Pseudomonas Mendocina Wound Infection in a Farmer: A Rare Case
Varsha Gupta1, Lipika Singhal2, Kritika Pal3, Ashok Attri4, Jagdish Chander5
1 Professor, Department of Microbiology, Government Medical College and Hospital, Chandigarh, India.
2 Assistant Professor, Department of Microbiology, Government Medical College and Hospital, Chandigarh, India.
3 Demonstrator, Department of Microbiology, Government Medical College and Hospital, Chandigarh, India.
4 Professor, Department of General Surgery, Government Medical College and Hospital, Chandigarh, India.
5 Professor, Department of Microbiology, Government Medical College and Hospital, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kritika Pal, Government Medical College, Sector-32, Chandigarh, India.
E-mail: drkritika4390@gmail.com
The members of the family Pseudomonadaceae have been reorganised under various groups, each with several species and are known as opportunistic pathogens. Pseudomonas mendocina (P.mendocina) formerly known as CDC group Vb-2, belongs to stutzeri group (group II) and was first discovered in 1970 in Mendoza. The present case report is about an overwhelming leg ulcer in an asthmatic and diabetic 53-year-old, Indian farmer following a fall due to a multi-drug resistant strain of P.mendocina without any systemic spread due to timely intervention. Authors emphasise that P. mendocina may be an important emerging pseudomonad or alternatively an under-diagnosed pathogen in immunocompromised patients exposed to soil. The multidrug resistant nature of this organism is alarming and it may become a threat to people with weakened immune systems.
Immunocompetent, Immunocompromised, Overwhelming leg ulcers
Case Report
A 53-year-old male, farmer by occupation, presented with an ulcer on right leg below the knee [Table/Fig-1] since 15 days, following a fall (informed consent was obtained from the patient for publication of any images). The ulcer which started as a small wound was rapidly progressive in nature and was associated with pain and oedema of the surrounding area. It was associated with fever, pedal oedema and pus discharge for 4-5 days before approaching to hospital. He complaint of severe leg pain and difficulty in walking. His relevant medical history included bronchial asthma since last 25 years, with seasonal exacerbations, which was controlled with Metered dose Inhaler (Budesonide 200 mcg). The patient was also diagnosed with Type II diabetes mellitus in 2018 and was put on Metformin 500 mg BD. He was a reformed smoker and a social drinker, smoking about 1-2 bundles of cigarette per day for the last 30 years. The patient had a history of taking corticosteroids for acute exacerbations of bronchial asthma on and off. The pus collected from the ulcer was sent for culture and sensitivity. On Gram stain, gram-negative bacilli with plenty of pus cells were seen [Table/Fig-2].
Overwhelming leg ulcer caused by Pseudomonas mendocina.

Gram stain showing gram-negative bacilli (black arrow) (10X).

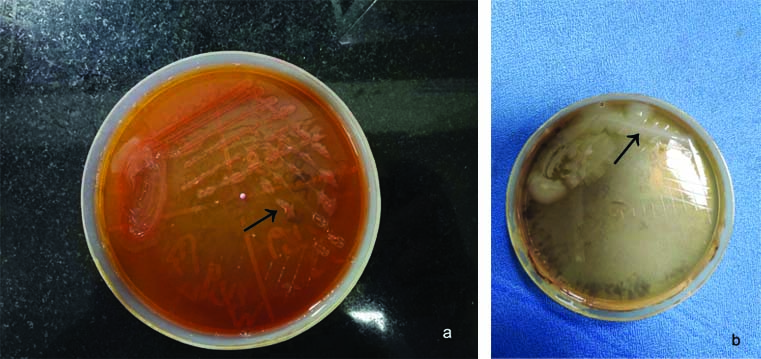
Pus was inoculated on 5% Sheep blood agar and MacConkey agar medium. After overnight incubation at 37°C, a confluent growth of non-haemolytic colonies was observed on blood agar medium. On MacConkey agar, lactose non-fermenting colonies [Table/Fig-3a] grew which was oxidase and nitrate reduction positive. The isolate was identified as a non-pigmented Pseudomonas species on Nutrient Agar [Table/Fig-3b] and based on biochemical tests. A repeat pus sample was collected three days after first sample that also grew the same organism. Subsequently, the identification of the isolate was done using Matrix Assisted Laser Desorption Ionisation-Time Of Flight Mass Spectrometry (MALDI-TOF MS, Bruker Daltonics, Germany). Spectra were analysed using MALDI Biotyper 3, and the isolate was identified as Pseudomonas mendocina with a high score of 2.0.
a) MacConkey agar showing lactose non-fermenting flat irregular colonies (black arrow); b) Nutrient agar showing non-pigmented Pseudomonas colonies (black arrow).
Due to overwhelming wound site infection, blood was also cultured but was found to be sterile. The antimicrobial susceptibility profile of the isolate was determined using Kirby bauer disk diffusion method as per CLSI 2019 guidelines [1] and it was found to be resistant to the anti-pseudomonal antibiotics like ciprofloxacin, ceftazidime, amikacin, pipercillin-tazobactum and aztreonam and was found to be susceptible only to colistin with Minimum Inhibitory Concentration (MIC) 1 μg/mL. The patient was started on empiricial therapy with beta lactam and beta lactamases inhibitor with aminoglycoside (Amoxicillin-clavulanic acid 500 mg tds and gentamicin 5 mg/kg tds). Surgical debridement of the wound was done. After the culture report, the patient was put on Anti-pseudomonal treatment i.e., Meropenem 500 mg IV q8hr in combination with gentamicin 5 mg/kg IV qhr for 10 days. The patient was discharged after 10 days and was put on ciprofloxacin 500 mg q12 hour for seven days. Betadine dressings were done for 15 days as per the standard protocol for treating leg wounds, to which the patient slowly responded. The patient came for regular follow-up for dressings and the wound significantly decreased in size over a period of 2-3 weeks. Although the patient responded to the treatment, but he later on experienced maggot infestation due to unhygienic conditions, for which turpentine oil was used. Later on the patient was lost to follow-up.
Discussion
The members of the family Pseudomonadaceae have been reorganised under various groups, each with several species and are known as opportunistic pathogens. Pseudomonas mendocina (formerly CDC group Vb-2) belongs to stutzeri group (group II) and was first discovered in 1970 in Mendoza, Argentina and was presumed to be non-pathogenic in humans [2]. The preliminary studies revealed it to be a soil de-nitrifier [2-4]. In nature, P.mendocina has been isolated from water and soil and is documented to be able to survive on over 75 different substrates, growing at temperatures ranging from 25°C to 42°C [2].
A research in 1992 revealed that the first case of infection in humans by P. mendocina was reported in a 63-year-old man with infective endocarditis in Argentina [2]. Until now, very few cases of infection by P.mendocina have been reported in immunocompromised as well as immunocompetent patients following suspected prolonged exposure to the bacteria.
P.mendocina is an opportunistic pathogen with low virulence potential. P.mendocina is a rare source of bacterial infection in humans. There have been 14 reported cases of P. mendocina in the world [2]. Six of these cases were reported from South East Asian region [Table/Fig-4] [2,3,5-13].
Various studies showing Pseudomonas mendocina as pathogen [2,3,5-13].
| S. No. | Author, publication year | Age (years)/Gender | Location | Diagnosis | Type of infection | Patient outcome |
|---|
| 1. | Gani M et al., 2019 [2] | 64/M | USA | Bacteremia | Mono | Survived |
| 2. | Huang CR et al., 2018 [5] | 55/M | Taiwan | Meningitis | Mono | Survived |
| 3. | Huang CR et al., 2018 [5] | 66/F | Taiwan | Meningitis | Mono | Survived |
| 4. | Huang CR et al., 2018 [5] | 79/M | Taiwan | Meningitis | Poly-Aeromonas caviae | Survived |
| 5. | Huang CR et al., 2018 [5] | 78/F | Taiwan | Meningitis | Poly-Acinetobacter | Survived |
| 6. | Chi CY et al, 2005 [6] | 65/M | Taiwan | Spondylodiscitis | Mono | Survived |
| 7. | Aragone MR et al., 1992 [3] | 63/M | Argentina | Native mitral valve endocarditis | Mono | Survived |
| 8. | Chiu LQ and Wang W, 2013 [7] | 34/M | Singapore | Foot wound infection | Poly-Stenotrophomonas maltophilia | Survived |
| 9. | Rapsinski GJ et al., 2016 [8] | 57/M | USA | Native mitral valve endocarditis | Mono | Survived |
| 10. | Suel P et al, 2011 [9] | 79/F | France | Native aortic valve endocarditis | Mono | Survived |
| 11. | Jeronimo TM et al., 2017 [10] | 22/M | Portugal | Peritonitis | Mono | Survived |
| 12. | Johansen HK et al, 2001 [11] | 28/F | Denmark | Native tricuspid valve endocarditis | Mono | Survived |
| 13. | Mert A et al., 2007 [12] | 36/M | Turkey | Native mitral valve endocarditis | Mono | Survived |
| 14. | Nseir W et al., 2011 [13] | 31/M | Israel | Bacteremia | Mono | Survived |
| 15. | Present case, Gupta V et al., 2021 | 53/M | India | Leg wound infection | Mono | Survived |
This was the first from Indian subcontinent. Most of the cases have been reported from Taiwan [5,6] and only one case has been reported from Singapore [3,7]. In all the cases the patients were severely immunocompromised and had underlying condition making them susceptible to the infection. To the best of our knowledge we have reported the first report of mono-microbial wound infection with P.mendocina without systemic involvement. This is in contrast to previously reported wound infections [14]. None of the cases of human P.mendocina infection could provide any information regarding the source of infection. In the present case, the patient gave history of fall in his farm while working and developed a wound on leg. We propose that P.mendocina being present in soil and water could have gained entry into the wound. Being an immunocompromised individual due to diabetes, and prolong history of bronchial asthma with intermittent corticosteroid treatment the patient developed an overwhelming infection. However, the exact source of infection could not be traced because of the lack of environmental surveillance.
Also being an uncommon clinical pathogen not much data is available about P.mendocina antibiotic susceptibility pattern. Being closely related to Pseudomonasstutzeri and likewise it is also expected to be susceptible to most antibiotics. However, in this study, the isolate was multidrug resistant which was in contrast to most of the studies [8,9].
Conclusion(s)
This was a case of an overwhelming leg ulcer in an asthmatic and diabetic Indian farmer following a fall due to a multidrug resistant strain of P.mendocina without any systemic spread due to timely intervention. P.mendocina may be considered as an important emerging non-Pseudomonasaeruginosa pseudomonad or alternatively an under-diagnosed pathogen in immunocompromised patients exposed to soil. It is pertinent to accurately identify the bacterium owing to the multidrug resistant nature of this organism which is alarming and it may become threat to people with weakened immune systems.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 25, 2020
Manual Googling: Oct 14, 2020
iThenticate Software: Jan 18, 2021 (7%)
[1]. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing: Twenty-third informational supplement. Clinical and Laboratory Standards Institute. CLSI document M100-S29. Wayne, PA, USA (2019) [Google Scholar]
[2]. Gani M, Rao S, Miller M, Scoular S, Pseudomonas mendocina bacteremia: A case study and review of literatureAm J Case Rep 2019 20:453-58.10.12659/AJCR.91436030948701 [Google Scholar] [CrossRef] [PubMed]
[3]. Aragone MR, Maurizi DM, Clara LO, Estrada JLN, Ascione A, Pseudomonas mendocina, an environmental bacterium isolated from a patient with human infective endocarditisJ Clin Microbiol 1992 30(6):1583-84.10.1128/JCM.30.6.1583-1584.19921624580 [Google Scholar] [CrossRef] [PubMed]
[4]. Palleroni NJ, Doudoroff M, Stanier RY, Solánes RE, Mandel M, Taxonomy of the aerobic pseudomonads: The properties of the Pseudomonas stutzeri groupJ Gen Microbiol 1970 60(2):215-31.10.1099/00221287-60-2-2155488055 [Google Scholar] [CrossRef] [PubMed]
[5]. Huang CR, Lien CY, Tsai WC, Lai WA, Hsu CW, Tsai NW, The clinical characteristics of adult bacterial meningitis caused by non-Pseudomonas (Ps.) aeruginosa Pseudomonas species: A clinical comparison with Ps. aeruginosa meningitisKaohsiung J Med Sci 2018 34(1):49-55.10.1016/j.kjms.2017.08.00729310816 [Google Scholar] [CrossRef] [PubMed]
[6]. Chi CY, Lai CH, Fung CP, Wang JH, Pseudomonas mendocina spondylodiscitis: A case report and literature reviewScand J Infect Dis 2005 37(11-12):950-53.10.1080/0036554050026317716308244 [Google Scholar] [CrossRef] [PubMed]
[7]. Chiu LQ, Wang W, A case of unusual Gram-negative bacilli septic arthritis in an immunocompetent patientSingapore Med J 2013 54(8):164-68.10.11622/smedj.201316224005465 [Google Scholar] [CrossRef] [PubMed]
[8]. Rapsinski GJ, Makadia J, Bhanot N, Mi Z, Pseudomonas mendocina native valve infective endocarditis: A case reportJ Med Case Rep 2016 10(1):27510.1186/s13256-016-1057-627716406 [Google Scholar] [CrossRef] [PubMed]
[9]. Suel P, Martin P, Berthelot G, Robaday S, Etienne M, Chibani A, A case of Pseudomonas mendocina endocarditisMed Mal Infect 2011 41(2):109-10.10.1016/j.medmal.2010.09.00921094007 [Google Scholar] [CrossRef] [PubMed]
[10]. Jerónimo TM, Guedes AM, Stieglmair S, Guerreiro R, Laranjo C, Bernardo I, Pseudomonas mendocina: The first case of peritonitis on peritoneal dialysisNefrologia 2017 37(6):647-49.10.1016/j.nefro.2016.11.00428655401 [Google Scholar] [CrossRef] [PubMed]
[11]. Johansen HK, Kjeldsen K, Høiby N, Pseudomonas mendocina as a cause of chronic infective endocarditis in a patient with situs inversusClin Microbiol Infect 2001 7(11):650-52.10.1046/j.1198-743x.2001.00331.x11737094 [Google Scholar] [CrossRef] [PubMed]
[12]. Mert A, Yilmaz M, Ozaras R, Kocak F, Dagsali S, Native valve endocarditis due to Pseudomonas mendocina in a patient with mental retardation and a review of literatureScand J Infect Dis 2007 39(6-7):615-16.10.1080/0036554060107188317577828 [Google Scholar] [CrossRef] [PubMed]
[13]. Nseir W, Taha H, Abid A, Khateeb J, Pseudomonas mendocina sepsis in a healthy manIsr Med Assoc J 2011 13(6):375-76. [Google Scholar]
[14]. Kiryszewska A, Szczerba I, Grzegorczyk JL, Gaszyński W, Pseudomonas mendocina as an agent of bacteremia, case study and literature reviewJ Clin Case Rep 2015 5:59810.4172/2165-7920.1000598 [Google Scholar] [CrossRef]