A Rare Case of Scapulothoracic Bursitis of the Chest Wall with Numerous Rice Grain like Loose Bodies- A Pathological Correlation
KR Chatura1, CN Aarthy2
1 Professor, Department of Pathology, J.J.M Medical College, Davangere, Karnataka, India.
2 Postgraduate, Department of Pathology, J.J.M Medical College, Davangere, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. KR Chatura, Professor, Department of Pathology, J.J.M Medical College, Davangere-577004, Karnataka, India.
E-mail: chaturakr@gmail.com
Scapulothoracic bursitis is a rare disease which is caused from the inflammation of the bursa secondary to trauma or its overuse, owing to sports activities or work. It usually presents with pain, swelling without redness at the scapulothoracic interface. A 22-year-old male presented to the surgeon with the swelling in the left scapular region following a history of trauma. Ultrasound (USG) showed a large loculated fluid collection with internal debris outside the muscular plane. With the clinical diagnosis of haematoma surgical resection was done. It showed a cystic swelling containing haemorrhagic fluid attached to the chest wall. The specimen was sent for histopathological correlation. The thickened cystic structure had numerous rice grain like loose bodies on the inner surface. Microscopy showed fibrocollageneous wall with congested blood vessels, granulation tissue, fibrinoid bodies and macrophages. This case report describes a cystic lesion in left scapular region diagnosed as a case of scapulothoracic bursitis based on pathological correlation. Surgery was an effective treatment for this case with no complication and recurrence on follow-up.
Bursa, Fibrinoid bodies, Trauma
Case Report
A 22-year-old male, presented to the surgeon with the swelling in the left infrascapular region for a month [Table/Fig-1]. He had a history of fall three months back before the onset of the swelling. He complained of pain during movements of upper extremities. On examination, the swelling appeared to become prominent during elevation and anteflexion of upper extremities. It was firm in consistency, non-mobile and tender during palpation and a clinical diagnosis of haematoma was made as there was a history of fall. USG showed a large loculated fluid collection with internal debris outside the muscular plane and x-ray showed a soft tissue swelling [Table/Fig-2]. Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) were not done. Surgery was planned as the swelling did not subside by traditional methods like cold compression, topical anticoagulants and range of movements involving the upper extremities were restricted.
Swelling in left infrascapular region.

X-ray of lateral view of chest showing a soft tissue mass in infrascapular region.

Surgical resection under general anaesthesia yielded a cystic swelling containing haemorrhagic fluid attached to the chest wall. The cystic swelling was opened and numerous rice grain like loose bodies were seen inside [Table/Fig-3] and haemorrhagic fluid was drained out. The provisional diagnosis of haematoma with fibrin thrombi was considered by the surgeon. The specimen was sent to the Pathological Department, measured about 16×8.5×1 cm. The thickened cyst wall was congested and the inner shaggy cyst wall had numerous attached and friable membranous fibrinous exudates and rice grain like loose bodies [Table/Fig-4].
Numerous rice grain like loose bodies seen inside the cystic swelling.

A cut open cystic structure measuring 16×8.5×1 cm with multiple rice grain like bodies.

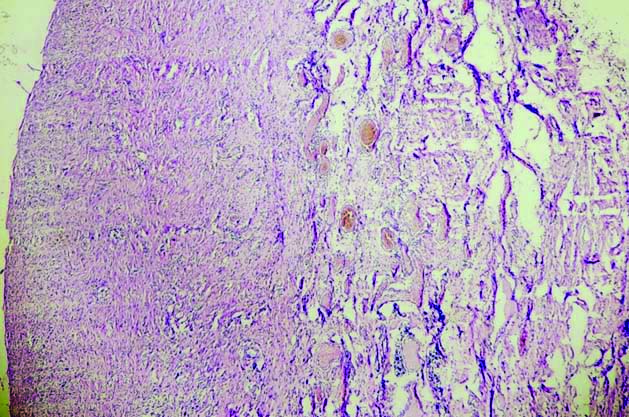
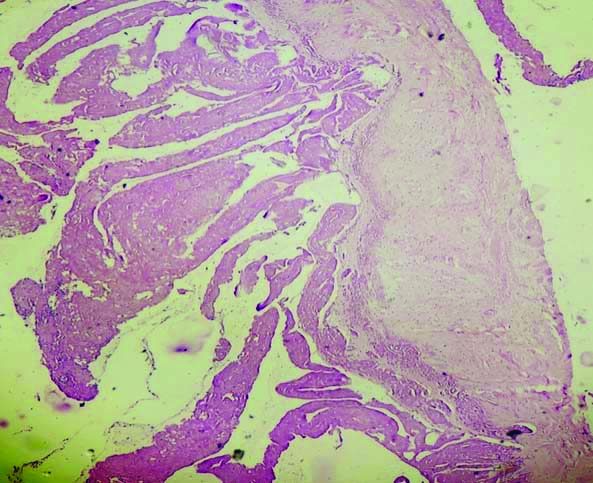
Microscopically, the thickened cyst wall showed fibrocollagenous tissue with congested blood vessels and proliferating granulation tissue [Table/Fig-5]. There was also fibrin deposition with inflammatory infiltrates predominantly constituting neutrophils and scattered haemosiderin laden macrophages as villous like structures [Table/Fig-6]. The rice grain like loose bodies found inside the cyst wall was made up of fibrin.
Cystic structure showing fibrocollageneous stroma and congested blood vessels (H&E, 200X).
Villous like projection of fibrin (H&E, 400X).
Thus, based on the location of the swelling which showed rice grain like loose bodies and histopathological correlation, the cystic swelling was diagnosed as Scapulothoracic Bursitis. The patient was followed-up after surgery for a month and there was no recurrence.
Discussion
Scapulothoracic bursitis is a rare disease which is caused by the inflammation of the bursa secondary to trauma or its overuse, owing to sports activities or work [1]. It usually presents with pain, swelling without redness at the scapulothoracic interface. Magnetic resonance remains the best imaging tool and is treated by conservative methods or surgery.
Scapulothoracic articulation has two anatomic bursae and four adventitious bursae. Of the two major anatomic bursae, the supraserratus bursa lies between the serratus anterior muscle and subscapularis muscle, the infraserratus bursa is between the serratus anterior muscle and thoracic wall. These bursae provide the sliding movement to the scapulothoracic joint [2-4]. In this case, infraserratus bursa was involved.
Scapulothoracic bursitis presents as pain or swelling of the bursa at the scapulothoracic articulation [5]. The pathogenesis involves the chronic repeated mechanical stress either by bony abnormalities of the scapula or rib cage. Soft tissues of the scapulothoracic joint will be damaged during many sports or due to overuse and in work which involves repeated movements of the scapula against the posterior thoracic wall [3,5]. Osteochondroma can also manifest with recurrent bursitis and its malignant transformation can be identified by histopathological examination and MRI [6].
Magnetic resonance is the best imaging tool for identifying scapulothoracic bursitis which appears as a well-demarcated cystic mass between the serratus anterior muscle and the thoracic rib cage [7]. The other chest wall masses in this region include elastofibroma, abscess, haematoma and sarcomas. A distended scapulothoracic bursa can be distinguished from other soft tissue masses with the aid of CT and MRI [8].
Conservative treatments for scapulothoracic bursitis involve rest, shoulder exercises, local hot compresses, anti-inflammatory drugs, intracystic injection of a long-acting corticosteroid or ethanol and ionophoresis for symptomatic cases. Surgical intervention could be applied for coexistent osseous lesions or when conservative treatment has failed [8]. However, the complication of pneumothorax, haematoma, damage of nerve and recurrence are associated with surgery.
Grossly, the scapulothoracic bursitis presents as a thick walled cystic structure with light yellow coloured fluid. Inside the cystic structure, numerous villi and rice grain like bodies can be seen, as noticed in this case. These rice like bodies are seen in joints or bursae in conditions like rheumatoid arthropathy, seronegative inflammatory arthritis and tuberculosis joint. These rice bodies are formed secondary to the synovial inflammation [8]. Histologically, bursitis shows a cystic lesion with a dense fibrotic wall covered by synovial lining having papillary projections and capillary proliferation. In the lumen of the cyst there can be blood clots with presence of fibrinoid substances, siderophages, lymphocytes, neutrophils and giant polynuclear cells [9,10]. The rice bodies are composed of fibrin deposition with fibroblast and mononuclear infiltrates.
Conclusion(s)
This case report describes a cystic lesion in left scapular region unsuspected by the clinician and diagnosed as a case of scapulothoracic bursitis based on pathological correlation. Scapulothoracic bursitis which is rare and in this case secondary to trauma can be missed. Demonstration on gross and microscopy of numerous rice grain like loose bodies was the highlight of this case. Surgery was found to be effective treatment for this case with no complication and recurrence.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 01, 2020
Manual Googling: Dec 16, 2020
iThenticate Software: Jan 25, 2021 (17%)
[1]. Conduah AH, Baker CL, Baker CL, Clinical management of scapulothoracic bursitis and the snapping scapulaSports Health 2010 2:147-55.10.1177/194173810933835923015932 [Google Scholar] [CrossRef] [PubMed]
[2]. Williams GR, Shakil M, Klimkiewicz J, Iannotti JP, Anatomy of the scapulothoracic articulationClin Orthop Relat Res 1999 359:237-46.10.1097/00003086-199902000-0002710078149 [Google Scholar] [CrossRef] [PubMed]
[3]. Seol SJ, Han SH, Scapulothoracic bursitis in a patient with quadriparesis: A case reportMedicine (Baltimore) 2015 94:e75210.1097/MD.000000000000075225906107 [Google Scholar] [CrossRef] [PubMed]
[4]. Kuhn JE, Plancher KD, Hawkins RJ, Symptomatic scapulothoracic crepitus and bursitisJ Am Acad Orthop Surg 1998 6:267-73.10.5435/00124635-199809000-000019753753 [Google Scholar] [CrossRef] [PubMed]
[5]. Son SA, Lee DH, Lee YO, Lee SC, Kim KJ, Cho JY, Operative management in a patient with scapulothoracic bursitisKorean J Thorac Cardiovasc Surg 2013 46:486-89.10.5090/kjtcs.2013.46.6.48624368981 [Google Scholar] [CrossRef] [PubMed]
[6]. Maras Ozdemır Z, Karakaplan M, Kahraman AS, Karadag N, Adventitious bursitis overlying an osteochondroma of the humerus facing the thoracic wallCase Rep Radiol 2013 2013:93937210.1155/2013/93937224369522 [Google Scholar] [CrossRef] [PubMed]
[7]. Higuchi T, Ogose A, Hotta T, Okamoto K, Kamura T, Sasai K, Clinical and imaging features of distended scapulothoracic bursitis: Spontaneously regressed pseudotumoral lesionJ Comput Assist Tomogr 2004 28:223-28.10.1097/00004728-200403000-0001215091127 [Google Scholar] [CrossRef] [PubMed]
[8]. Joshi PS, Severe sub-acromial bursitis with rice bodies in a patient with rheumatoid arthritis: A case report and review of literatureMalays Orthop J 2018 12:52-55.10.5704/MOJ.1807.01030112130 [Google Scholar] [CrossRef] [PubMed]
[9]. Dzian A, Skalicanova M, Fucela I, Malik M, Micak J, Bilateral cystic lesions of the chest wall: Presentation of scapulothoracic bursitisInt J Surg Case Rep 2019 54:116-19.10.1016/j.ijscr.2018.11.03530641437 [Google Scholar] [CrossRef] [PubMed]
[10]. Huang CC, Ko SF, Ng SH, Lin CC, Huang HY, Yu PC, Scapulothoracic bursitis of the chest wall-sonographic features with pathologic correlationJ Ultrasound Med 2005 24:1437-40.10.7863/jum.2005.24.10.143716179630 [Google Scholar] [CrossRef] [PubMed]