Pulmonary Adenofibroma in an Elderly Male with Recurrent Soft Tissue Sarcoma
Sandhya Devi Pasupathy1, Archana Lakshmanan2, S Annapurneswari3
1 DNB Resident, Department of Pathology, Apollo Hospitals, Chennai, Tamil Nadu, India.
2 Consultant, Department of Pathology, Apollo Hospitals, Chennai, Tamil Nadu, India.
3 Senior Consultant (HOD), Department of Pathology, Apollo Hospitals, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Sandhya devi Pasupathy, 35, Ahalya Apartments, Mambalam High Road, T. Nagar, Chennai, Tamil Nadu, India.
E-mail: psd_sandhya@hotmail.com
Pulmonary Adenofibroma (PAF) is a rare soft tissue tumour of the lung. It is a benign lesion, having a biphasic pattern with an admixture of epithelial and stromal components and has resemblance to fibroadenoma of the breast and adenofibroma of the female genital tract. The diagnosis can be challenging and it has to be delineated from other entities with biphasic pattern, like pulmonary hamartoma, pulmonary blastoma, intrapulmonary solitary fibrous tumour and metastases from soft tissue and visceral sarcomas, as each tumour has its own therapeutic and prognostic implications. Here, we report a case of a 73-year-old male, a known case of recurrent soft tissue sarcoma of the thigh, who presented with solitary pulmonary lesion. The patient was a non-smoker and did not have any specific respiratory complaints. On staging work-up with a Positron Emission Tomography and Computed Tomography (PET-CT), a hypermetabolic lesion was identified in the anterior segment of right upper lobe of the lung, following which he underwent right lobectomy. The tumour was a solitary lesion located near the hilum and on histology showed a biphasic pattern with scattered glandular spaces lined by columnar epithelium set in a hyalinised spindle cell stroma. The cells showed mild pleomorphism with oval to elongated nuclei and indistinct cytoplasm. On immunohistochemistry, the epithelial component showed positivity for Cytokeratin (CK), Epithelial Membrane Antigen (EMA), Thyroid Transcription Factor-1 (TTF-1) and Napsin-A and the stromal component showed positivity for Vimentin, Desmin, Smooth Muscle Actin (SMA) and H-Caldesmon (High molecular weight isoform-Caldesmon). With the given histological and immunohistochemistry findings, a diagnosis of PAF was rendered.
Biphasic, Lung, Metastases, Sarcoma
Case Report
A 73-year-old male patient reported to the Department of Pathology. Patient had a history of recurrent high grade soft tissue sarcoma in the right thigh, which was diagnosed and treated with repeated wide excision and was on regular follow-up since past 10 years. He was non-smoker. The patient was evaluated with a follow-up PET-CT which showed a hypermetabolic lesion in the anterior segment of right upper lobe of the lung with no other identifiable lesions. The patient had no respiratory symptoms and no other associated co-morbidities. The provisional diagnosis was metastasis from the soft tissue sarcoma of the thigh. Since the patient had good performance status with what appeared to be a solitary lesion with non-specific symptoms, he was taken-up for right lobectomy. The postoperative period was uneventful.
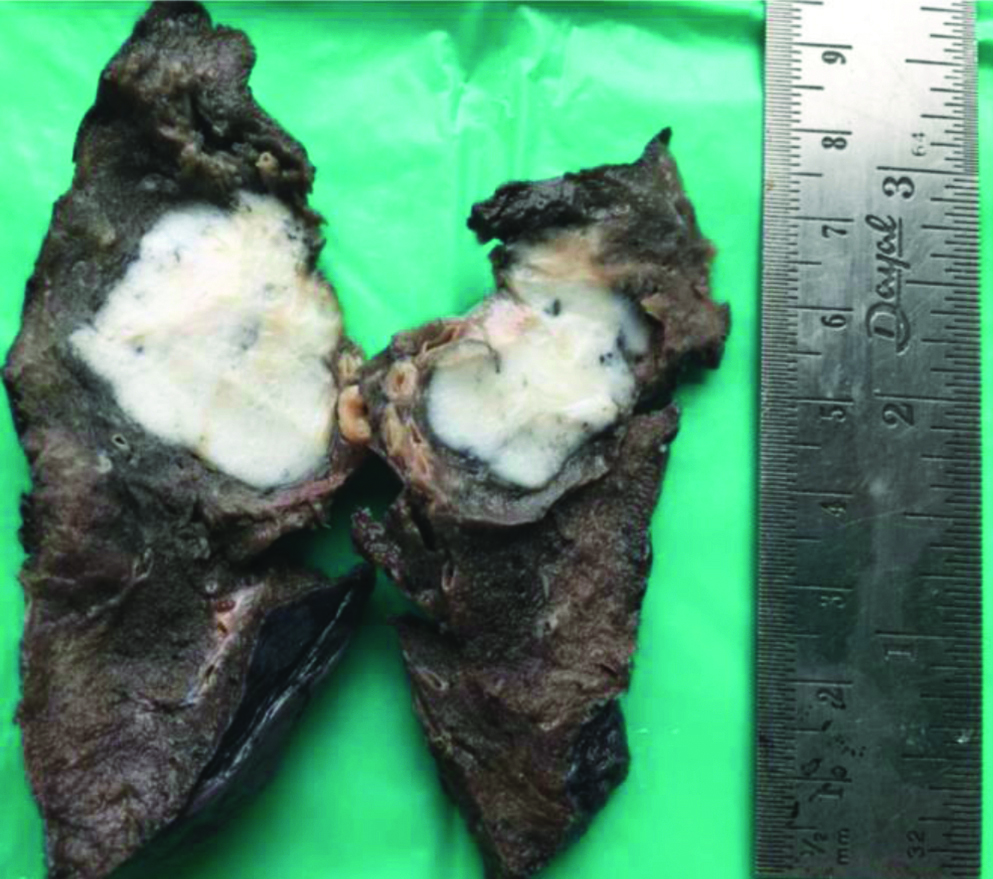
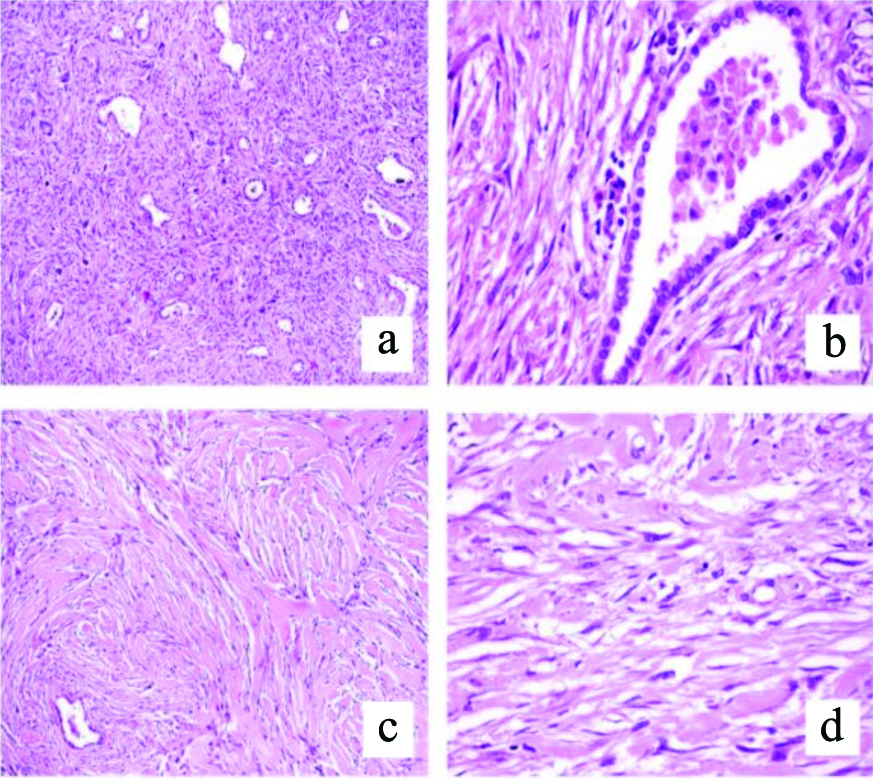
Macroscopically, a greyish-white, fleshy, fairly circumscribed lesion was identified near the hilum and measured 3.5×2.5×2 cm [Table/Fig-1]. Histological examination showed an un-encapsulated lesion with biphasic pattern with both the components closely intermingled with each other. One component was composed of spindle cells with extensive areas of stromal hyalinisation with dense collagen. The cells had elongated spindly nuclei and indistinct cytoplasm. Amidst these were tubular glands of varying sizes lined by cuboidal to columnar cells. There was no significant cellular atypia in both the glands as well as the stroma. Mitotic figures were hard to find. There was no necrosis or haemorrhage. No other mesenchymal components like fat, muscle or adipose tissue were identified. Histopathological findings were as depicted in [Table/Fig-2]. The differentials considered were metastatic sarcoma, Solitary Fibrous Tumour (SFT) with entrapped bronchioles, pulmonary hamartoma and PAF.
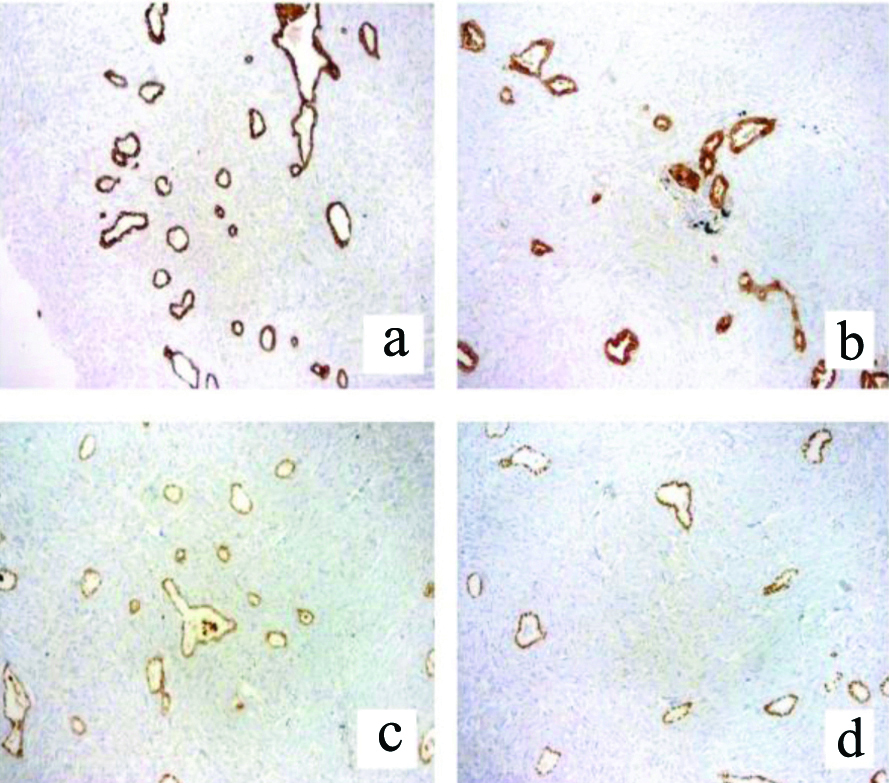
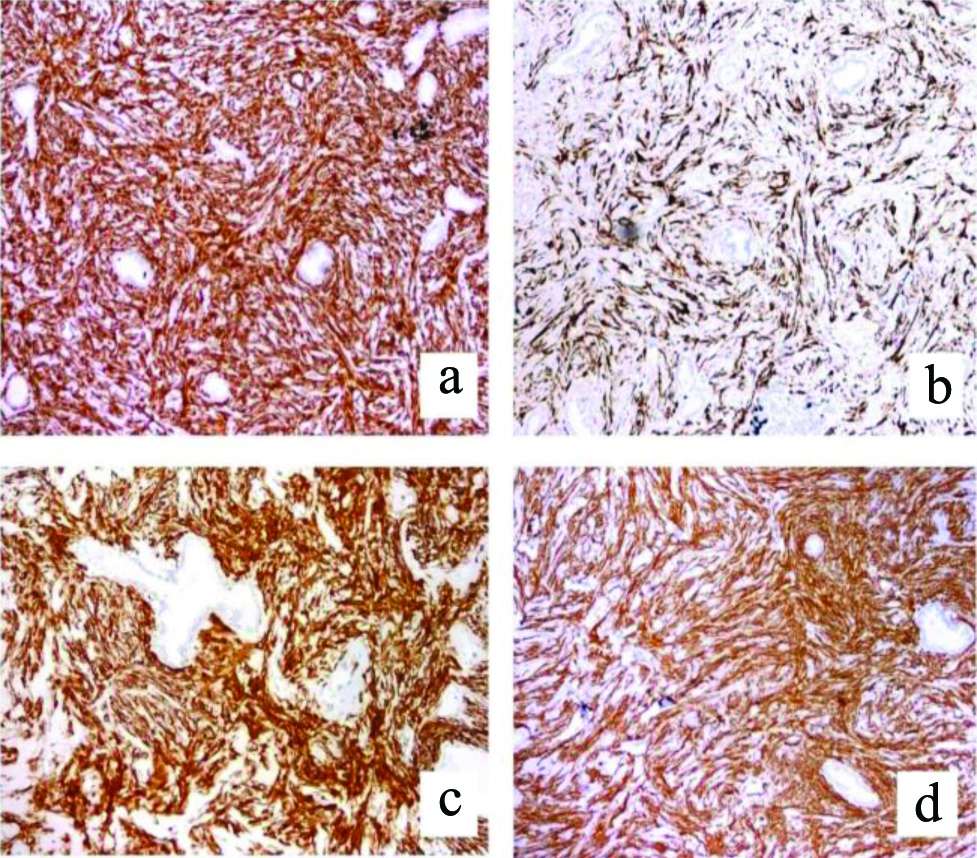
Immunohistochemical analysis demonstrated positivity for CK, EMA, TTF-1 and Napsin-A in glands [Table/Fig-3]. Vimentin, desmin, SMA, H-Caldesmon and CD10 were positive in spindle cell areas [Table/Fig-4]. The glandular and stromal cells were both negative for CD34, S-100, Signal Transducer and Activator of Transcription 6 (STAT-6), oestrogen Receptor (ER), Progestrone Receptor (PR) and B-Cell Lymphoma 2 (BCL-2). Thus, a final diagnosis of PAF was rendered. Patient is doing well without any evidence of disease recurrence at one year of follow-up.
A greyish-white fleshy lesion located in the right upper lobe of lung close to the hilum.
a: (H&E-100X); b: (H&E-400X): Tubular glands of varying sizes lined by single layer of cuboidal cells without atypia; c: (H&E-100X); d: (H&E-400X): Background shows spindly cells with extensive stromal hyalinisation and dense collagen.
Glandular component is positive for CK (a-100X), EMA (b-100X), Napsin-A (c-100X) and TTF-1 (d-100X).
CK: Creatine kinase; EMA: Ephithelial membrane antigen; TTF-1: Thyroid transcription factor 1
Stromal cells are positive for vimentin (a-100X), desmin (b-100X), SMA (c-100X) and H-Caldesmon (d-100X).
SMA: Smooth muscle actine
Discussion
The PAF is an uncommon entity which was first described by Scarff RW and Gowar FJ in 1944 [1]. It is more common in adults, mostly in the 5th and 6th decade with male preponderance [2,3]. In present case, the patient was an elderly male with no specific respiratory symptoms. It is a rare lesion with most patients being asymptomatic and others present with non-specific respiratory symptoms. Few authors consider the tumour to be neoplastic and few as hamartomatous in nature [1,3-5]. Other experts stated that the tumour originates from peri-bronchial connective tissue and from the pulmonary epithelium [6,7]. Hence, the histologic nature of this disease remains ambiguous.
The lesion is usually detected as an incidental finding on radiological examination and presents mostly as a solitary pulmonary nodule [4]. Very rarely, they can present as multiple masses as reported by Hao J et al., and Kim M et al., [8,9]. Histologically, PAF shows close admixture of stromal and epithelial components. The stromal component shows spindle cells with elongated nuclei and indistinct cytoplasm with stromal hyalinisation. The tubular glands noted show cuboidal to columnar lining. Diagnosis can be very challenging and this lesion needs to be distinguished from both benign and malignant pulmonary mimics with biphasic patterns because of therapeutic implications. It is usually hard to diagnose these lesions on routine fine needle aspiration cytology, core needle biopsies and on frozen sections [4].
The differentials include pulmonary hamartoma, pulmonary blastoma, solitary fibrous tumour, low grade sarcoma and metastases [4]. Given the history of recurrent sarcoma in the present case, the main differential considered was metastatic sarcoma. As this lung lesion was solitary with absence of atypia or mitotic activity, a possibility of metastasis was excluded. On morphology, pulmonary hamartomas appear as a solitary lesion, composed of variable mixture of mature hyaline cartilage, fibrous tissue, smooth muscle, fat, sometimes with calcification/ossification and entrapped clefts lined by respiratory epithelium. Pulmonary blastomas are aggressive lesions with a biphasic component with admixed epithelium and primitive stroma showing atypia with or without heterologous differentiation. Solitary Fibrous Tumour (SFT) is a main differential diagnosis, as some authors consider PAF to be a variant of SFT. Although many studies emphasise the importance of STAT6 in delineating the two entities [10,11]. Fusco N et al., found that recurrent NAB2-STAT6 fusions were noted in PAF along with Estrogen Receptor (ER) expression [12]. Few authors have even reported an adenomatous or papillary variant of SFT, which is very similar to PAF [13,14]. Olson NJ et al., reported synchronous PAF with SFT in the same patient [15]. It is difficult to draw a conclusion, whether these entities represent spectrum of same tumour or two different entities based on these few case studies. Future larger studies may help in deriving a clear picture, due to the clinical relevance. Immunohistochemistry findings helped in present case in excluding other mimics and arriving at the correct diagnosis.
The diagnostic efficacy with the help of cytology and core biopsy for PAF is stunted and there are chances where it can be misinterpreted as a malignant lesion [5]. Hence, resection of the lesion with minimally invasive procedure would be a better option. Intraoperative frozen section can also serve as a better option for management in these patients. In present case, frozen section was not carried out. Wang Y et al., concluded that video-assisted thoracoscopic surgery is the most appropriate mode of management of lung lesions located peripherally and for few centrally located pulmonary lesions [16].
Similar to present case report, Corzani R et al., reported a case of PAF during a staging work-up of a testicular tumour in a 24 year male, which they initially thought to be a metastatic lesion [17]. According to the articles reviewed, most of the PAFs ran a benign course with no potential for metastasis.
Conclusion(s)
Pulmonary adenofibroma is a benign lesion of the lung with cryptic histogenesis, possessing a biphasic pattern composed of glandular and stromal elements. It is often detected as a pulmonary nodule with no distinguishing clinical or radiological features and the diagnosis in present case was a histological surprise. Hence, it is important for pathologists to recognise this entity and demarcate it from other pulmonary mimics to aid in the appropriate management.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? NA
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 03, 2020
Manual Googling: Dec 29, 2020
iThenticate Software: Jan 19, 2021 (8%)
[1]. Scarff RW, Gowar FJS, Fibroadenoma of the lungJ Pathol Bacteriol 1944 56(2):257-59. [Google Scholar]
[2]. Esmaeili H, Azimpouran M, Shokohi B, Mostafidi E, Karbasi M, Pulmonary adenofibroma; A rare findingAm J Med Case Rep 2016 4(3):101-07. [Google Scholar]
[3]. Kumar R, Desai S, Pai T, Pramesh CS, Jambhekar NA, Pulmonary adenofibroma: Clinicopathological study of 3 cases of a rare benign lung lesion and review of the literatureAnn Diagn Pathol 2014 18(4):238-43.10.1016/j.anndiagpath.2014.04.00224908371 [Google Scholar] [CrossRef] [PubMed]
[4]. Vitkovski T, Zeltsman D, Esposito M, Morgenstern N, Pulmonary adenofibroma: Cytologic and clinicopathologic features of a rare benign primary lung lesionDiagn Cytopathol 2013 41(11):991-96.10.1002/dc.2287422645035 [Google Scholar] [CrossRef] [PubMed]
[5]. Suster S, Moran C, Pulmonary adenofibroma: Report of two cases of an unusual type of hamartomatous lesion of the lungHistopathology 1993 23(6):547-51.10.1111/j.1365-2559.1993.tb01241.x8314238 [Google Scholar] [CrossRef] [PubMed]
[6]. Bateson EM, Histogenesis of intrapulmonary and endobronchial hamartomas and chondromas (cartilage-containing tumours): A hypothesisJ Pathol 1970 101(2):77-83.10.1002/path.17110102025475528 [Google Scholar] [CrossRef] [PubMed]
[7]. Perez-Ataide AR, Seiler MW, Pulmonary hamartoma. An ultra-structural studyCancer 1984 53(3):485-92.10.1002/1097-0142(19840201)53:3<485::AID-CNCR2820530319>3.0.CO;2-S [Google Scholar] [CrossRef]
[8]. Hao J, Zhang C, Cao Q, Zou J, Wang C, Pulmonary adenofibroma: Report of a case with multiple massesAnn Clin Lab Sci 2016 46(6):691-95. [Google Scholar]
[9]. Kim M, Bae YA, Byeon SJ, Choi JA, Pulmonary adenofibroma manifesting as two nodules in different lobes of the lung: A case reportJ Korean Soc Radiol 2020 81(2):436-41.10.3348/jksr.2020.81.2.436 [Google Scholar] [CrossRef]
[10]. Demicco EG, Harms PW, Patel RM, Smith SC, Ingram D, Torres K, Extensive survey of STAT6 expression in a large series of mesenchymal tumoursAm J Clin Pathol 2015 143(5):672-82.10.1309/AJCPN25NJTOUNPNF25873501 [Google Scholar] [CrossRef] [PubMed]
[11]. Lindholm KE, Sansano Valero I, Rodriguez JL, Cajal SR, Moran CA, Pulmonary adenofibromas: A clinicopathologic correlation of 13 casesAm J Surg Pathol 2020 44(7):917-21.10.1097/PAS.000000000000145632091433 [Google Scholar] [CrossRef] [PubMed]
[12]. Fusco N, Guerini-Rocco E, Augello C, Terrasi A, Ercoli G, Fumagalli C, Recurrent NAB2-STAT6 gene fusions and oestrogen receptor-alpha expression in pulmonary adenofibromasHistpathology 2017 70(6):906-17.10.1111/his.1316528072477 [Google Scholar] [CrossRef] [PubMed]
[13]. Cavazza A, Rossi G, De Marco L, Putrino I, Pellegrino S, Piana S, Solitary fibrous pseudopapillary tumour of the lung: Pulmonary fibroadenoma and adenofibroma revisitedPathologica 2003 95(3):162-66. [Google Scholar]
[14]. Sironi M, Rho B, Spinelli M, Adenofibromatous pattern in a solitary fibrous tumour of the lungInt J Surg Pathol 2005 13(1):7910.1177/10668969050130011115735859 [Google Scholar] [CrossRef] [PubMed]
[15]. Oslon NJ, Czum JM, de Abreu FB, Linos K, Black CC, Synchronous pulmonary adenofibroma and solitary fibrous tumour: Case Report and review of literatureInt J Surg Pathol 2019 27(3):322-27.10.1177/1066896918807302 [Google Scholar] [CrossRef]
[16]. Wang Y, Xiao HL, Jia Y, Chen JH, He Y, Tan QY, Pulmonary adenofibroma in a middle-aged man: Report of a caseSurg Today 2013 43(6):690-93.10.1007/s00595-012-0341-323139047 [Google Scholar] [CrossRef] [PubMed]
[17]. Corzanni R, Bellan C, Luzzi L, Ghisalberti M, Ligabue T, Meniconi F, A rare pulmonary adenofibroma mimicking a metastatic lesionClin Surg 2017 2(1-3):1691 [Google Scholar]