Non-surgical Approach to Improve Prognosis of Ocular Prostheses for Grade III and IV Contracted Sockets
Neeti Solanki1, Saumyendra Singh2, Deeksha Arya3
1 Junior Resident, Department of Prosthodontics, Crown and Bridges, King George’s Medical University, Lucknow, Uttar Pradesh, India.
2 Professor, Department of Prosthodontics, Crown and Bridges, King George’s Medical University, Lucknow, Uttar Pradesh, India.
3 Additional Professor, Department of Prosthodontics, Crown and Bridges, King George’s Medical University, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Saumyendra Singh, 2/273, Viramkhand, Lucknow, Uttar Pradesh, India.
E-mail: saumyendravsingh@gmail.com
Patients with Grade III or IV contracted ocular sockets, most often due to Post Enucleation Socket Syndrome (PESS), suffer from loss of ocular volume along with a lax lower eyelid, which complicates prosthetic rehabilitation in terms of fit as well as aesthetics. Surgical correction is preferable, though not always feasible. A non-invasive approach for prosthetic rehabilitation of such difficult cases, using bandaging and progressively larger conformers is described here.
Bandaging, Conformer, Post enucleation socket syndrome, Reduced ocular volume
Introduction
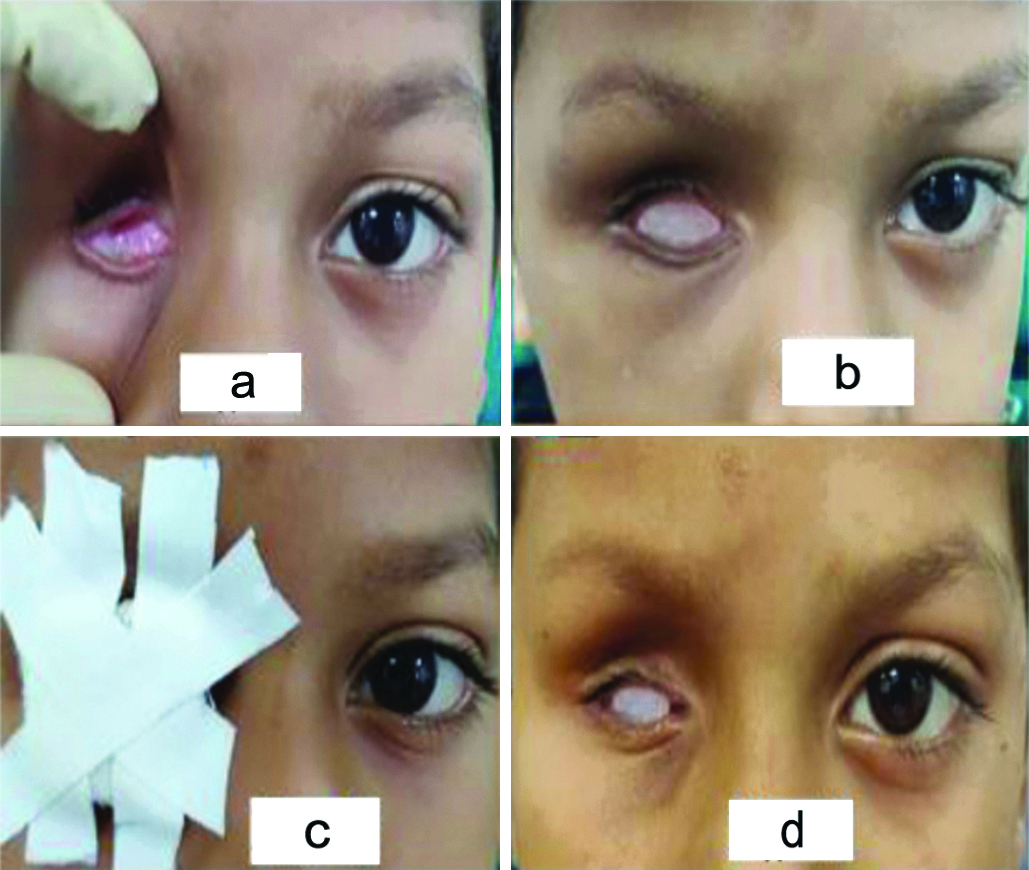
Prosthetic rehabilitation of an obliterated eye socket {mostly due to Post Enucleation Socket Syndrome (PESS)} [1], can prove to be quite a challenge for the maxillofacial prosthodontist owing to the reduced ocular prosthetic volume and shallow palpebral vestibules along with a lax lower lid [Table/Fig-1a] [2], which affects both fit and aesthetics [3]. In severe cases, it may be impossible to retain even an initial conformer without corrective surgery [Table/Fig-1b] [4,5]. A simple and effective approach using bandaging to enhance retention and aesthetic outcome of an ocular prosthesis is being described here. Bandage was used here to hold the prosthesis in place within the contracted socket so as to achieve the adequate attention. Patient consent was obtained for the use of images in the manuscript.
a: Grade III Constricted ocular socket. b: Conformer not retained in socket due to PESS. c: Conformer bandaged in place. d: Conformer retained in the socket with eyelids well-adapted over it.
Technique
Make an ocular impression, pour a model, fashion an ocular wax pattern, do a try in and dewax conventionally.
Keep the pattern overextended by 1 mm in all areas needing extension/enlargement. Keep the pattern contour as similar to normal counterpart as possible.
Fabricate an ocular conformer in heat cured acrylic. Finish and polish.
Bandage the conformer in proper position until the next follow-up, with the eyelids gently approximated, using gauze and surgical tape in a criss-cross manner [Table/Fig-1c].
This should maintain constant and mild force within the socket, without causing pain.
Instruct the patient not to remove the bandage himself and to keep the prosthesis in place till the next visit.
Schedule first follow-up appointment at three days, and subsequently at weekly intervals.
At each follow-up, evaluate the socket for increase in space, fit of conformer [Table/Fig-1d] and absence of inflammation.
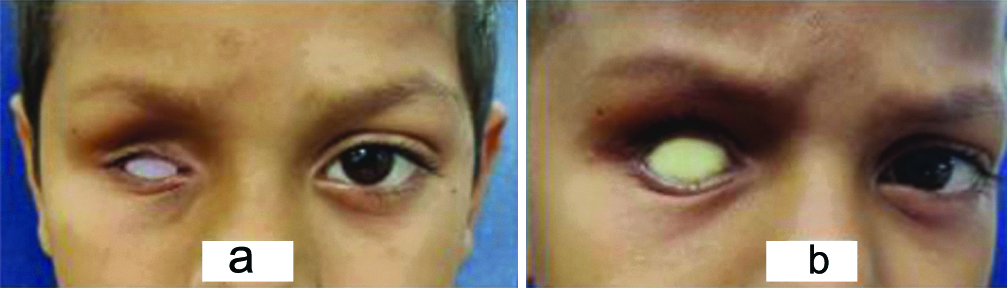
If all three of the above parameters are favourable, enlarge the conformer 1 mm with chair-side soft liner, bandage and continue follow-up. Continue this cycle till the desired conformer size is retained [Table/Fig-2a,b].
If at any appointment, any of the above mentioned parameters are unfavourable, continue with the same conformer without adjustment for a week, then re-evaluate.
If the soft liner becomes too bulky (after three or four appointments), make a new set of impressions, fabricate a conformer and continue as above.
Any inflammation and pain because of confinement of a slightly overextended conformer can be countered by a regular follow-up protocol.
Comparison of change in size of an initial conformer (a) with the final one (b).
The described non-invasive technique has proven to be a simple, inexpensive, viable option in increasing ocular socket volume for patients where surgery is not desirable, feasible or preferable [6]. In cases where initial conformer isn’t retained within the constricted socket, using bandaging and progressively enlarging the socket non-surgically has yielded favourable results. Decidedly, this approach cannot match the surgical alternative in speed and extent of correction. This approach needs patience on part of the treatment provider, and compliance from the patient. Experience is also needed in knowing where to arbitrarily enlarge the conformer. The described procedure shall become more predictable with time, as more patients are observed for longer time periods.
This technique provides a promising option for patients who were unable to wear any prosthesis because of PESS and were reticent to go for corrective surgery.
Conclusion(s)
Contracted ocular socket can be successfully rehabilitated non-invasively through gradual expansion by modifying the conventional prosthetic protocol. Bandaging serves as a medium to hold the prosthesis in place till optimum retention is achieved.
Author contributions: NS in Conceptualisation, investigation and writing original draft. Singh VS in conceptualisation, methodology, writing, reviewing and editing. Arya D in formal analysis, writing, reviewing and editing.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 07, 2020
Manual Googling: Dec 03, 2020
iThenticate Software: Jan 20, 2021 (9%)
[1]. Krishna G, Contracted sockets -I (Aetiology and types)Indian J Ophthalmol 1980 28(3):117-20. [Google Scholar]
[2]. Tyers AC, Collin JR, Orbital implants and post enucleation socket syndromeTrans Ophthalmol Soc UK 1982 102(Pt 1):90-92. [Google Scholar]
[3]. Aggarwal H, Singh SV, Kumar P, Kumar Singh A, Prosthetic rehabilitation following socket reconstruction with blair-brown graft and conformer therapy for management of severe post-enucleation socket syndrome-A clinical reportJ. Prosthodont 2015 24(4):329-33.10.1111/jopr.1222225231188 [Google Scholar] [CrossRef] [PubMed]
[4]. Mavrikakis I, Malhotra R, Shelley MJ, Sneddon KJ, Surgical management of the severely contracted socket following reconstructionOrbit 2006 25(3):215-19.10.1080/0167683060067138316987769 [Google Scholar] [CrossRef] [PubMed]
[5]. Tsur H, Kaplan H, Shafir R, Rosner M, Orenstein A, Rosen N, Repair of the severely contracted socket with meshed skin graft and semi-rigid conformerOphthal Surg 1991 22(5):269-73. [Google Scholar]
[6]. Jamayet N, Johari Y, Alam MK, Husein A, Expansion of a contracted eye socket by ocular prosthesis: An alternative prosthetic approach to correct the post enucleation socket syndromeOHDM 2015 14(3):136-39. [Google Scholar]