The origin of RCA and LCA of the heart is from the aortic sinus of Valsalva, the right arises from the anterior aortic sinus and the left from the left posterior aortic sinus, the right posterior aortic sinus is devoid of any orifice hence, known as a non-coronary sinus. The junction between the aortic dilatation and the aortic tube is known as sinotubular junction, this is represented by a well-defined circumferential supra-valvular ridge, and the coronary ostia normally open near to this ridge [1]. The morphometry of the coronary ostia is very important for various cardiovascular interventions such as cardiac catheterisation, percutaneous aortic root valve replacement, aortotomy, approach for aortic root enlargement, and surgical ostioplasty [2]. With the recent change in the lifestyle and increased stress among the various populations, coronary heart diseases are on the high rise, and several angiographies and coronary by-pass surgeries are being done on day to day basis in every hospital. According to the World Health Organisation (WHO), CHD constitutes the major cause of death in the industrial world, the risk factors being hypertension, diabetes, hyperlipidemia, and lack of physical exercise and other factors that can lead to the destruction of the vascular cells. The study of coronary ostia helps design coronary catheters or cannulas [3].
The aim of this study was to describe the location, size, and shape of the coronary ostia in cadaveric hearts and to compare the same on both RCA and LCA. This can shed more light on the anatomical knowledge on the coronary ostia necessary for the therapeutic and diagnostic cardiac interventions by both cardiologists and radiologists.
Materials and Methods
This was a descriptive cross-sectional study. The study was conducted at the dissection hall, Department of Anatomy, JSS Medical College, Mysuru, Karnataka, India. The heart specimens were obtained from the mortuary of Mysore Medical College and JSS Medical College, Mysuru, Karnataka, India. A total of 110 adult cadaveric normal human hearts were collected 90 males (82%) and 20 (18%) females with an average mean age of males 67 years and females 63 years. The adult cadaveric hearts were obtained from the Department of Forensic Medicine of JSS Medical College and Mysore Medical College and Research Institute, Mysuru, Karnataka state, during March 2017 to March 2019. A sample size of 110 was calculated using the formula 4pq/l2. The number of cadaveric hearts was collected depending on the availability of the cadavers at the time of postmortem in the mortuary.
Ethical consideration: The study protocol was reviewed and approved by the JSS Medical College Institutional Ethical Review Board. Permission to conduct the study was obtained by the Institutional Ethical Committee (JSS Institutional Ethical approval number: JSSMC/PG/6399/2016-17) of JSS Medical College, JSSAHER, Mysuru, on 01/02/2017.
Inclusion criteria: Human adult cadaveric hearts were utilised with no history of cardiovascular diseases or cardiac surgery/injury with intact coronary arteries and aortic root.
Exclusion criteria: Cadaveric hearts with a history of cardiac injuries/trauma, cardiac surgeries, stent insertions, and cardiomegaly were not utilised for this study.
Data entry: All the morphological and morphometric measurements like the location, size and shape of both the coronary ostia were entered into the excel sheet by the investigator. The data was verified by rechecking all the parameters and validity ensured by randomly selecting 10% of observations and an average of three means were taken after each measurement of a parameter; this was cross-checked again while entering the data for any errors.
Procedure: The thoracic cavity was exposed after cutting the ribs and sternum, the parietal pericardium was incised along with the great vessels to remove the heart from the thoracic cavity. Each specimen was immediately washed thoroughly in running tap water to remove all the blood clots and debris from the major vessels of the heart. The aorta and pulmonary trunk were identified and incised transversely about 3-4 inches above the supra-valvular ridge. The aortic root was incised vertically and the three aortic sinuses were identified along with their coronary ostia. A vertical incision was made along the tubular wall of the non-coronary sinus for clear visualisation of both the ostia. A vernier caliper was used to measure the diameters of RCO and LCO. The presence of any single or multiple coronary ostia was observed. In the present study, the following observations were recorded and analysed statistically.
The diameter of the coronary ostia;
The location of coronary ostia;
Variations in the shape of the coronary ostia and
Presence of anomalous accessory coronary orifices.
Statistical Analysis
All data was analysed using SPSS software, version 22.0. Descriptive statistics were obtained. Independent t-tests were done for continuous variables. Pearson’s chi-square tests were done to study the coronary ostia and morphometric differences between RCA and LCA. The p-value less than 0.05 considered significant.
Results
The aortic valves did not show any variations; in all the 110 specimens the three aortic cusps were normal. No openings were observed in the non-coronary sinus.
1. Diameter of coronary ostia: The average diameter of the RCO was 3.43±0.389 mm and the LCO was 3.66±0.40 mm. [Table/Fig-1] shows the measurement of the diameter of the coronary ostia being taken using the digital vernier calipers.
Measurement of the coronary ostium using digital vernier calipers.

[Table/Fig-2] shows the comparison of the diameters of RCO and LCO. There is a statistically significant difference in diameters of RCO and LCO. The diameter of LCO was found to be greater than the RCO.
Comparison of the diameters of right and left coronary ostia.
| Side of coronary ostia | Frequency (n) | Mean (mm) | Standard deviation | p-value |
|---|
| Right | 110 | 3.43 | 0.38 | <0.001 |
| Left | 110 | 3.66 | 0.40 |
*Independent Sample t-test; n: Number of specimens
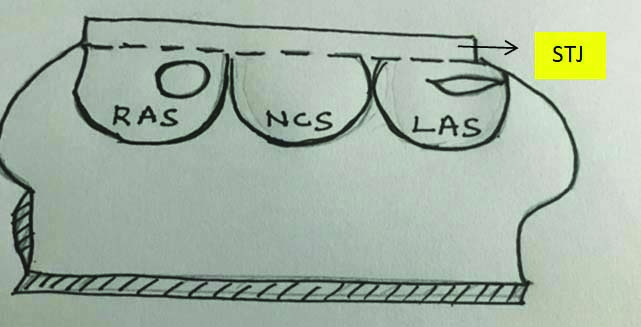
2. Location of coronary ostia: Normally the RCA arises from the right anterior aortic sinus and the LCA from the left posterior aortic sinus. In present study, the RCA in all the 110 hearts was seen taking origin from the anterior aortic sinus and the left from the left posterior aortic sinus. No anomalous origin from the non-coronary sinus was observed [Table/Fig-3].
The normal location and shapes of coronary ostia.
STJ: Sinutubular junction; RAS: Right aortic sinus; NCS: Non-coronary sinus; LAS: Left aortic sinus
[Table/Fig-4] shows the frequency and percentage of variations in the location of RCO and LCO. The percentage of the presence of RCO and LCO within the sinus was found to be greater than the ostia present in the STJ. No openings were observed at the tubular level.
Showing the frequency and percentage of different locations of right and left coronary ostia.
| Side | Location of coronary ostia | Frequency (%) |
|---|
| Right | Sinus | 85 (77.3) |
| Sinutubular junction | 25 (22.7) |
| Tubular | 0 (0) |
| Total | 110 (100) |
| Left | Sinus | 81 (73.6) |
| Sinutubular junction | 29 (26.4) |
| Tubular | 0 (0) |
| Total | 110 (100) |
3. Variations in the shape of coronary ostia: Three types of shapes have been observed like, Circular (C), Horizontally Elliptical (HE) and Vertically Elliptical (VE).
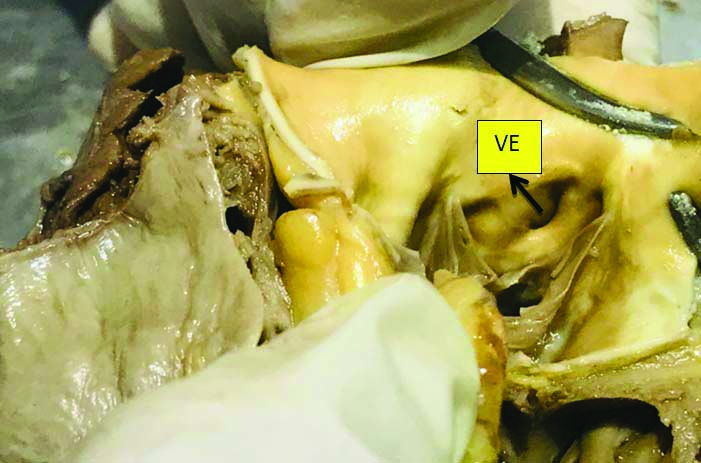
The [Table/Fig-5] heart specimen below shows the presence of VE right coronary ostium in the right aortic sinus.
The heart specimen showing the Vertically Elliptical (VE) coronary orifice.
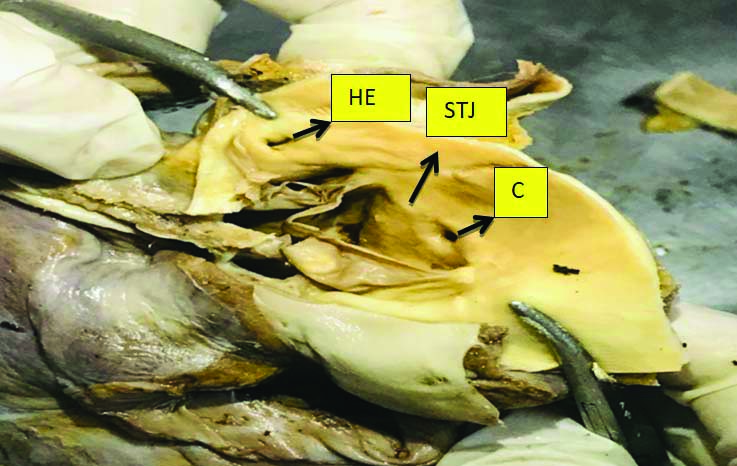
The [Table/Fig-6] heart specimen below shows different shapes of coronary ostia at STJ, the RCO showing the circular shape (C) and the LCO showing HE shape of coronary ostia within the aortic sinus.
The heart specimen showing the circular (C) and Horizontally Elliptical (HE) coronary Ostia seen at the Sinu-Tubular Junction (STJ).
The [Table/Fig-7] shows the frequency and percentage of variations in the shape of RCO and LCO. In 70.9% of cases the RCO was circular in shape, whereas the LCO was circular in 52.7% of cases, the highest frequency was seen with the circular shape, next was the HE and lastly the VE shape.
The frequency and percentage of different shapes of coronary ostia in present study.
| Side | Shape of coronary ostia | Frequency (%) |
|---|
| Right | Horizontally elliptical | 30 (27.3) |
| Circular | 78 (70.9) |
| Vertically elliptical | 02 (1.8) |
| Total | 110 (100) |
| Left | Horizontally elliptical | 45 (40.9) |
| Circular | 58 (52.7) |
| Vertically elliptical | 07 (6.4) |
| Total | 110 (100) |
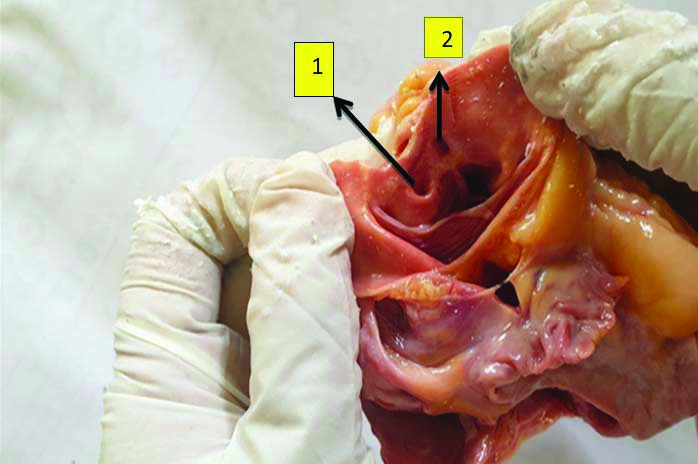
4. Presence of a single accessory coronary ostia/Third Coronary Artery (TCA): Single right accessory coronary ostia was present in 9% (10/110) and the LCO did not show any accessory ostia 0%. Double TCA was seen in three hearts (2.7%). [Table/Fig-8] shows the heart specimen with the anterior aortic sinus, with a single RCA Ostium and a single accessory coronary Ostium/TCA opening in the anterior aortic sinus in close relation to the RCA orifice.
Showing the heart specimen with a single accessory coronary ostia (1) in close relation to the right coronary orifice (2).
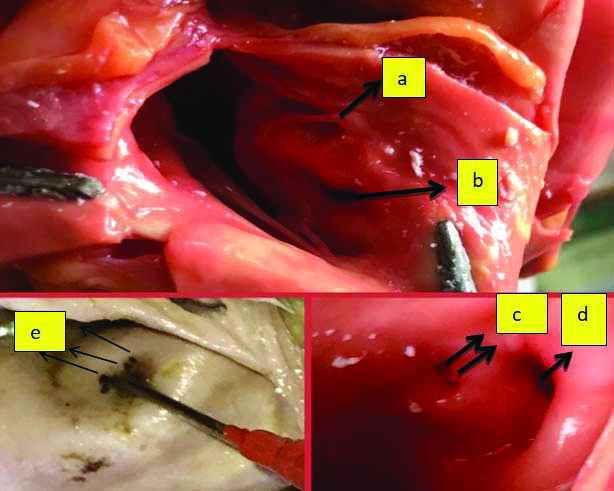
5. Presence of multiple small accessory coronary ostia: Multiple right accessory ostia were seen in 7.27% (08/110) and there were no multiple ostia in the left coronary sinus 0%. The Sinoatrial (SA) nodal artery; vasa vasorum to the pulmonary trunk and ventricular branch of RCA was seen arising from the anterior aortic sinus apart from the TCA. Such a finding is rare and presence of this anastomotic arterial circle is an advantage since it indicates an important communication between the RCA and LCA. Totally, the presence of TCA was observed in 11.8% (13/110) of cases, 12 were male cadavers and one was female cadaver. There was no statistically significant difference in the parameters of the location, size, or shape of the coronary ostia among the males and females. [Table/Fig-9] shows the heart specimen showing the presence of RCA Ostia and accessory coronary orifice, presence of double accessory coronary ostia and presence of multiple accessory coronary ostia in the anterior aortic sinus. The probe in the figure represents the RCA Ostia.
The heart specimens showing multiple accessory coronary ostia arising from the anterior aortic sinus along with the right coronary ostia. a: Single 3rd coronary artery; b: Right coronary ostia; c: Double 3rd coronary artery; d: Right coronary ostia; e: Multiple accessory coronary ostia.
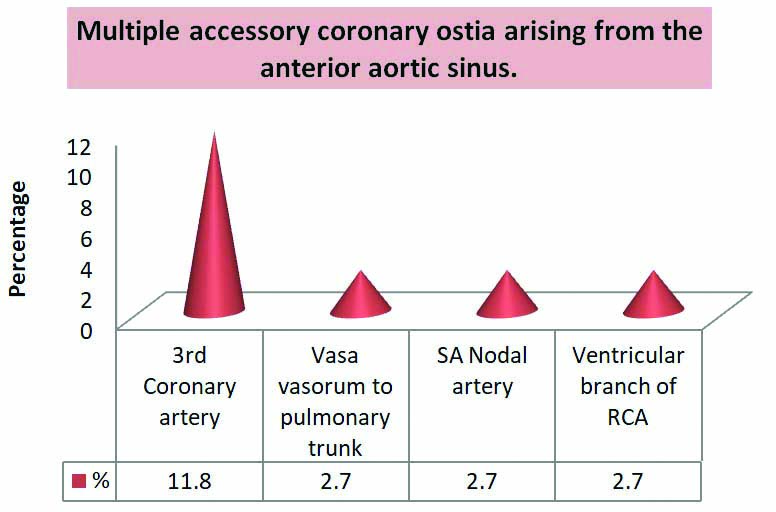
[Table/Fig-10] depicts the percentage of the multiple accessory coronary ostia arising from the anterior aortic sinus along with the TCA in present study. The incidence of TCA was 11.8% and other orifices for vasa vasorum to the pulmonary trunk, SA nodal artery and ventricular branch of RCA were found to be 2.7% in present study. In all the 110 hearts, the accessory orifices were observed in the anterior aortic sinus in close relation to the right coronary orifice.
Graphical representation of multiple accessory ostia seen in anterior aortic sinus.
Discussion
The cardiac catheterisation of the coronary arteries is done for either therapeutic or diagnostic intervention. It is done for evaluation and treatment of various heart diseases like coronary or myocardial diseases, measurement of haemodynamics in the heart, measurement of saturation and cardiac output, evaluation of left ventricular function, evaluation and treatment of cardiac arrhythmias. It was Claude Bernard who first placed the catheters into the arteries and veins of the horses. In 1929, it was Forssmann and Cournand, the Nobel Laureates who performed the revolutionary catheterisation of human hearts. In 1959, it was Sones who introduced the selective catheterisation technique for coronary angiography. In 1967 Ampaltz described the femoral route of introducing selective coronary catheters through the perpendicularly placed coronary Ostia [4-6]. Judkin’s or Amplatz cannulas are most commonly used for coronary arteriography in the recent years. The emergence of the coronary artery orifices is a result of more of ingrowth rather than an outgrowth of the arterial channels. The mechanism considered reinforcing the theory of ingrowth to the development of coronary arteries is:
i) The role of neural crest cells;
ii) Growth factors: Vascular Endothelial Growth Factor (VEGF) family members [7].
A study conducted in 2017 by Surekha WM et al., mentions the following clinical significance of the anatomical knowledge of coronary ostia [8]. It has been found that the presence of anomalous ostia can cause difficulty in cannulation of vessels during open-heart surgeries; in coronary arteriography and angiography an aortic root injection of dye is given to locate many ostia, anomalous ostia can cause fatal outcome; multiple coronary ostia may be associated with cardiac abnormalities like hypertrophic cardiomyopathy; knowledge of accessory ostia is important to interpret angiographic findings correctly; ectopic origin of right conus artery from the right aortic sinus is also known as TCA, it forms a separate path of anastomosis between the RCA and LCA [8].
According to Prajapati BSK et al., the coronary ostia above the STJ remains open during systole and diastole, this causes continuous blood flow and decreases coronary insufficiency [9]. In contrast, Joshi SD et al., stated that the aortic cusp does not flatten against the walls of the aortic sinus even at maximum systolic pressure [10]. Therefore, the ostia above the STJ is not advantageous. A high take-off of the coronary artery can lead to serious clinical implications like myocardial infarction and sudden cardiac death. However, it has been suggested that the location of ostia within the aortic sinus or below the STJ is functionally advantageous [10].
In present study, also the LCO (3.66±0.40 mm) had a greater diameter than the RCO (3.43±0.38 mm). [Table/Fig-11] shows the comparison of the mean diameters of the coronary ostia of present study with the previous studies [2-4,11,12].
Comparison of the diameters of the coronary ostia among different population with present study [2-4,11,12].
| Studies (Publication year) | Population | Sample size | RCO (mm) | LCO (mm) |
|---|
| Cavalcanti JS et al., [11] (2003) | Brazil | 51 | 3.46±0.94 | 4.75±0.93 |
| Kaur D et al., [12] (2012) | North India | 77 | 3.9±1.0 | 4.6±1.0 |
| Kulkarni JP and Vaishali P [2] (2015) | North India | 90 | 2.5±1.0 | 2.8±1.0 |
| Jyothi SR and Dakshayani KR [3] (2017) | India | 49 | 3.4±0.9 | 4.3±0.7 |
| Iman S et al., [4] (2017) | East India | 40 | 4.19±0.36 | 4.41±0.4 |
| Present study (2021) | South India | 110 | 3.43±0.38 | 3.66±0.40 |
In present study, the percentage of circular shape was found to be highest in both RCO (70.9%) and LCO (52.7%) compared to the other shapes. [Table/Fig-12] shows comparison of the percentages of different shapes of coronary ostia among various population [2,13,14].
Comparison of the percentages of different shapes of coronary ostia among various population with present study [2,13,14].
| Studies (Publication year) | Sample size | Population | Right coronary ostia (%) | Left coronary ostia (%) |
|---|
| HE | C | VE | HE | C | VE |
|---|
| Gosva F et al., [13] (2010) | 100 | Turkey | - | 60 | - | - | 55 | - |
| Kulkarni JP and Vaishali P [2] (2015) | 90 | North India | 76 | 16 | 7 | 73 | 23 | 10 |
| Jeshika SL et al., [14] (2019) | 50 | South Africa | 24 | 52 | 24 | 60 | 30 | 10 |
| Present study (2021) | 110 | South India | 27.3 | 70.9 | 1.8 | 40.9 | 52.7 | 6.4 |
HE: Horizontally elliptical; C: Circular; VE: Vertically elliptical
A study conducted by Cihan A et al., observed the angiographic incidence of anomalous aortic origins of the coronary arteries in 44.7% of patients. This study suggested that such anomalous coronary ostia can help to design appropriate catheters for angiographies [15].
In present study also, all the accessory coronary ostia were situated below the supra-valvular ridge/STJ. Banchi A in 1904 reported the highest percentage being 71% of RCO located at STJ [16] and 48% of LCO located at STJ compared to the other locations [17]. Wilkins CE in 1988 observed only the tubular locations of both the RCO and LCO [18]. Reig J and Petit M reported 56% of RCO and LCO being located in the sinus region and at STJ, no tubular location were found [19]. In present study also no tubular locations were found in all 110 hearts. Vaishaly KB and Arole V reported the STJ being the commonest position compared to other locations, RCO in 62% of cases and LCO in 66% of cases were seen located at STJ [20].
Schlesinger MJ et al., (1949) was the first author to describe the TCA in detail, he mentioned that it supplied the right ventricle and inter-ventricular septum [21].
In present study, the RCO (77.3%) and LCO (73.6%) were located within the sinus, the RCO (22.7%) and LCO (26.4%) were located at STJ and no tubular locations were observed. The [Table/Fig-13] below shows the comparison of percentages of different locations of coronary ostia of previous authors with present study [3,16,18-20]. [Table/Fig-14] shows comparison of the incidence of third coronary artery with other studies [3,17,19,20,22,23]. [Table/Fig-15] shows comparison of the anomalous origin of different arteries from the anterior aortic sinus [3,20,24].
Comparison of the percentages of different locations of the right and left coronary ostia of previous studies with present study [3,16,18-20].
| Authors (Publication year) | RCO/LCO | Sinus (%) | STJ (%) | Tubular (%) |
|---|
| Banchi A [16] (1904) | RCO | 10 | 71 | 19 |
| LCO | 18 | 48 | 34 |
| Wilkins CE et al., [18] (1988) | RCO | - | - | 8 |
| LCO | - | - | 8 |
| Reig J and Petit M [19] (2004) | RCO | 56 | 56 | - |
| LCO | 56 | 56 | - |
| Bharambe VK and Arole V [20] (2012) | RCO | 22 | 62 | 16 |
| LCO | 10 | 66 | 24 |
| Jyothi SR and Dakshayani KR [3] (2017) | RCO | 89.8 | 8.2 | 3 |
| LCO | 38.7 | 53.1 | 8.2 |
| Present study (2021) | RCO | 77.3 | 22.7 | 0 |
| LCO | 73.6 | 26.4 | 0 |
Comparison of the incidence of 3rd coronary artery with the previous studies [3,17,19,20,22,23].
| Author (Publication year) | Percentage (%) |
|---|
| Reig J and Petit M [19] (2004) | 33-51 |
| Kalpana R [17] (2004) | 24 |
| Stankovic I and Jesic M [24] (2004) | 34.8 |
| Koenig PR and Hijazi ZM [23] (2005) | 50 |
| Bharambe VK and Arole V [20] (2012) | 22 |
| Jyothi SR et al., [3] (2017) | 10.2 |
| Present study (2021) | 11.8 |
Comparison of the anomalous origin of different arteries from the anterior aortic sinus (apart from the 3rd coronary artery) [3,20,24].
| Previous studies (Publication year) | Anomalous origin from the anterior aortic sinus |
|---|
| Mc Alpine WA [24] (1975) | Ventricular branch of RCA |
| Bharambe VK and Arole V [20] (2012) | SA nodal artery, circumflex branch, vasa vasorum to the pulmonary trunk, ventricular branch of RCA. |
| Jyothi SR and Dakshayani KR [3] (2017) | Ventricular branch of RCA. |
| Present study (2021) | SA nodal artery, vasa vasorum to the pulmonary trunk, ventricular branch of RCA. |
Muriango M et al., (1997) reported the 3rd coronary ostia in the anterior aortic sinus in five hearts and a single coronary ostia in five hearts [25].
In present study, it was observed that the SA nodal artery; vasa vasorum to the pulmonary trunk and ventricular branch of RCA arising from the anterior aortic sinus apart from the TCA. Such a finding is rare and presence of this anastomotic arterial circle (circle of Vieussens) is an advantage since it indicates the communication between the RCA and LCA. Manisha RD et al., in her study stated the incidence of TCA in 48 out of 150 hearts (32%), in 42 hearts (28%) with a single TCA, and in 6 hearts (4%) double TCA was noted. All were closely related to the RCO. In two cases, 4 ostia were observed, one for RCA, 2 for TCA and 1 for the pulmonary trunk [26]. Gajbe UL et al., conducted study in 30 cadaveric hearts and found the presence of TCA in 2 hearts (6%) and presence of anomalous origin of RCA, SA nodal artery and vasa vasorum of pulmonary trunk as 3 separate openings in the anterior aortic sinus in 3 hearts (10%) [27]. Urbanski PP et al., performed the ascending aorta replacement in patient with coronary ostia localised above the sinotubular junction by slide-plasty of an aberrant coronary artery. Transposition of the anomalous coronary artery origin from the replaced ascending aorta into the normal sinus of valsalva using slide-plasty was considered as a simple and safe surgical procedure for which a sound anatomical knowledge of the size, location and shape of the coronary Ostia is essential for the operating surgeon in the same population [28].
Limitation(s)
The major limitation was that the number of female cadaveric hearts was comparatively less than the male hearts. This study will help in interventional studies by cardiologist and radiologists during diagnostic and therapeutic approach in coronary vascular disease and its management. The present study of size, location and shape of the coronary ostia will also help to design appropriate catheters and cannulas for coronary angiography and cardiac interventions for the same population.
Conclusion(s)
The diameter of the LCO was found to be greater than the RCO and the shape was circular in most of the coronary ostia. The majority of the coronary ostia were found to be located within the aortic sinuses below the STJ. This anatomical study will enhance the clinical knowledge of the variations associated with the coronary ostia and will greatly help the radiologists performing coronary angiographies.
*Independent Sample t-test; n: Number of specimens
HE: Horizontally elliptical; C: Circular; VE: Vertically elliptical