Introduction
Asthma control is the extent of observed asthma symptoms in patients and reduction in symptoms after treatment. Simple screening tools are available to assess asthma control. Asthma control test is a simple numerical scoring system that can be easily used on a routine basis. Latest Global Initiative for Asthma (GINA) guidelines stress that asthma control is the main objective of asthma treatment. In this COVID-19 pandemic situation, there is an hesitancy in performing and undergoing pulmonary function tests among physicians and the patients. Hence, in this study it was planned to correlate the asthma control test values with FEV1 and other parameters like Peak Expiratory Flow Rate (PEFR), Absolute Eosinophil Count (AEC) and serum magnesium.
Aim
To study the correlation between asthma control test and FEV1; to study the correlation between asthma control test and other parameters like PEFR, AEC and Serum magnesium.
Materials and Methods
This was a cross-sectional observational study done from February 2019 to January 2020 conducted at Department of Pulmonary Medicine. A total of 55 patients of Bronchial asthma in line with GINA Guidelines were included in the study. Asthma control test questionnaire was administered to all the patients. Routine blood investigations like Total Leucocyte Count (TLC), Differential Leucocyte Count (DLC), Absolute Eosinophil Count (AEC), serum magnesium levels were done. Pulmonary function parameters like FEV1 and PEFR were measured.
Results
Asthma control test had positive correlation with FEV1 with a spearman’s correlation of 0.2758 and p-value of 0.0414 which was statistically significant. The spearman’s correlation between asthma control test and AEC was -0.4583 with a p-value of <0.001, which was significant. The correlation of asthma control test with serum magnesium was 0.3414 with a p-value of 0.010.
Conclusion
Asthma control test score had a significant positive correlation with FEV1 and serum magnesium levels. It also had significant negative correlation with AEC (inflammatory marker). Hence, asthma control test can be used as tool for treatment response in the current COVID-19 pandemic situation and also in resource limited settings.
Introduction
Bronchial asthma is one of the most common chronic airway diseases characterised by hyper responsiveness of airways and reversibility in bronchoconstriction after nebulisation with bronchodilator. Bronchial asthma affects 1-18% of population in different countries [1].
Asthma control is the extent of observed asthma symptoms in patients and reduction in symptoms after treatment. Asthma control have two domains i.e., symptom control and future risk of exacerbations. Simple screening tools are available to assess asthma control. Various tools available are GINA symptom control tool, primary care asthma control tool. There are a few numerical asthma control tools which scores and cuts points to distinguish different symptoms and severity of asthma [1].
Asthma severity is assessed retrospectively based on the level of treatment required for symptom control and prevention of exacerbations. Mild asthma is asthma that is well controlled with step 1 and step 2 of treatment, moderate asthma is asthma controlled with step 3 of treatment and severe asthma is asthma controlled by step 4 and step 5 of treatment [1,2].
Poor asthma control leads to substantial effect on quality of life and economic burden. Various host factors and environmental factors are responsible for development and control of bronchial asthma. Host factors are genetics, obesity, sex and preterm or with small size for gestational age. Environmental factors are allergens, infections, microbiome, occupational sensitizers, microbiome, diet, stress and smoking [1,3].
Numerical asthma control tools available are asthma control questionnaire and asthma control test. Asthma control questionnaire score ranges from 0-6, higher the value, worse is the asthma control. Asthma control test scores range from 5-25, higher the value, better is the asthma control [1].
ACTs have good accuracy for screening control of asthma. An ACT score of 19 or less suggests patients might be experiencing control problems. This score detected severe asthma with specificity (71%) and sensitivity (71%). A score of 19 or less might obviate the need for further evaluation of the patient to determine measures required to improve asthma control. The data from different studies suggests that a score of 16 or less is of concern because it predicts poor control of asthma [2].
Schatz M et al., performed a study on reliability of asthma control test which showed it was reliable and valid in asthma control assessment for patients under the care of asthma specialists. Study also provided evidence that ACT scores change overtime with asthma treatment. Study also observed that ACT correlates poorly with FEV1 which is consistent with the previous studies that concluded asthma control cannot be inferred from single measure of lung function [2].
Lung function should be assessed at diagnosis and three to six months of controlled treatment and periodically thereafter. Studies have shown that FEV1 does not strongly correlate with asthma symptoms in adults and children. PEFR is used as a monitoring tool in asthmatics to predict exacerbation and decline in lung function but the correlation of PEFR with asthma control test has not been studied [4]. Eosinophils have been viewed as the primary effector cell in asthma since their discovery [5]. Various studies have noted that levels of eosinophils in blood is related to disease severity in asthma patients [6,7].
Magnesium is the fourth most common cation in the body. Magnesium has many functions in the body. It competes with calcium influx in the smooth muscles and prevents muscular contraction, stabilises the mast cells, also influences cholinergic transmission and stimulates synthesis of nitric oxide. Both intravenous and nebulised magnesium sulphate are shown to be useful in management of bronchial asthma and the prevalence of hypomagnesemia in bronchial asthma cases is well documented [8].
Many cross-sectional studies have concluded that higher intake of dietary magnesium is associated with decreased airway responsiveness and symptoms in adults. Magnesium has bronchodilator property and this has led to its use for acute asthma exacerbation in emergency department [9].
Asthma control test is a simple numerical scoring system that can be easily used on a routine basis. Latest GINA guidelines stress that asthma control is the main objective of asthma treatment. The objective measures of asthma control include pulmonary function tests measuring FEV1, PEFR. The association of AEC and serum magnesium in asthma control has also been studied. But however, literature on correlation of lung function parameters and serum magnesium levels with Asthma control test is limited [1].
In this COVID-19 pandemic situation there is hesitancy in performing and undergoing pulmonary function tests among physicians and the patients. Hence, this study was planned to correlate the asthma control test values with FEV1 and PEFR as the primary objective and to correlate the asthma control test with AEC, serum magnesium as secondary objective.
Materials and Methods
Study design: A cross-sectional observational study was conducted at Department of Pulmonary Medicine, from February 2019 to January 2020. Ethical clearance was taken from the institutional ethics committee and the ethical clearance number was 1611/IEC/2019. All procedures followed were in accordance with the ethical standards of the committee on human experimentation. Informed consent was obtained from all patients for being included in the study.
Patients of Bronchial Asthma in line with GINA Guidelines were included in the study. Sample size=55 {n=(z1-α/2)2(p)(q)/(d)2} p=Prevalence of asthma in India 3.7% [10].
Each patient was explained in detail about the study and was asked to sign a written informed consent document before enrolment and before any study procedures is performed.
Inclusion criteria: Age more than 18 years, patients diagnosed with asthma according to the current GINA guidelines, mild to moderate asthmatics.
Exclusion criteria: Pregnancy, patients on diuretic therapy, cardiac disease, chronic kidney disease, life threatening asthma, chronic persistent severe asthma.
Asthma Control Test
Asthma control test is a simple numerical tool to assess asthma control which has various parameters like symptom control, frequency of night symptoms, use of controller medications, disturbance from work. It has a total of five questions with a score of 0-5, 0 being the least score and 5 being the highest score in each question. Asthma control test is divided into three categories: well controlled if it 20-25, not well controlled if it is 16-19 and very poorly controlled asthma if less than 15.
A detailed clinical history was taken and a thorough physical examination was done on all the patients included in study. Asthma control test questionnaire was administered to all the patients. Routine blood investigations like TLC, DLC, AEC, serum magnesium levels were done. Pulmonary function parameters like FEV1 and PEFR were measured.
Statistical Analysis
Descriptive analysis was done in Microsoft excel software. Statistical tests used for standard deviation and spearman’s rank correlation and p-value was calculated to know the significance of correlation.
Results
A total of 55 diagnosed asthma patients were included in the study. The mean age of patients in the study population was 39.9±14.9. A total of 27 females and 28 males were present in the study.
Asthma control test: The mean ACT score was 15.6±4.01. Eight patients had well controlled asthma, 21 patients had partially controlled asthma and 26 patients had uncontrolled asthma [Table/Fig-1].
Distribution of patients in the three groups of asthma control.
| ACT score | Number of patients |
|---|
| 0-15 (very poorly controlled asthma) | 26 (47%) |
| 16-19 (not well controlled) | 21 (38%) |
| >20 (well controlled) | 8 (14%) |
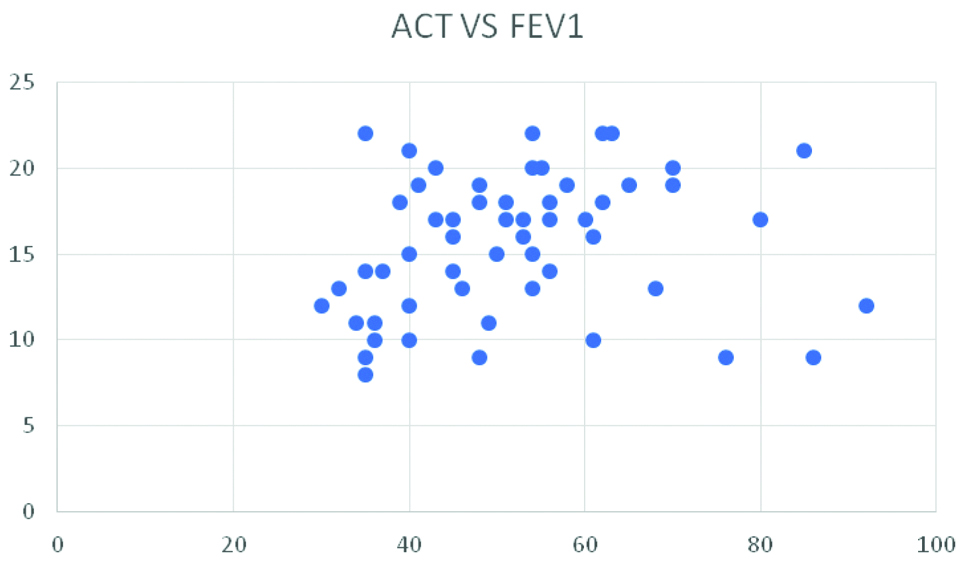
FEV1 and its correlation with ACT: The mean percentage predicted of FEV1 was 52.01±14.47. The FEV1 of three patients was more than 80% which was normal. 47% of the patients had FEV1 between 30% to 50% and 45% patients had FEV1 between 50% to 80% [Table/Fig-2]. The spearman’s correlation between asthma control test and FEV1 was 0.2758 with a p-value of 0.0414 which was statistically significant [Table/Fig-3]. Correlation of ACT with study parameters [Table/Fig-4].
Distribution of patients in FEV1 groups.
| FEV1 | Number of patients |
|---|
| <30% | 1 |
| 30-50% | 26 |
| 50-80% | 25 |
| >80% | 3 |
Scatter plot of correlation between ACT and FEV1.
ACT: Y axis FEV1: X axis
| Parameter | Mean±SD | Correlation with ACT | p-value |
|---|
| FEV1 | 52.01±14.47 | 0.2758 | 0.0414 |
| PEFR | 234.54±83.26 | 0.2575 | 0.05 |
| AEC | 456.34±266.9 | -0.4583 | <0.001 |
| Serum magnesium | 1.99±0.21 | 0.3414 | 0.010 |
Peak Expiratory Flow Rate (PEFR) and its correlation with ACT: The mean was PEFR 234.54±83.26 [Table/Fig-5]. The correlation between asthma control test and PEFR was 0.2575 with a p-value of 0.05 which was not statistically significant.
Distribution of PEFR among patients.
| PEFR | Number of patients(n=55) |
|---|
| <200 L/MIN | 28 |
| 200-400 L/MIN | 25 |
| >400 L/MIN | 2 |
Absolute Eosinophil Count (AEC) and its correlation with ACT: The mean AEC was 456.34 cells μL with a standard deviation of 266.9. A majority of patients had AEC between 251-500 cells μL, 47% (26 patients) [Table/Fig-6]. The spearman correlation between Asthma control test and AEC was -0.4583 with a p-value of <0.001, which was statistically significant.
Levels of peripheral eosinophils in the study population.
| AEC cells μL | Number of patients (n=55) |
|---|
| 100-250 | 12 |
| 251-500 | 26 |
| 501-750 | 8 |
| >750 | 9 |
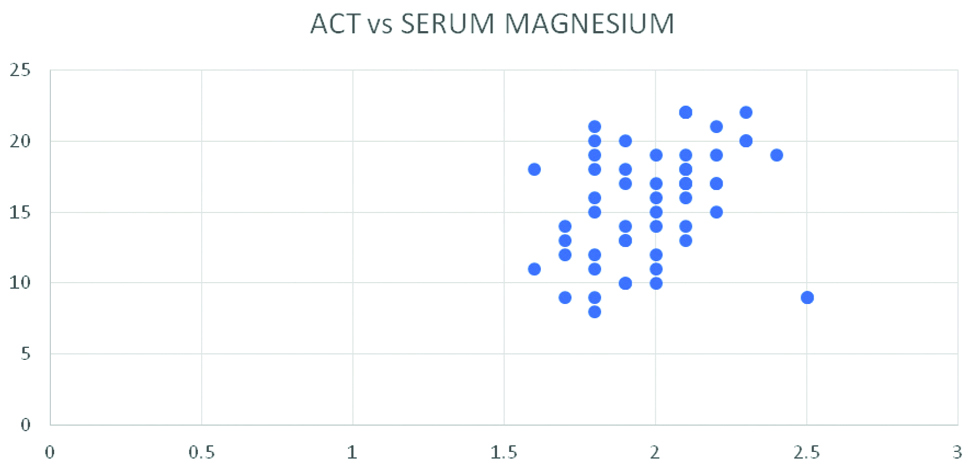
Correlation of ACT and levels of serum magnesium: The mean serum magnesium was 1.99±0.21. The spearman correlation of asthma control test with serum magnesium was 0.3414 with a p-value of 0.010, which was statistically significant [Table/Fig-7].
Scatter plot of ACT and Serum magnesium levels.
ACT: Y axis Serum magnesium: X axis
Discussion
Pulmonary function tests and asthma control test: In present study, Asthma control test and FEV1 had a positive correlation with a p-value of 0.0414 which is statistically significant.
Obianulu O et al., studied the correlation between ACT and prebronchodilator FEV1 in Nigerian with bronchial asthma. They included 46 asthmatics and found that ACT has a positive correlation with FEV1 similar to present result [11]. Papokosta D et al., studied the relationship of ACT with FEV1 and exhaled nitric oxide (FeNO) in 160 asthmatics. They found that ACT had a positive correlation with prebronchodilator predicted FEV1 % (r=0.177, p=0.25) and negative correlation with FeNO (r=-0.211, p=0.007). They concluded that ACT score was found to reflect lung function and inflammation in Greek asthmatic population [12].
Asthma control and PEFR: No studies were reported on asthma control and PEFR in adults. In present study, ACT and PEFR did not have a significant positive correlation (Spearman’s correlation-0.2575, p-value 0.05). In a study performed by Chan M et al., comparing asthma control test and PEFR showed no correlation in paediatric population [13].
Asthma control test and serum magnesium levels: Daliparty VM et al., conducted a cross-sectional study on the effect of serum magnesium levels on asthma control in 160 patients. They concluded that serum magnesium levels are correlated positively with asthma symptom control. It can be inferred from this study that serum magnesium levels might be used as a biomarker in assessing control or severity of asthma [14].
Kılıc H et al., did a case control study with 50 patients and 40 controls in which the relationship between serum magnesium values and lung function parameters were studied. It was found that lung functions were significantly lower in patients with hypomagnesemia [8]. From these studies it can be inferred that serum magnesium levels are associated with asthma control.
In present study, asthma control test had a significant positive correlation with serum magnesium levels. None of the patients in present study had hypomagnesemia, the mean levels of serum magnesium was 1.99 mg/dL. It has to be noted at this point that serum magnesium levels are not true indicators of magnesium levels in body.
A magnesium concentration of less than 1.6 mg/dL suggests hypomagnesemia, however it does not lead to manifestation of symptoms and signs, until it is less than 1.2 mg/dL in the serum. Measurement of the serum magnesium level however might not imply accurately the levels of intracellular magnesium. Intracellular depletion of magnesium may be seen despite a normal serum concentration. Estimation of magnesium concentration within the cells is not usually done because of the difficulty in performing tissue and cellular assays [15].
Asthma control test and Absolute Eosinophil Count (AEC): Casciano J et al., conducted a study to determine whether healthcare resources use and expenditure vary by eosinophil levels among patients with asthma. They included 2164 patients and found that patients with elevated eosinophil levels had significantly greater mean annual hospital admissions. From this study it can be concluded that higher eosinophil count is associated with poor asthma control [16].
In present study, asthma control test had significant negative correlation with AEC. Spearman’s correlation value was -0.4583 with a p-value less than 0.001. It is in line with the previous studies showing that increased blood eosinophils are associated with poorly controlled asthma [17].
Limitation(s)
Asthma being more prevalent condition among Indian population, a larger sample size would have been more representative.
Conclusion(s)
Asthma control test score had a significant positive correlation with FEV1 and serum magnesium levels. It also had significant negative correlation with AEC (inflammatory marker). Hence, Asthma control test can be used as tool for treatment response in the current COVID-19 pandemic situation and also in resource limited settings.
[1]. Initiative G, Global Initiative for Asthma: Global strategy for asthma management and prevention (Updated 2020)Rev Fr d’Allergologie d’Immunologie Clin 2020 36(6):685-704.10.1016/S0335-7457(96)80056-6 [Google Scholar] [CrossRef]
[2]. Schatz M, Sorkness CA, Li JT, Marcus P, Murray JJ, Nathan RA, Asthma Control Test: Reliability, validity, and responsiveness in patients not previously followed by asthma specialistsJ Allergy Clin Immunol 2006 117(3):549-56.10.1016/j.jaci.2006.01.01116522452 [Google Scholar] [CrossRef] [PubMed]
[3]. Bahadori K, Doyle-Waters MM, Marra C, Lynd L, Alasaly K, Swiston J, Economic burden of asthma: A systematic reviewBMC Pulm Med 2009 9:2410.1186/1471-2466-9-2419454036 [Google Scholar] [CrossRef] [PubMed]
[4]. Comparison of the asthma control test and % predicted FEV1 in relation to correlation with physicians assessment of asthma control and treatment decisions;Uruj Hoda, Bogusia Kasternow, Succony Laura, Corrigan ChrisEuropean Respiratory Journal 2011 38:4029 [Google Scholar]
[5]. Wenzel SE, Eosinophils in asthma-closing the loop or opening the door?N Engl J Med 2009 360(10):1026-28.10.1056/NEJMe090033419264692 [Google Scholar] [CrossRef] [PubMed]
[6]. Horn BR, Robin ED, Theodore J, Van Kessel A, Total eosinophil counts in the management of bronchial asthmaN Engl J Med 1975 292(22):1152-55.10.1056/NEJM1975052929222041124105 [Google Scholar] [CrossRef] [PubMed]
[7]. Filley WV, Holley KE, Kephart GM, Gleich GJ, Identification by immunofluorescence of eosinophil granule major basic protein in lung tissues of patients with bronchial asthmaLancet 1982 2(8288):11-16.10.1016/S0140-6736(82)91152-7 [Google Scholar] [CrossRef]
[8]. Kılıc H, Kanbay A, Karalezlı A, Babaoglu E, Hasanoglu HC, Erel O, The Relationship between Hypomagnesemia and Pulmonary Function Tests in Patients with Chronic AsthmaMed Princ Pract 2018 27(2):139-44.Epub 2018 Feb 1810.1159/00048776029455196 [Google Scholar] [CrossRef] [PubMed]
[9]. McKeever TM, Britton J, Diet and asthmaAm J Respir Crit Care Med 2004 170(7):725-29.10.1164/rccm.200405-611PP15256393 [Google Scholar] [CrossRef] [PubMed]
[10]. Agrawal S, Pearce N, Ebrahim S, Prevalence and risk factors for self-reported asthma in an adult Indian population: A cross-sectional surveyInt J Tuberc Lung Dis 2013 17(2):275-82.10.5588/ijtld.12.043823317966 [Google Scholar] [CrossRef] [PubMed]
[11]. Ozoh OB, Bandele OE, Chukwu C, Okubadejo N, Correlation between the asthma control test score and FEV1 in Nigerians with bronchial asthmaChest 2010 138(4):146A10.1378/chest.9803 [Google Scholar] [CrossRef]
[12]. Papakosta D, Latsios D, Manika K, Porpodis K, Kontakioti E, Gioulekas D, Asthma control test is correlated to FEV1 and nitric oxide in Greek asthmatic patients: Influence of treatmentJ Asthma 2011 48(9):901-06.10.3109/02770903.2011.61195821923284 [Google Scholar] [CrossRef] [PubMed]
[13]. Chan M, Sitaraman S, Dosanjh A, Asthma control test and peak expiratory flow rate: Independent pediatric asthma management toolsJ Asthma 2009 46(10):1042-44.10.3109/0277090090333110119995144 [Google Scholar] [CrossRef] [PubMed]
[14]. Daliparty VM, Manu MK, Mohapatra AK, Serum magnesium levels and its correlation with level of control in patients with asthma: A hospital-based, cross-sectional, prospective studyLung India 2018 35(5):407-10.10.4103/lungindia.lungindia_55_1830168460 [Google Scholar] [CrossRef] [PubMed]
[15]. Whang R, Flink EB, Dyckner T, Wester PO, Aikawa JK, Ryan MP, Magnesium depletion as a cause of refractory potassium repletionArch Intern Med 1985 145(9):1686-89.10.1001/archinte.1985.003600901620244026498 [Google Scholar] [CrossRef] [PubMed]
[16]. Casciano J, Krishnan JA, Small MB, Buck PO, Gopalan G, Li C, Burden of asthma with elevated blood eosinophil levelsBMC Pulm Med 2016 16(1):10010.1186/s12890-016-0263-827412347 [Google Scholar] [CrossRef] [PubMed]
[17]. Kostikas K, Brindicci C, Patalano F, blood eosinophils as biomarkers to drive treatment choices in asthma and COPDCurr Drug Targets 2018 19(16):1882-96.10.2174/138945011966618021212001229437007 [Google Scholar] [CrossRef] [PubMed]