Case Report
Case 1
A 25-year-old male patient was referred to the Department of Prosthodontics for replacement of missing upper front teeth, which he had lost due to road traffic trauma a few years ago. The patient had undergone orthodontic treatment for malocclusion, which was started approximately two years back and once the desired mesio-distal width (20.6 mm) between proximal surfaces of 12 and 23 was achieved for replacement of the missing anterior teeth, he was referred to the Department of Prosthodontics for review. The patient did not gave history of wearing any prosthesis at the time of presentation to us. There was no relevant medical history and on clinical examination, it was revealed that both maxillary central incisors i.e., 11, 21 and left maxillary lateral incisor i.e., 22 were missing. The occlusion was stable.
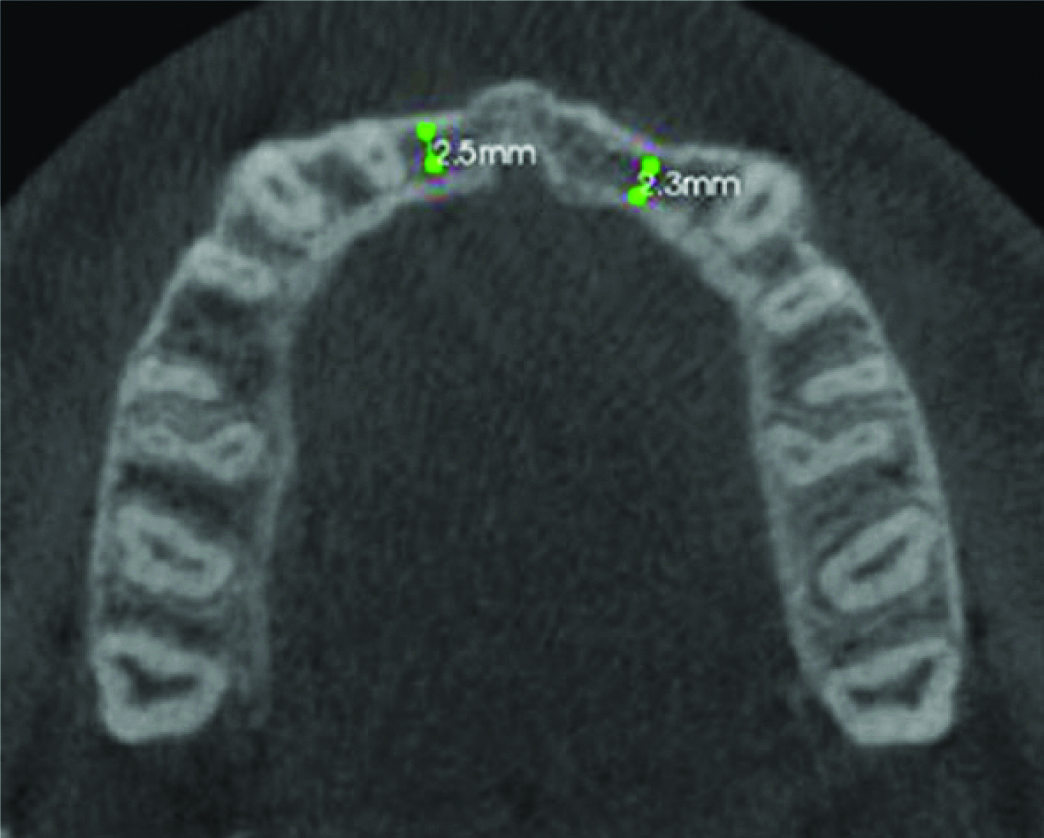
Cone Beam Computed Tomography (CBCT) revealed that labio-palatal bony dimensions were nonfavourable for any type of implant placement (2.5 mm in 11 and 22 and 2.3 mm in 22 region) [Table/Fig-1].
CBCT section showing bone anatomy with labial bone loss in case 1.
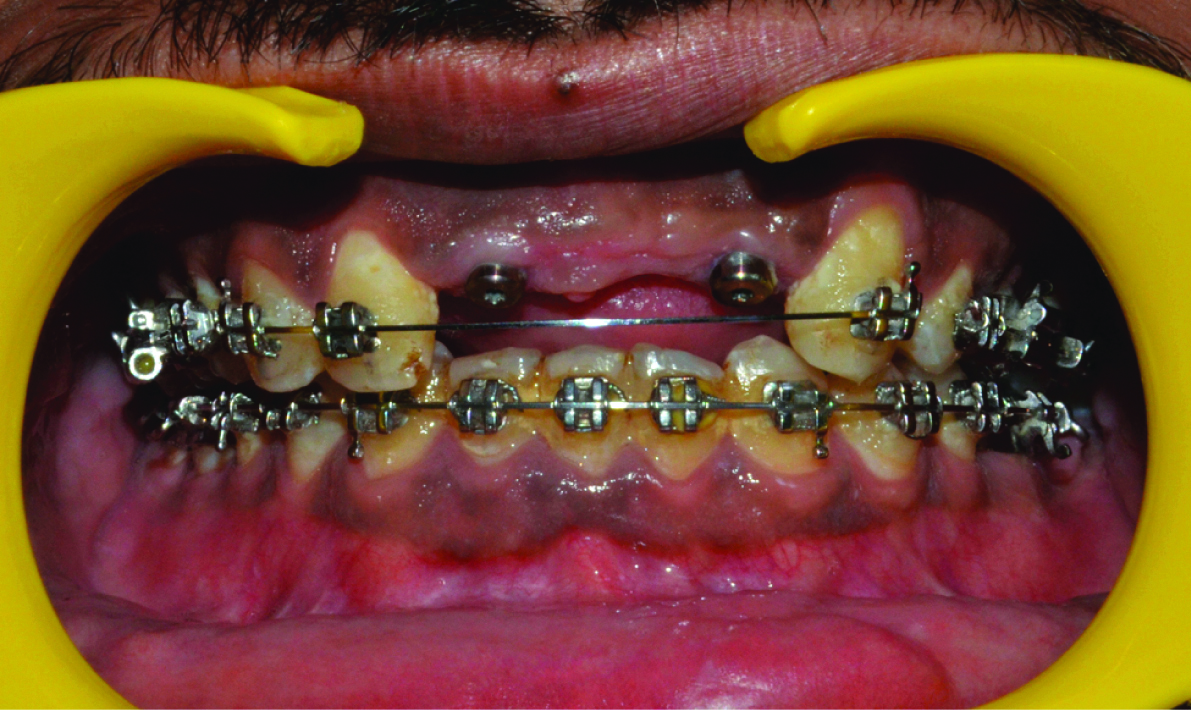
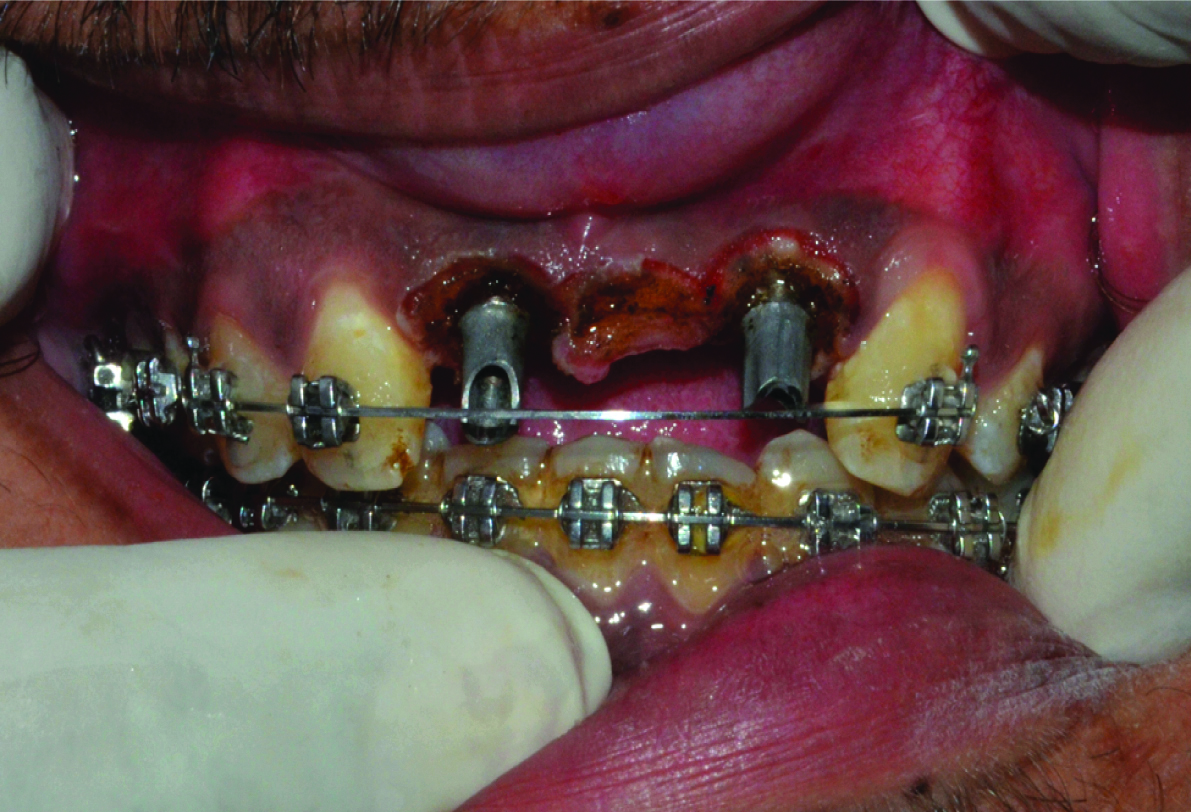
To gain some bone width, horizontal bone augmentation was performed by the oral surgeon using block bone grafting after chin harvesting. Assessment after three months of bone grafting revealed an adequate gain in bone width; hence, two dental implants were planned in 11 and 22 region followed by a three-unit implant supported prosthesis from 11 to 22 (21 as pontic). This prosthetic plan was based on best sites for implant placement avoiding the site 21 because of a deficient bone resulting in labial concavity despite block grafting spanning the whole edentulous site. Patient’s consent was taken and two dental implants (narrow platform with conical connection, 3.5×11.5 mm, Nobel Replace, Nobel Biocare India Pvt., Ltd.,) were placed in 11, 22 positions by an oral surgeon in the available bone. Implants were exposed in oral cavity after 3 months and patient was then referred to us for fabrication of prosthesis [Table/Fig-2].
Gingival levels after initial presentation after second stage surgery exposure.
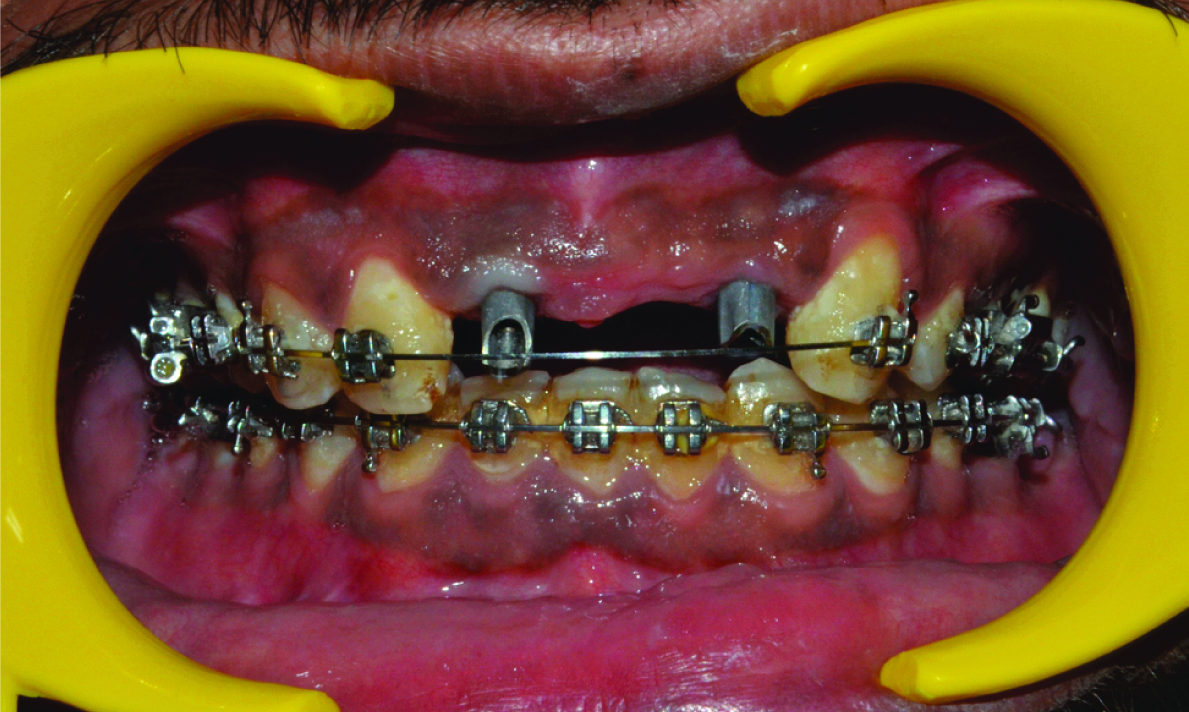
A standard procedure of splinted open tray indirect implant level impression was made and models were fabricated. Three-unit prosthesis was fabricated on custom implant abutments. However, during the trial appointment, it was observed that the coronal structures of all three prosthetic units were shorter and uneven in their inciso-gingival dimension than desired to give satisfactory aesthetics [Table/Fig-3,4].
Gingival positions with planned abutments.
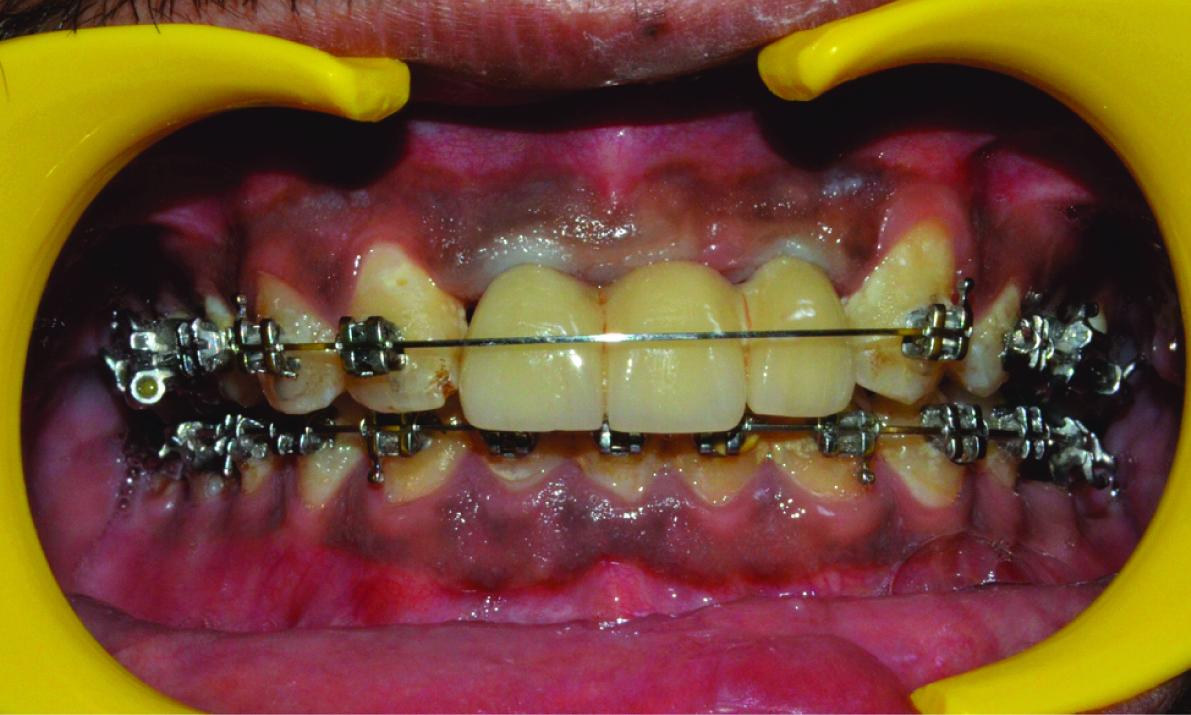
Mismatch of gingival zeniths of implant supported prosthesis vs natural teeth and unsatisfactory aesthetics.
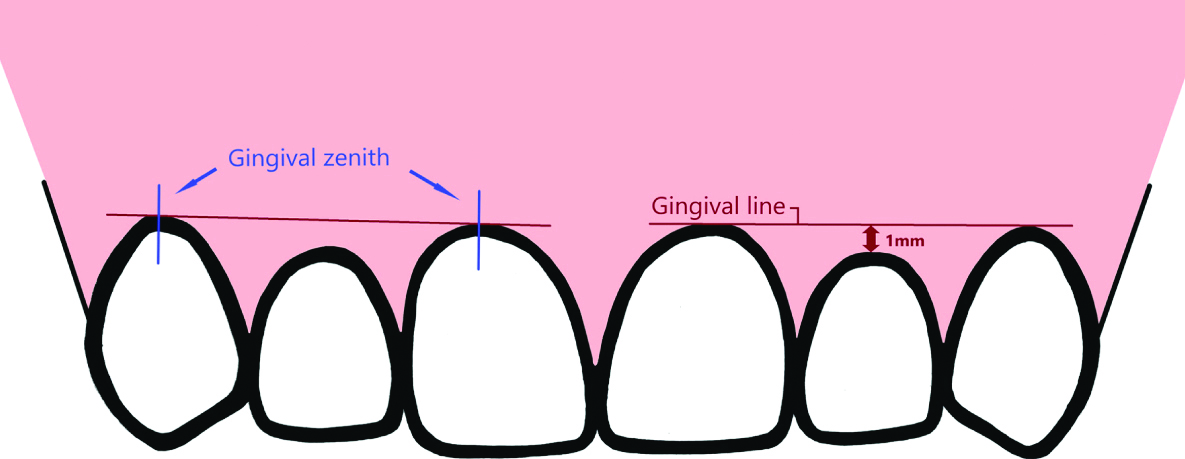
Ideally, the gingival line, which is established by joining the tangents of the gingival zenith of maxillary central incisor and canine, follows the contour of the upper lip symmetrically on both sides. The lateral incisors should have the gingival zenith approximately 1 mm coronal to this gingival line [Table/Fig-5] [1].
Ideal zenith positions with gingival line of anterior teeth.
But in this case, the gingival zeniths of all the three units were placed coronal as compared to maxillary canine and thus the gingival line being coronal as well [Table/Fig-3,4].
After appropriate radiographic and clinical examination of dental implants and adjoining hard and soft tissues, including the evaluation of gingival biotype, sulcus depth, bone level, etc., a decision to perform gingivectomy using diode laser was made. Patient’s informed consent was taken, topical anaesthesia was administered and the procedure was performed with proper isolation. Diode laser (Biolitec, Germany) with a wavelength of 980 nm with 200-micrometer fibre diameter was used at 4W power setting in contact type treatment mode. Necessary gingival sulcus measurements were made all around the implant abutments [Table/Fig-6] and planned free gingival margin was marked to create bleeding spots using a UNC 15 periodontal (Hu-Friedy) probe. The final position determined came out to lie roughly 2 mm apical to the initial levels [Table/Fig-6].
Comparative Preoperative and Postoperative Gingival sulcus measurements on facial (F), palatal (P), mesial (M) and distal sides (D) (in mm) for cases 1 and 2.
| M | MF | F | DF | D | DP | P | MP |
|---|
| Patient 1- Tooth 11 |
| Pre-Op | 2 | 2.5 | 3 | 3 | 3 | 3 | 1 | 1 |
| Post-Op | 2 | 1 | 1 | 1 | 3 | 3 | 1 | 1 |
| Patient 1- Tooth 22 |
| Pre-Op | 2 | 2 | 3 | 3 | 4 | 4 | 1 | 3 |
| Post-Op | 2 | 1 | 1 | 1 | 4 | 4 | 1 | 3 |
| Patient 2- Tooth 11 |
| Pre-Op | 2.5 | 3 | 4 | 3 | 2 | 1 | 1 | 1 |
| Post-Op | 2 | 1 | 1 | 1 | 2 | 1 | 1 | 1 |
Pre-Op: Preoperative; Post-Op: Postoperative
Diode laser tip was used in a continuous sweeping motion to join all the bleeding spots. Gingival tissue ablation was also carried out in the region of left central incisor to create a suitable shallow tissue bed for resting the pontic, as well as providing space for placing two central incisors with matching inciso-gingival lengths [Table/Fig-7,8].
Gingivectomy and recontouring with laser.
Modified gingival position with respect to previous prosthesis.

Analgesics (Tab. Paracetamol 500 mg) and local application of analgesic (in the form of 8.7% wt/wt Choline Salicylate and 2% wt/wt Lidocaine based ointment were prescribed to be used as and when needed. No major postoperative complications like severe pain, recession, swelling, etc., were observed and the wound healing was achieved uneventfully without scar formation at two weeks [Table/Fig-9].
At two weeks post-healing of gingival tissue.

Impressions were re-made after one month, once adequate healing was achieved and new 3-unit prosthesis (zirconia with ceramic layering) was fabricated over aesthetic soft tissue contours [Table/Fig-10].
New prosthesis with improved aesthetics and gingival positions.

Overall, the outcome of the procedure provided a positive aesthetic result; marked improvement was observed in final gingival tissue settlement and health over the follow-up visits made at one week, 15 days, one month and three months, as perceived by the patient as well as the clinician.
Case 2
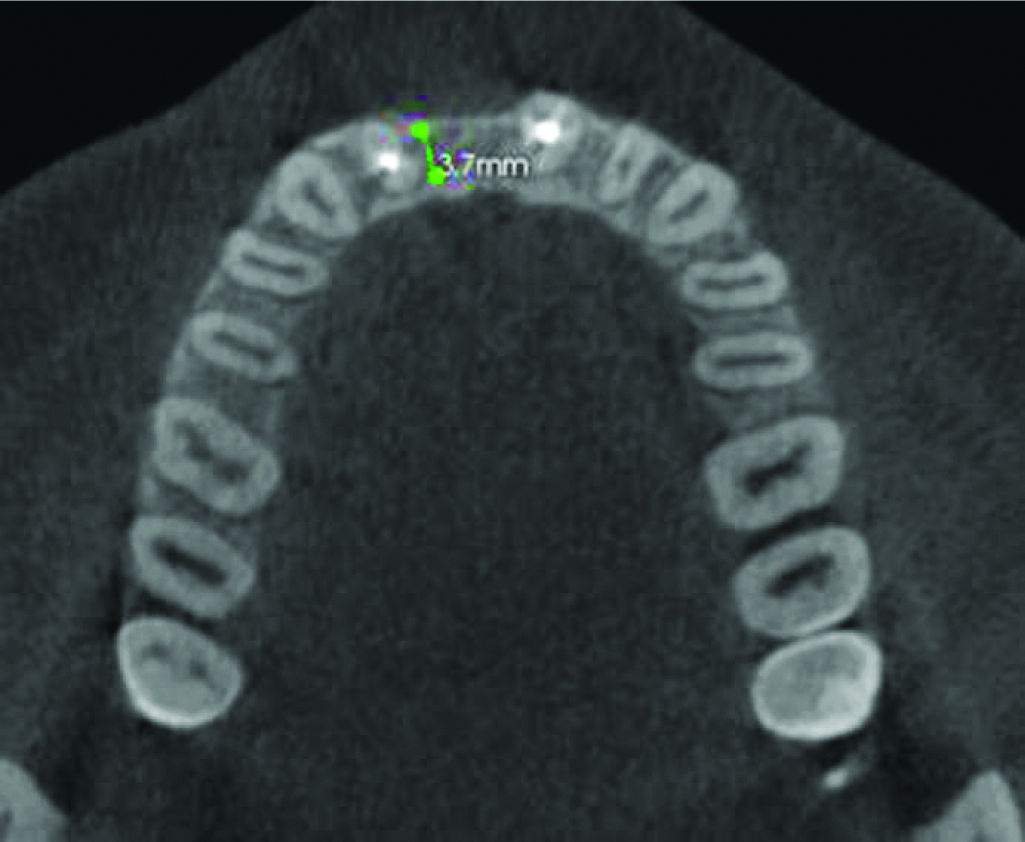
An 18-year-old female patient was referred for replacement of missing right maxillary central incisor i.e., 11, which she had lost subsequent to fall while playing eight years ago. Since the anterior tooth was missing for many years without any space maintainer or prosthesis, the mesio-distal space was lost and hence, orthodontic treatment was performed to gain the lost space. Medical history was not relevant and clinical examination showed missing 11; and root canal treated tooth i.e., 12 and 21 with no discoloration. Remaining occlusion was stable. Since CBCT revealed less width of available bone (3.7 mm), a narrow platform, (3.5×11.5 mm, Nobel Replace, with conical connection, Nobel Biocare India Pvt., Ltd.,) was placed by the oral surgeon.
As there was loss of labial bone post-trauma [Table/Fig-11], the eventual implant position came out to be more palatal than the ideal, leaving a thick gingival biotype labial to the implant, which was also more coronally placed as compared to adjacent central incisor [Table/Fig-12].
CBCT section showing bone anatomy with labial bone loss in case 2.
Gingival levels after second stage surgery of case 2.

Gingival biotype was evaluated using the transparency test [2]. Prosthetic crown was fabricated over models obtained, using conventional indirect implant level impression, and trial was done in patient’s mouth. The resultant position and outcome came out to be unsatisfactory concerning aesthetic expectations of the patient [Table/Fig-13].
Significant mismatch between crown height and gingival levels of implant supported crown.

Patient was explained about the reason and was given options of excision of soft tissue with blade or with laser. As the patient did not want an injectable anaesthesia, she opted for laser with topical anaesthetic application. Gingivectomy was performed in a similar manner as described above. The resultant change in the tissue level post gingivectomy was appreciable after healing [Table/Fig-6].
In this case, a layer of flowable composite was injected around the secondary healing cap [3] and stabilised with Coe-Pak to preserve the gingival contours and maintain emergence profile during the healing phase [Table/Fig-14]. An indirect implant level impression was remade post-adequate healing of three weeks after the laser therapy. A ceramic layered zirconia crown was fabricated and cemented over the abutment [Table/Fig-15].
Flowable composite around secondary healing abutment to maintain custom contours post gingivectomy.

Final prosthesis with improved aesthetics and dimensions.

Eventually, the gingival contours of both the central incisors were at a similar level, with appreciable improvement with regard to the patient’s initial presentation. Follow-up visits at one week, 15 days, one month revealed appropriate maturity of gingival levels with no formation of black triangles, recession, or inflammation. Patient was referred back to unit of orthodontics for completion of her treatment.
Consent was obtained from both patients for the images presented in the manuscript.
Discussion
In the last decade, soft tissue lasers like Carbon Dioxide (CO2), Nd:YAG, argon, holmium, and diode lasers; due to their numerous advantages, have effectively replaced conventional scalpel or electro surgery to perform soft tissue manipulation procedures like gingivectomy, gingival contouring, frenectomy, operculectomy, implant punch hole and exposure, gingival depigmentation, excision of reactive lesions of gingiva etc., [4].
Diode lasers have a wavelength ranging between 805-980 nm. At this wavelength, it is well absorbed by water and pigments like haemoglobin, melanin, etc. As a result, these lasers act on soft tissues like gingiva which contain such pigments, with minimal effect on hard tissues like tooth and implant surface as these are devoid of any such constituents [5]. The penetrative depth of diode lasers is approximately 2-6 mm into the soft tissue resulting in a superficial wound that heals faster with minimal scarring and oedema [6]. The longer wavelengths provide a lesser penetrative depth. This wavelength is also well absorbed by the pigment containing bacteria thus curtailing the overall bacterial load locally [7]. The heat generated by these lasers is taken up by the haemoglobin which seals off small blood vessels leading to a relatively bloodless and neat operating field [8].
A study performed by Neill ME revealed a mean score of 1.9 (between 0-10) with regard to pain experienced three hours after laser soft tissue procedure [9]. In various aspects, soft tissue lasers offer various advantages, like minimal bleeding, cleaner field of operation, better patient comfort over conventional means of a scalpel and/or electro surgery used for performing similar procedures; for the fact that they work in a minimal depth, evoking a suppressed inflammatory response from the body [4].
Several case reports have been published in the past using diode laser to perform soft tissue contouring procedures with precision [4-6]. In a study by Arora SA et al., clinical crown lengthening was performed using diode lasers leading for better healing of the operated site [5]. Shivaprasad BM et al., also conducted a study on correction of gummy smile using diode lasers and stated that such procedures can be carried out using diode lasers in a faster, more precise, and comfortable manner [4]. With respect to their use in implantology, El-Kholey KE compared use of diode lasers with conventional method of using a surgical blade for implant exposure. He concluded that diode lasers can be effectively used as an alternative to conventional techniques with added advantages like minimal need for local anaesthesia for the same [10]. In a review published by Gupta R et al., lasers were found to be gentler, less invasive, and less painful as compared to the traditional methods used in implantology for hard and soft tissue alterations [11]. Diode lasers along with Er:YAG lasers have shown to be effective, at a power of 2W, in removal of inflamed tissue and bacterial biofilm from the implant helping in the management of peri-implantitis [12].
However, there are diverse laser types with varying power settings, not all are suited for soft tissue dental use. A power setting of more than 8W has been reported to result in necrosis of superficial cellular layers, tooth sensitivity, gingival recession, and postoperative pain. Hence, it is advisable to use the lowest power setting that is able to perform the desired procedure in soft tissues [13].
Care must be taken while performing such lengthening procedures to leave at least 2 mm of keratinised attached gingiva around the implants, improving their overall prognosis and longevity [14]. Although, the cases provided above had missing maxillary anterior teeth as a resultant of trauma causing labial cortical bone loss; with adequate planning and care, the final soft tissue placement results can be replicated as closely as outlined and anticipated.
Conclusion(s)
Using diode lasers, desired gingival zenith and contours around implant supported prostheses can be achieved in a controlled and painless manner enhancing the aesthetics of anterior restorations.
[1]. Chu SJ, Tan JH, Stappert CF, Tarnow DP, Gingival zenith positions and levels of the maxillary anterior dentitionJ Esthet Restor Dent 2009 21(2):113-20.10.1111/j.1708-8240.2009.00242.x19368601 [Google Scholar] [CrossRef] [PubMed]
[2]. Kan JY, Rungcharassaeng K, Umezu K, Kois JC, Dimensions of peri-implant mucosa: An evaluation of maxillary anterior single implants in humansJ Periodontol 2003 74(4):557-62.10.1902/jop.2003.74.4.55712747463 [Google Scholar] [CrossRef] [PubMed]
[3]. Solow R, Contour correction for stock titanium healing abutmentsJ Prosthet Dent 2018 120(5):787-88.10.1016/j.prosdent.2017.12.01929961609 [Google Scholar] [CrossRef] [PubMed]
[4]. Shivaprasad BM, Rakesh MP, Prabhu SS, Esthetic correction of gummy smile by gingivectomy using diode laserJ Health Sci Res 2015 6(1):17-21.10.5005/jp-journals-10042-1013 [Google Scholar] [CrossRef]
[5]. Arora SA, Chhina S, Kazimm J, Goel A, Mishra S, Nidhi S, Clinical crown lengthening using soft tissue diode laser: A case seriesInt J Oral Health Med Res 2015 2(5):81-83. [Google Scholar]
[6]. Sobouti F, Rakhshan V, Chiniforush N, Khatami M, Effects of laser-assisted cosmetic smile lift gingivectomy on postoperative bleeding and pain in fixed orthodontic patients: A controlled clinical trialProg Orthod 2014 15(1):66.810.1186/s40510-014-0066-525487965 [Google Scholar] [CrossRef] [PubMed]
[7]. Harris DM, Yessik M, Therapeutic ratio quantifies laser antisepsis: ablation of Porphyromonas gingivalis with dental lasersLasers Surg Med 2004 35(3):206-13.10.1002/lsm.2008615389740 [Google Scholar] [CrossRef] [PubMed]
[8]. Wigdor HA, Walsh JT Jr, Featherstone JD, Visuri SR, Fried D, Waldvogel JL, Lasers in dentistryLasers Surg Med 1995 16(2):103-33.10.1002/lsm.19001602027769957 [Google Scholar] [CrossRef] [PubMed]
[9]. Neill ME, Sulcular debridement and bacterial reduction with the PulseMaster Dental Laser: Clinical evaluation of the effects of pulsed Nd:YAG laser on periodontitis and periodontal pathogensMS Thesis, University of Texas Graduate School of Biomedical Sciences at San Antonio 1997 [Google Scholar]
[10]. El-Kholey KE, Efficacy and safety of a diode laser in second-stage implant surgery: A comparative studyInt J Oral Maxillofac Surg 2014 43(5):633-38.10.1016/j.ijom.2013.10.00324210453 [Google Scholar] [CrossRef] [PubMed]
[11]. Gupta R, Luthra RP, Gupta S, Lasers in dental implantology: A reviewInt Dent Med J Adv Res 2016 2:01-04.10.15713/ins.idmjar.46 [Google Scholar] [CrossRef]
[12]. Nikitas A, Er:YAG and diode lasers in treatment of peri-implantitis- A case reportJournal of Clinical and Diagnostic Research 2019 13(1):ZD08-10.10.7860/JCDR/2019/36611.12465 [Google Scholar] [CrossRef]
[13]. Kurtzman GM, Mahesh L, Implant uncovery and soft-tissue modification utilizing a diode laserInt J Oral Implantol Clin Res 2015 6(1):20-25.10.5005/jp-journals-10012-1131 [Google Scholar] [CrossRef]
[14]. Berglundh T, Lindhe J, Dimension of the periimplant mucosa. Biological width revisitedJ Clin Periodontol 1996 23(10):971-73.10.1111/j.1600-051X.1996.tb00520.x8915028 [Google Scholar] [CrossRef] [PubMed]