According to new definition of dry eye by Dry Eye Work Shop (DEWS II) “It is a multifactorial disease of precorneal tear film characterised by decreased homeostasis of the tear film, including the ocular symptoms, in which along with instability and hyperosmolarity of tear film, inflammation and neurosensory defect are also included” [1]. Tear film disorder due to tear deficiency or tear evaporation damages ocular surface which causes ocular discomfort [2]. Cataract and retinopathy are well known ocular complications in diabetes since ages. Recently, attention has been drawn towards its association with dry eyes and ocular surface problems. Tear film abnormality is the salient feature of the diabetic ocular surface disease which is due to poor quality and function of tear along with subnormal ocular surface. The global prevalence of DED ranging from 5% to 35% is greatly influenced by geographic location, climatic condition and life style of the people [1,3,4]. Prevalence of DR in diabetic patients in India is approximately 21.27% [5]. DED is more commonly seen in ageing females, disease of ocular adnexa, systemic conditions like diabetics, thyroid disease, arthritis, hypertension, connective tissue disorders, several systemic and topical drugs [6,7].
Various pathophysiological mechanisms have been proposed for DED in diabetics which includes hyperglycaemia, advanced glycated end product accumulation, oxidative stress and upregulation of inflammatory mediators. Research shows “autonomic neuropathy” affecting the nerves that control the lacrimal gland [8], leads to aqueous deficient dry eye in diabetes. Evaporative dry eye due to inflammation in hyperglycaemic condition is also an accepted cause of DED in India [9]. People with DED often report with visual disturbances such as foggy vision, fluctuating vision and glare; often in spite of normal visual acuity using standard testing technique [10,11].
DED in diabetics can lead to variety of complication including superior punctate keratopathy, persistent epithelial defect, trophic ulceration which may lead to vision deficit, scarring and perforation of cornea and ultimately blindness. Moreover, patient with DR do not complaint of dry eye due to autonomic dysfunction but they have clinicopathological signs of kerotoconjunctivitis sicca. DR and DED appear to have common association. Hence, dry eye evaluation should be an integral part of routine ocular examination in the diabetics and diagnosing and managing it at the earliest. Except for a few studies done in New Delhi and Jammu, very few studies in India have stated association between dry eye and DR [12].
This study aims at evaluating the tear film dysfunction in diabetic patients with DR comparing to those without DR.
Materials and Methods
The present observational cross-sectional study was conducted in the Department of Ophthalmology, in a Tertiary Care Hospital, Vadodara, Gujarat, India from December 2017 to September 2019, after getting clearance from Institutional Ethics Committee (SSVIEC/ON/MEDI/BNPG16/D17173) in accordance with guidelines of the Declaration of Helsinki. Total of 103 patients (206 eyes) diagnosed with type ll diabetes, aged 40-80 years, consenting for the study were included.
All patients with pre-existing tear film dysfunction, ocular surface disorders, glaucoma and uveitis and having history of rheumatic arthritis and other connective tissue disorder were excluded. Patients on topical and systemic medication causing dry eye were also excluded.
Routine data including age, sex and duration of diabetes were obtained and all the patients underwent routine ophthalmic checkup including Best Corrected Visual Acuity (BCVA), Slit lamp examination, Tonometry and Fundus examination.
Posterior segment evaluation was done by indirect ophthalmoscopy and grading of DR was done according to Early Treatment in Diabetic Retinopathy Study (ETDRS) [13].
HbA1c was done along with routine diabetic investigations. Grading of dry eyes was based on OSDI questionnaire [10] and was confirmed by TBUT and Schirmer I and II test.
OSDI includes 12 questions divided in 3 parts i.e.,
Symptoms related to disturbance in vision
Symptoms related to function of vision
Symptoms related to external factors
Each question can be given a maximum score of 4 based on which a total score was calculated. Final score was obtained using a specific equation. Grading was considered as normal if the value was 0-12, 13-22 was considered as mild grade, 23-32 was considered as moderate grade and 33-100 was considered as severe grade.
Schirmer’s Test I
Reflex as well as basal tear secretion was measured by this test. Schirmer strip (Whatman filter paper No. 41) was placed at the junction of medial 2/3rd and lateral 1/3rd fornix of the lower lid, away from the cornea with the eyes closed. Closing of eyes was not necessary for this test, however it was found to give more accurate results as opposed to open eyes. The wetting of the tear strip was evaluated after 5 minutes. A value of less than 10 mm was considered abnormal.
Schirmer’s Test II
In this test topical proparacaine (0.5%) eye drops were instilled. Similar procedure was done according to Schirmer I test, wetting of tear strip was checked after 5 minutes and a value less than 10 mm was considered abnormal. Only the basal secretion was tested in this method and was found to be more reliable than Schirmer I.
Tear film Break Up Time (TBUT)
Fluorescein strip after putting a drop of saline was applied on ocular surface and patient was asked to blink 3-4 times. Under the Cobalt blue filter appearance of the first dry spot after the last blink in seconds gives the value. Grading can be done as >10 seconds is considered normal. A 5-10 seconds is considered mild to moderate dry eye and <5 seconds is considered severe.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS) version 20 was used for statistical analysis of this study data. All quantitative data were analysed by using parametric test whereas all qualitative data were analysed by using non-parametric test to find significance level and the p-value <0.05 was considered significant.
Results
In present study, 103 diabetic patients were evaluated for dry eyes and DR, out of which 46 were female and 57 were male. Out of 46 diabetic female patients 28 (60.9%) had dry eyes and out of 57 male patients 33 patients (57.9%) were diagnosed with dry eyes. It was not statistically significant (p=0.841) [Table/Fig-1].
Comparison of demographic variables and dry eye.
| Demographic variables | No Dry eye | Dry eye | Total | p-value |
|---|
| Gender | Female | 18 (39.1%) | 28 (60.9%) | 46 (100%) | 0.841 |
| Male | 24 (42.1%) | 33 (57.9%) | 57 (100%) |
| Age* (years) | 41-50 | 15 (46.9%) | 17 (53.1%) | 32 (100%) | 0.244 |
| 51-60 | 17 (42.5%) | 23 (57.5%) | 40 (100%) |
| >60 | 10 (32.3%) | 21 (67.7%) | 31 (100%) |
| Duration of diabetic (years) | 1-5 | 24 (41.4%) | 34 (58.6%) | 58 (100%) | 0.999 |
| 6-10 | 12 (40%) | 18 (60%) | 30 (100%) |
| 11-15 | 4 (40%) | 6 (60%) | 10 (100%) |
| >15 | 2 (40%) | 3 (60%) | 5 (100%) |
*Total of 61 (59.2%) were diagnosed with dry eyes; However, p-value was not statistically significant
In the age group of 41-50 years, 15 patients had normal tear film and 17 patients had dry eyes. In the age group of 51-60 years, 17 patients had normal tear film while 23 patients had dry eyes. In the age group of more than 60 years, 10 patients had normal tear film while 21 patients had dry eyes. So, a total of 42 patients had normal tear film and 61 were diagnosed with dry eyes. However, it was not statistically significant (p=0.244) [Table/Fig-1].
Based on duration of diabetes, there were 34, 18, 6 and 3 patients with dry eyes in 1-5 years, 6-10 years, 11-15 years and more than 15 years groups, respectively. Patients with normal tear film were 24, 12, 4 and 2 in 1-5 years, 6-10 years, 11-15 years and more than 15 years, respectively. It was not found to be statistically significant. (p=0.999) [Table/Fig-1].
On the basis of OSDI scoring, out of 103 diabetic patients, 38 patients had DR, in which 8 (18.6%) patients had mild dry eye, 13 (30.2%) patients had moderate dry eye and 17 (39.6%) had severe dry eye. While 60 patients had no DR, in which 30 (50%) patients had normal tear film, 15 (25%) patients had mild dry eye, 6 (10%) patients had moderate dry eye and 9 (15%) had severe dry eye. So, total of 38 (88.4%) DR patients were diagnosed as dry eye while, 30 (50%) patients with no DR were diagnosed with dry eye. The difference among the groups was statistically significant p=0.002 [Table/Fig-2].
| Impression | OSDI | Total | p-value |
|---|
| Normal | Mild | Moderate | Severe |
|---|
| DR | 5 (11.6%) | 8 (18.6%) | 13 (30.2%) | 17 (39.6%) | 43 (100%) | 0.002 |
| No DR | 30 (50%) | 15 (25%) | 6 (10%) | 9 (15%) | 60 (100%) |
| Total | 35 (34%) | 23 (22.4%) | 19 (18.4%) | 26 (25.2%) | 103 (100%) |
Out of 43 diabetic patients with DR, 38 patients had dry eye. In contrast, 60 diabetic patients without DR, 30 patients had dry eye. The difference among the groups was statistically significant p=0.002
In a total of 103 patients, 43 patients had DR and 60 patients had no DR changes, out of which 7 patients (16.3%) had normal tear film and 36 patients (83.7%) had dry eyes on basis of Schirmer’s I. While out of 60 patients with no DR changes, 38 patients (63.3%) had normal tear film and 22 patients (36.7%) had dry eyes. It was found to be statistically significant with a p-value=0.0001 [Table/Fig-3]. On basis of Schirmer’s II, 4 patients (9.3%) had normal tear film and 39 patients (90.7%) with DR changes had dry eyes. In patients with no DR changes, 37 patients (61.7%) had normal tear film and 23 patients (38.3%) had dry eyes. It was found to be statistically significant with a p-value=0.0001 [Table/Fig-3].
Schirmer I and II and dry eye.
| Impression | Sch I No dry eye | Sch I dry eye | Total | p-value | Sch II No dry eye | Sch II dry eye | Total | p-value |
|---|
| DR | 7 (16.3%) | 36 (83.7%) | 43 (100%) | 0.0001 | 4 (9.3%) | 39 (90.7%) | 43 (100%) | 0.0001 |
| No DR | 38 (63.3%) | 22 (36.7%) | 60 (100%) | 37 (61.7%) | 23 (38.3%) | 60 (100%) |
| Total | 45 (43.7%) | 58 (56.3%) | 103 (100%) | 41 (39.8%) | 62 (60.2%) | 103 (100%) |
Sch: Schirmer’s test; DR: Diabetic retinopathy; Prevalence of dry eyes in Diabetic patients was 56.3% i.e., 58 diabetics out of 103 on basis of Sch I; Prevalence of dry eye in diabetic patient was 60.2% based on Sch II. It was found to be statistically significant
When TBUT of 103 diabetic patients were performed, 15 patients (34.9%) had normal tear film, 22 patients (51.1%) had mild-moderate dry eye and 6 patients (14%) had severe dry eyes in patients with DR changes. While in patients with no DR changes 27 patients (45%) had normal tear film, 32 patients (53.3%) had mild-moderate and 1 patient (1.7%) had severe dry eyes. It was statistically significant with a p-value=0.046 [Table/Fig-4].
Tear film break up time and dry eye.
| Impression | TBUT |
|---|
| Normal | Mild to moderate | Severe | Total | p-value |
|---|
| DR | 15 | 22 | 6 | 43 | 0.046* |
| 34.9% | 51.1% | 14% | 100% |
| No DR | 27 | 32 | 1 | 60 |
| 45% | 53.3% | 1.7% | 100% |
| Total | 42 | 54 | 7 | 103 |
| 40.8% | 52.4% | 6.8% | 100% |
*Statistically significant with a p-value=0.046. Thus, prevalence of dry eye on basis of TBUT was 59.2%.
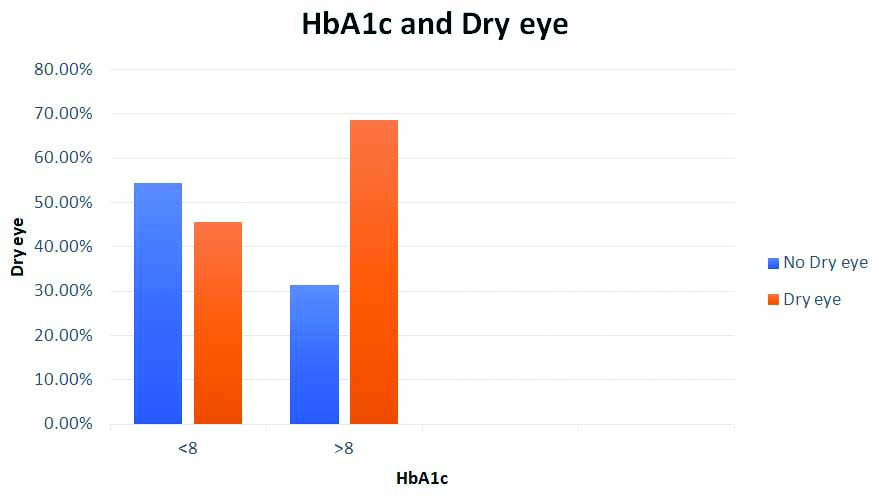
HbA1c <8% was observed in 55 patients out of which 25 patients (45.5%) had dry eyes, while 48 patients had ≥8% HbA1c, out of which 33 (68.7%) had dry eye. An increase is seen in the dry eyes incidence with higher HbA1c values but the results were not statistically significant (p=0.059) [Table/Fig-5].
Comparison of HbA1c and dry eye.
An increase is seen in the dry eyes incidence with higher HbA1c values but the results are not statistically significant (p=0.059)
Discussion
Tear film dysfunction in patients with type 2 Diabetes Mellitus is a common entity with complaints like grittiness, foreign body sensation, redness and watering. The prevalence of dry eyes in diabetes is as high as 15 to 54% [14]. In present study, the prevalence of dry eye in diabetic patients was 66% on basis of OSDI score [Table/Fig-2].
In present study, out of 103 diabetic patients, 46 (44.66%) were females and 57 (55.34%) were males having almost equal number of males and females, with no statistical significance (p-value= 0.691). Among 46 females, 28 (60.9%) had dry eyes and among 57 males, 33 (57.9%) had dry eyes (p=0.841) [Table/Fig-1].
In a study by Seifart U and Strempel I “prevalence of dry eyes in patients with 65 years and over in diabetics was 15-33% and increases with age and was 50% more commoner in females” [15]. Present study shows increasing trend of dry eyes in diabetics with increase in age. Prevalence of dry eye is 67.7% in the patients more than 60 years of age, but was not statistically significant (p=0.244) [Table/Fig-1].
The comparison of duration of diabetes with dry eyes was done where almost 60% patients had dry eyes in >5 years of diabetes, but was not statistically significant owing to limited number of patients in the study (p=0.999) [Table/Fig-1]. A study by Manaviat MR et al., stated that dry eye syndrome was more frequent in diabetic patients as compared to the control group with statistically significant result with (p=0.01). It was documented in this study that dry eyes incidence increases with increase in duration of diabetes [16].
OSDI scoring was performed in patients who were included in the study and was compared between the no DR group and the DR group. Out of total number of 43 DR patients, 17 patients (39.6%) had severe grading based on OSDI whereas only 9 patients (15%) out of 60 patients in the no DR group had severe grading and this was a significant addition to the result of our study (p=0.002) [Table/Fig-2]. On the basis of the result, it can be suggested that severity of dry eyes is relatively more in DR patients than those without DR. To best of authors knowledge, very few studies have been conducted showing relation between OSDI scoring and DR. Further studies can be carried out to authenticate this result. Yazdani-Ibn-Taz MK et al., it was stated that “OSDI scores in dry eye patients were significantly higher in type 2 diabetes (p=0.001) and type 1 diabetes (p=0.03), compared to non-diabetic patients.” The results obtained were comparable to present study [17].
A significant association between Schirmer I and II test values and the presence of DR with a p-value=0.0001 was seen in both the comparison tables [Table/Fig-3]. Dry eye as measured by Schirmer I and II tests was present in 83.7% and 90.7% patients who were diagnosed with DR and it was 36.7% and 38.3% in patients without DR. Similarly, a positive association was found between the grading of dry eye based on TBUT and presence of DR with p-value=0.046 [Table/Fig-4]. In Kesarwani D et al., study “Diabetic patients showed significantly reduced Schirmer, TBUT measurements as compared to control group (p<0.001)” [8]. However, in a study by Li HY et al., “111 type 2 diabetes patients and 100 control subjects were taken. Patients with type 2 diabetes showed higher dry eye score, higher TBUT values as compared to the control patients but the value of Schirmer I test were equal in both the groups 10.61±6.86 s in diabetic group, 10.92±7.05 s in control group, p>0.05” [18]. Unlike present study, this above mentioned study did not find statistical difference in Schirmer 1 test in diabetic and control group. Very few studies have taken into account Schirmer 2 in comparison to DR. In a study by Khurana G had similar results which stated that positive correlation was found between Schrimer II test and presence of DR (p<0.0001) [12].
In present study, an increase in the incidence of dry eyes was found with increased levels of HbA1c. In total of 55 patients who had HbA1c <8, only 25 patients (45.5%) had dry eye, whereas in 48 patients with HbA1c more >8, 33 patients (68.7%) had dry eye. However, it was not statistically significant (p=0.059) [Table/Fig-5]. Zhang X et al., Zou X et al., studies results matched with the results of present study [14,19].
Limitation(s)
A limited number of cases in both groups may have affected the results in the study. Few important objective tests like corneal staining, conjunctival impression and cytology, tear osmolarity measurements could have given a better insight in correlating the prevalence of dry eyes to that of severity of DR. Corneal sensation was not assessed, which may have given more insight to present study.
Conclusion(s)
Present study states that the prevalence of dry eyes was more in DR patients, which can be due to mechanisms like oxidative stress and inflammation as mentioned earlier. Progressive damage to corneal nerves due to neuropathy in diabetes can lead to impaired corneal sensation and dry eye which correlates with the severity of DR. This shows that tear film quality is affected by the presence of DR. The results obtained by comparison between OSDI, Schirmer test and TBUT and DR also proves that tear film quantity is decreased in patients with DR. Dry eye screening should be done routinely in all diabetic patients so that proper management can be done. Diabetic patients with poor metabolic glycaemic control as measured by HbA1c levels are more likely to be diagnosed with DED. Yet a number of factors causing dry eyes in diabetic patients remain to be evaluated in greater depths in future studies.
*Total of 61 (59.2%) were diagnosed with dry eyes; However, p-value was not statistically significant
Out of 43 diabetic patients with DR, 38 patients had dry eye. In contrast, 60 diabetic patients without DR, 30 patients had dry eye. The difference among the groups was statistically significant p=0.002
Sch: Schirmer’s test; DR: Diabetic retinopathy; Prevalence of dry eyes in Diabetic patients was 56.3% i.e., 58 diabetics out of 103 on basis of Sch I; Prevalence of dry eye in diabetic patient was 60.2% based on Sch II. It was found to be statistically significant
*Statistically significant with a p-value=0.046. Thus, prevalence of dry eye on basis of TBUT was 59.2%.