Pleomorphic Adenoma Arising from Heterotopic Salivary Gland Tissue in the Submandibular Region
Toshinori Iwai1, Satomi Sugiyama2, Hiroaki Kitajima3, Makoto Hirota4, Kenji Mitsudo5
1 Assistant Professor, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
2 Clinical Fellow, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
3 Clinical Fellow, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
4 Associate Professor, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Medical Center, Yokohama, Kanagawa, Japan.
5 Professor, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Toshinori Iwai, 3-9 Fukuura Kanazawa-ku, Yokohama, Kanagawa, Japan.
E-mail: iwai104oams@yahoo.co.jp
Benign tumour, Chondroid, Myoepithelial, Painless
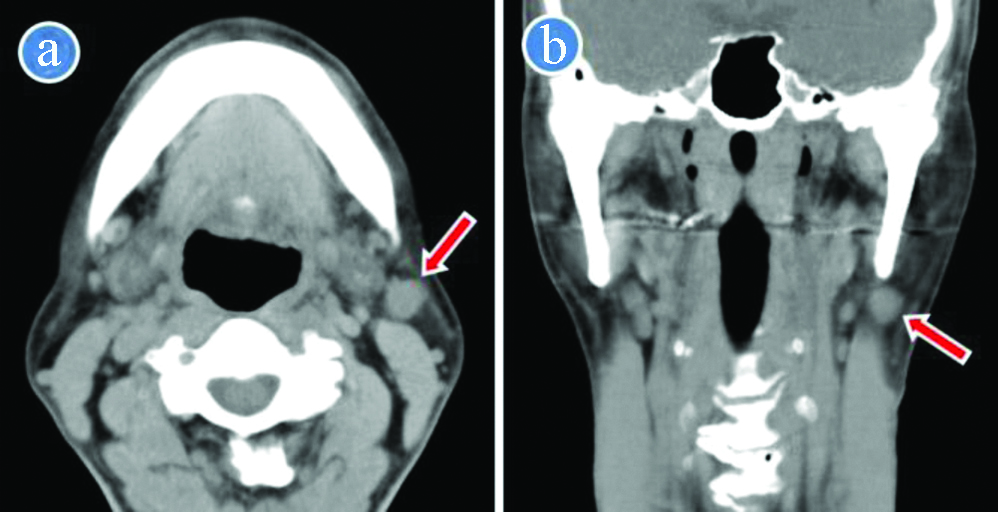
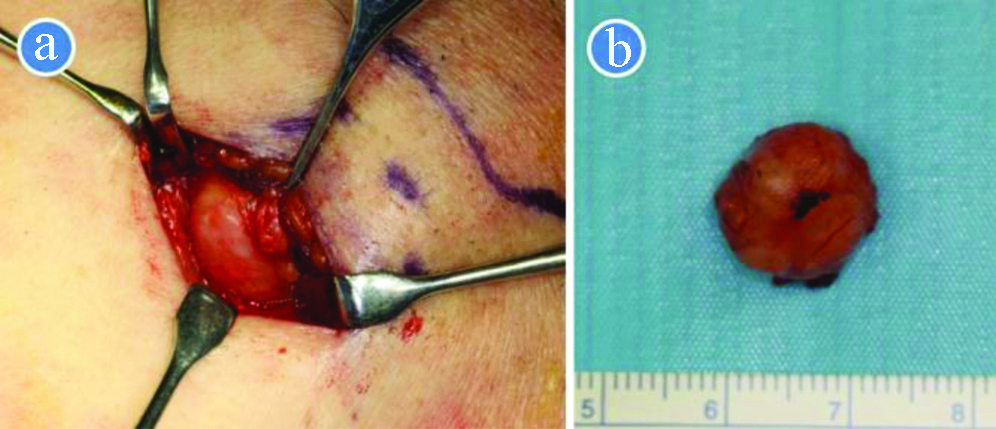
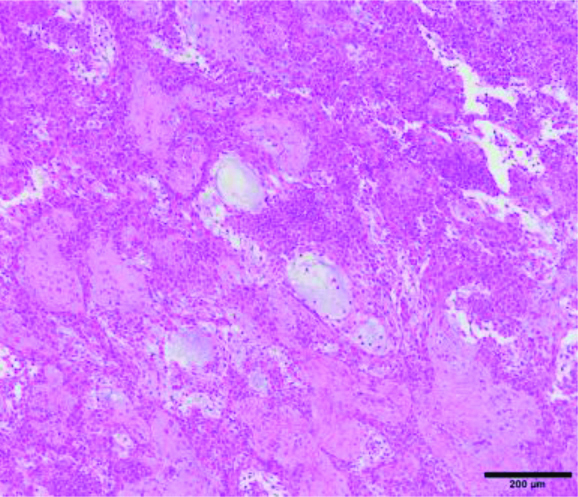
A 63-year-old male was referred to the Department of Oral and Maxillofacial Surgery becasue of left submandibular painless mass which has gradually grown for six years. The well-defined mass, measuring approximately 15×15 mm, was mobile and elastic hard. He was a nonsmoker and had no history of malignancy or tuberculosis. Clinical diagnosis was cervical lymphadenopathy. Computed Tomography (CT) revealed a well-circumscribed, round-shaped homogeneous mass (12×12×13 mm) was located below the left mandibular angle, anteriorly to the sternocleidomastoid muscle and posteroinferiorly to the submandibular gland [Table/Fig-1a,b]. Based on the clinical and radiological diagnosis of cervical lymphadenitis, he underwent removal of the lesion under general anesthesia. A 2 cm submandibular skin and the platysma muscle incision made, and the mass was removed easily without adhesion or connection of surrounding tissues including the submandibular or parotid gland [Table/Fig-2a,b]. Pathological diagnosis was pleomorphic adenoma without lymph node structure, and the tumour had myoepithelial and chondroid components [Table/Fig-3]. The postoperative course was uneventful without facial nerve palsy, and there was no recurrence 9 years after surgery.
Computed tomography revealed a well-circumscribed, round-shaped homogeneous mass (arrow) located below the left mandibular angle, anteriorly to the sternocleidomastoid muscle and posteroinferiorly to the submandibular gland. a) Axial image; b) Coronal image.
a) Intraoperative view. b) Removed specimen.
Microscopic pathology. The tumour had myoepithelial and chondroid components (Haemotoxylin and Eosin staining) (X100).
Heterotopic salivary gland tissue is defined as the presence of normal salivary gland tissue occurring outside of the normal distribution of the major and minor salivary glands [1,2]. Cervical heterotopic salivary gland tissue is rare and manifests as a mass, cyst, or draining sinus [2,3]. Tumours arising from cervical heterotopic salivary gland tissue are even rarer [1-7]. For the rarity, the present case was misdiagnosed with cervical lymphadenitis.
The embryological basis of heterotopic salivary gland tissue is unknown, but heterotopic salivary gland tissue may be caused by defective closure of the pre-cervical sinus [1]. Heterotopic salivary gland tissue arises in a lymph node, external auditory canal, middle ear, thyroglossal duct, hypophysis, mandible, mastoid bone, tongue, tonsil, hypopharynx, sternoclavicular joint, pituitary gland, thyroid, parathyroid gland, and in the upper and lower neck regions [1,2,4,5]. Heterotopic islands of salivary gland tissue are recognised as incidental microscopic findings, and are common in the peri-parotid and upper cervical lymph nodes [2,5-7]. The incidence of heterotopic salivary gland tissue in cervical lymph nodes was reported as 12.1% (31 of 257 patients) [8].
The mechanism of oncogenesis of salivary gland tumours in heterotopic sites is unclear, but the tumours may arise as a neoplastic transformation of heterotopic salivary gland tissue [5]. About 80% of heterotopic salivary gland tumours are benign [2]. Benign tumours arising from heterotopic salivary gland tissue are pleomorphic adenoma, Warthin’s tumour, and oncocytoma [1,2,4-7]. Warthin’s tumour is the most common benign tumour [2]. Malignant salivary gland tumours are reported as mucoepidermoid carcinoma, adenocystic carcinoma, acinic cell carcinoma, adenocarcinoma, and carcinoma ex pleomorphic adenoma [2,4,5]. A tumour arising from heterotopic salivary gland tissue is generally unilateral, but multiple ipsilateral cases with pleomorphic adenomas or Warthin’s tumours in parotid or submandibular lymph nodes [2,6] or bilateral case with three Warthin’s tumours was also reported [7]. Tumours arising from heterotopic salivary gland tissue are mainly adult, with a few pediatric cases [2]. Pleomorphic adenoma in the present case (adult male) was considered to arise in submandibular heterotopic salivary gland tissue, because the specimen had no lymph node structure.
For benign tumours arising from cervical heterotopic salivary gland tissue, local excision with close follow-up is appropriate management [2]. For the low-grade malignancies, local excision with close follow-up is performed as treatment of the benign tumours [3], whereas the management of high-grade malignant tumours includes neck dissection with/without postoperative radiation [2].
Concluding this, surgeons should take tumour arising from heterotopic salivary gland tissue into consideration in the clinical and radiological differential diagnosis of cervical mass.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? NA
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 23, 2020
Manual Googling: Sep 19, 2020
iThenticate Software: Jan 15, 2021 (20%)
[1]. La Macchia R, Stefanelli S, Lenoir V, Dulguerov N, Pache JC, Becker M, Pleomorphic adenoma originating from heterotopic salivary tissue of the upper neck: A diagnostic pitfallCase Rep Otolaryngol 2017 2017:576739610.1155/2017/576739629270325 [Google Scholar] [CrossRef] [PubMed]
[2]. Daniel E, McGuirt WF Sr, Neck masses secondary to heterotopic salivary gland tissue: A 25-year experienceAm J Otolaryngol 2005 26(2):96-100.10.1016/j.amjoto.2004.08.00915742261 [Google Scholar] [CrossRef] [PubMed]
[3]. Rodgers GK, Felder H, Yunis EJ, Pleomorphic adenoma of cervical heterotopic salivary gland tissue: Case report and review of neoplasms arising in cervical heterotopic salivary gland tissueOtolaryngol Head Neck Surg 1991 104(4):533-36.10.1177/0194599891104004191710048 [Google Scholar] [CrossRef] [PubMed]
[4]. Vegari S, Naderpour M, Hemmati A, Baybordi H, Pleomorphic adenoma of the cervical heterotopic salivary gland: A case reportCase Rep Otolaryngol 2012 2012:47065210.1155/2012/47065222953114 [Google Scholar] [CrossRef] [PubMed]
[5]. Surana R, Moloney R, Fitzgerald RJ, Tumours of heterotopic salivary tissue in the upper cervical region in childrenSurg Oncol 1993 2(2):133-36.10.1016/0960-7404(93)90023-R [Google Scholar] [CrossRef]
[6]. Shinohara M, Ikebe T, Nakamura S, Takenoshita Y, Oka M, Mori M, Multiple pleomorphic adenomas arising in the parotid and submandibular lymph nodesBr J Oral Maxillofac Surg 1996 34(6):515-19.10.1016/S0266-4356(96)90248-X [Google Scholar] [CrossRef]
[7]. Naujoks C, Sproll C, Singh DD, Heikaus S, Depprich R, Kübler NR, Bilateral multifocal Warthin’s tumors in upper neck lymph nodes. Report of a case and brief review of the literatureHead Face Med 2012 8:1110.1186/1746-160X-8-1122472434 [Google Scholar] [CrossRef] [PubMed]
[8]. Shinohara M, Harada T, Nakamura S, Oka M, Tashiro H, Heterotopic salivary gland tissue in lymph nodes of the cervical regionInt J Oral Maxillofac Surg 1992 21(3):166-71.10.1016/S0901-5027(05)80787-8 [Google Scholar] [CrossRef]