since the above mentioned disadvantages of modified radical mastoidectomy are not seen in atticotomy because the size of external auditory canal is not disturbed [9].
Atticotomy is a surgical procedure in which the lateral wall of attic region (epitympanum) is removed. This technique helps to preserve the posterior canal wall and also gives ample visualisation of the middle ear structures and the attic compartment. It also provides better access to posterior and anterior epitympanum and undersurface of malleus and incus in extensive cholesteatomas spreading to these regions. Removal of these above mentioned structures results in better visualisation of operative field and prevents cholesteatoma recurrence. In cases of attic cholesteatomas when the disease is confined to the attic region, unwanted exenteration of the mastoid antrum can be avoided by this approach [9].
Cortical mastoidectomy was not performed in this patient since the sac was limited to the epitympanic region and also keeping in mind the preoperative aim of surgery to provide a dry and safe ear which requires minimal postoperative care for the benefit of the patient. Although, mastoidectomy is still preferred in some cases of cholesteatoma extending through the aditus into the antrum [10-12].
Conclusion(s)
Any case of impacted cerumen should not be ignored by otorhinolaryngologist. Further evaluation with thorough examination under otomicroscope/otoendoscope has to be done, which can lead to different diagnosis and treatment plan. Atticotomy is a useful surgical procedure for managing cholesteatomas limiting to the attic. It has been shown to have a low recurrence rate with less postoperative complications compared to canal wall down procedures.
Author Declaration:
Financial or Other Competing Interests: None
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 19, 2020
Manual Googling: Dec 21, 2020
iThenticate Software: Jan 15, 2021 (18%)
[1]. Isaacson G, Diagnosis of pediatric cholesteatomaPediatrics 2007 120(3):603-08.10.1542/peds.2007-012017766534 [Google Scholar] [CrossRef] [PubMed]
[2]. Semaan MT, Megerian CA, The pathophysiology of cholesteatomaOtolaryngologic Clinics of North America 2006 39(6):1143-59.10.1016/j.otc.2006.08.00317097438 [Google Scholar] [CrossRef] [PubMed]
[3]. Dornelles C, da Costa SS, Meurer L, Schweiger C, Some considerations about acquired adult and pediatric cholesteatomasBrazilian Journal of Otorhinolaryngology 2005 71(4):536-45.10.1016/S1808-8694(15)31212-X [Google Scholar] [CrossRef]
[4]. Robinson JM, Cholesteatoma: Skin in the wrong placeJournal of the Royal Society of Medicine 1997 90(2):93-96.10.1177/0141076897090002129068441 [Google Scholar] [CrossRef] [PubMed]
[5]. Gray JD, The chronic ear: The treatment of cholesteatoma in childrenProc R Soc Med 1964 57(9):769-71.10.1177/003591576405700903 [Google Scholar] [CrossRef]
[6]. Castle JT, Cholesteatoma pearls: Practical points and updateHead and Neck Pathology 2018 12(3):419-29.10.1007/s12105-018-0915-530069838 [Google Scholar] [CrossRef] [PubMed]
[7]. Shihada R, Brodsky A, Luntz M, Giant cholesteatoma of the temporal boneIsrael Medical Association Journal 2006 8:718-19. [Google Scholar]
[8]. Prasad SC, Shin SH, Russo A, Di Trapani G, Sanna M, Current trends in the management of the complications of chronic otitis media with cholesteatomaCurrent Opinion in Otolaryngology & Head and Neck Surgery 2013 21(5):446-54.10.1097/MOO.0b013e328364646723892792 [Google Scholar] [CrossRef] [PubMed]
[9]. Kim JH, Choi SH, Chung JW, Clinical results of atticoantrotomy with attic reconstruction or attic obliteration for patients with an attic cholesteatomaClinical and Experimental Otorhinolaryngology 2009 2(1):39-43.10.3342/ceo.2009.2.1.3919434290 [Google Scholar] [CrossRef] [PubMed]
[10]. Nyrop M, Bonding P, Extensive cholesteatoma: Long-term results of three surgical techniquesThe Journal of Laryngology & Otology 1997 111(6):521-26.10.1017/S002221510013782X9231084 [Google Scholar] [CrossRef] [PubMed]
[11]. Jennings BA, Prinsley P, Philpott C, Willis G, Bhutta MF, The genetics of cholesteatoma. A systematic review using narrative synthesisClinical Otolaryngology 2018 43(1):55-67.10.1111/coa.1290028485112 [Google Scholar] [CrossRef] [PubMed]
[12]. Vadiya S, Kedia A, Atticotomy, attic reconstruction, tympanoplasty with or without ossiculoplasty, canal plasty and cortical mastoidectomy as part of intact canal wall technique for attic cholesteatomaIndian Journal of Otolaryngology and Head & Neck Surgery 2015 67(2):128-31.10.1007/s12070-015-0821-z26075165 [Google Scholar] [CrossRef] [PubMed]