Since childhood oral diseases remain a major health problem. The deprived oral health impacts the quality of life negatively and for results in decrease in school performance [1]. In a survey done in 2010, untreated tooth decay in primary teeth was ranked tenth while listing the most prevalent diseases in the world [2].
Proximal cavitated lesions in primary teeth have high prevalence, with larger contact area between teeth and limited salivary access being attributing factors [3]. Also, children’s decreased dexterity to use dental floss and dependence on parent’s for removal of interproximal dental plaque acts as added factors [4]. Moreover, difficulty of mechanical control of biofilm can further result in faster progression of proximal lesions in primary teeth [5].
In order to decrease the caries burden there is an imperative need to detect caries at an early, preventable and reversible stage [6]. Although diagnosis is the first step, it remains problematic, especially in cases of proximal cavitated lesions due to lack of visibility and accessibility [7]. The continuous cycles of re- and de-mineralisation that the tooth undergoes during carious process denotes another major challenging factor that prevents assessment of the ongoing stage of dental caries [8].
Although dentists have various diagnostic aids at their disposal, visio-tactile method and radiographic method have long stayed as the methods of choice [9]. Both these methods utilise various scales and instrumentation procedures with each one having its own usage guidelines. Visio-tactile method has a good accuracy which is further improved when used in conjunction with detailed and validated index [10].
In recent years, ICDAS has been developed in response to the growing interest in detection and management of early lesions [11]. ICDAS-I was developed in 2002 and was later modified to ICDAS-II in 2005 [1]. ICDAS criteria has been shown to be a reliable and effective tool for caries detection and has been applied successfully in clinical and in in-vitro studies in primary, mixed or permanent dentition [12]. It is a standardised clinical scoring system for caries detection that includes cavitated and non-cavitated lesions [13].
Radiographic examination provides additional information about stage of occlusal and proximal cavitated lesions [3]. As the demineralised tooth area allows a greater filtration of X-rays showing a radiolucent zone, it helps to reveal interproximal caries which go unnoticed during regular intraoral examination.
ICDAS-ICCMS (2012) is a system that promotes staging of the caries -process, risk assessment and management. It provides a comprehensive set of clinical protocols that includes preventive, diagnostic and restorative decisions necessary “to preserve tooth structure and restore only when indicated” [3]. This system uses ICDAS for clinical staging of caries and ICDAS Radiographic score for radiographic staging of carious lesion.
However, the scientific data regarding the diagnostic value of visual examination on the proximal surfaces is scant and the limited trials conducted with reference to variety of classification criteria’s lack histological validation [14,15].
As primary mandibular molars are the most susceptible tooth to dental caries (13.67%) due to the varied morphological pattern of the primary posterior teeth [16,17]. For this reason lower posterior teeth were selected and included in the study. Thus, a study was conducted to assess the topographical distribution of proximal cavitated lesions on mandibular arch and on primary mandibular molar tooth surface and also to determine the extent of agreement between clinical and radiographic examination in identifying proximal cavitated lesions involving primary mandibular molars.
Materials and Methods
An observational study was conducted in Department of Pedodontics and Preventive Dentistry between July 2018-August 2019, including a total of 100 primary mandibular molars (D or E) from 70 children having proximal cavitated lesions (distal/mesial). The proximal cavitation was examined both clinically (ICCMS caries merged category scores) and radiographically (ICDAS Radiographic scoring system) and the correlation between both scores were analysed. Study methodology and design were approved by Institutional Ethical Committee (SGTU/FDS/MDS/24/1/519).
The sample size calculation was done on basis of percentage (%) of occurrence of mandibular primary carious molars in population group [18,19]. At α=5% with power of 90%. Minimum sample of 90 teeth was estimated to be included in the study for both clinical and radiographic examination.
Inclusion criteria: Children having proximal cavitated lesion (distal/mesial) in primary mandibular molar, having an ICDAS score of 2-6, whose parents gave consent for radiograph were included in the study.
Exclusion criteria: The children for whom consent was not received from their parents or those having primary mandibular molar teeth with ICDAS score of 0-1 were excluded.
A total of 830 children were examined clinically for presence of proximal cavitated lesions in their mandibular primary molars. A total of 350 children who fulfilled the inclusion criteria for the trial were selected and their parents were provided with the consent and information sheet. Out of the selected children, parents of 120 children returned the consent form. However, due to child unco-operativeness during radiography further 50 children were excluded. Hence, a total of 70 children with 100 proximally cavitated primary mandibular molars were finally included in the trial.
All corresponding radiographs for the included proximal cavitated lesions were taken and evaluated. The radiographs were taken with the digital X-ray machine (Carestream CS 2100) with distance between the focus and film being 100 cm and digital sensor holders (Rinn, XCP-DS, York, PA, USA) were used. Radiographs were evaluated for their quality on the computer-screen with 5X magnification. After initial evaluation, radiographs with no distortion or error were included.
Inter-observer reliability: Before evaluation, the examiners underwent core-training for ICDAS and ICDAS/ICCMS criteria usage online (https://www.iccms-web.com/content/icdas). After the training the examiners evaluated 10 pairs of clinical and radiographic records selected randomly for inter-and intra-observer reliability and reproducibility. The kappa values for both inter and intra-examiner reproducibility was 0.8.
After the training and reliability assessment the collected radiographic and clinical records were analysed by two different investigators individually. Two criteria were used for clinical and radiographic scoring of the data.
In the present study, ICDAS-ICCMS caries merged categories were used for both clinical and radiographic scoring of the data. For clinical scoring of data, ICDAS caries merged scores i.e., score 1 and 2 for initial lesions, 3 and 4 for moderate lesions and 5 and 6 for extensive lesions were used. The merged scoring was used in the study for better observation and statistical analysis [Table/Fig-1].
Representative cases of topographic distirbution in proximally cavitated mandibular primary molars.
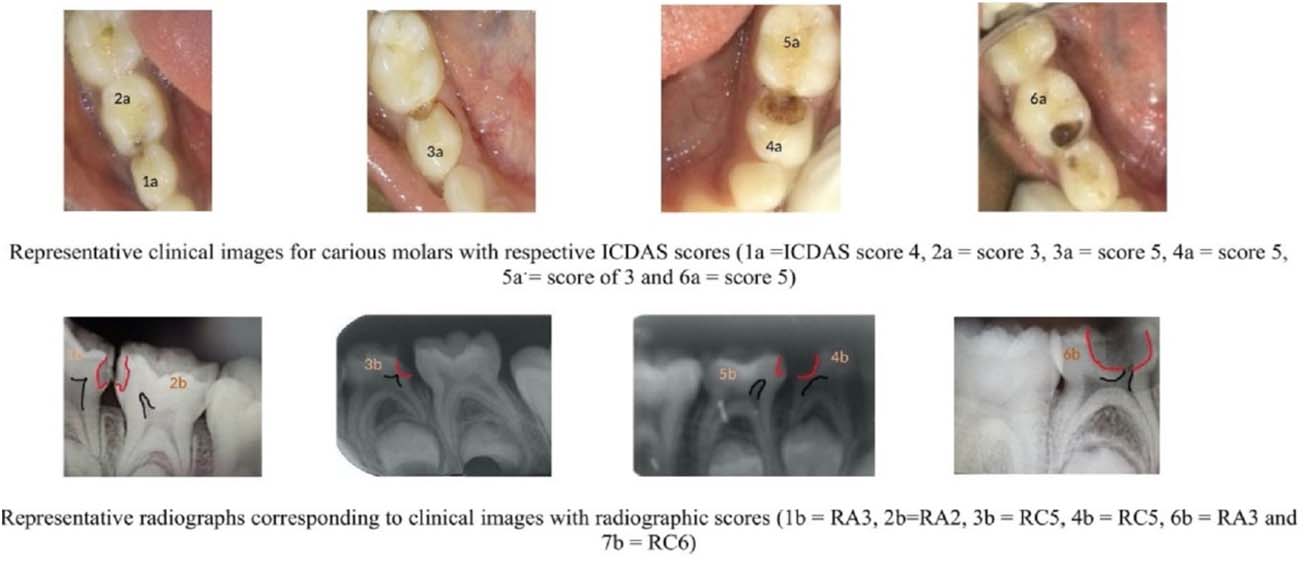
Similarly, ICDAS radiographic scores RA2 and RA3 for initial lesions, score of RB4 for moderate lesions and a score of RC5 and RC6 for extensive lesions respectively were used. In the present study, clinically moderate and extensive lesions were included [Table/Fig-1].
Statistical Analysis
Statistical analysis was done using SPSS version 19. Analysis for proximal cavitated lesion distribution on primary mandibular molars between first and second primary molar and on its tooth surface on the basis of ICDAS score and ICDAS/ICCMS radiographic scores was done using Chi-Square Test. The correlation between clinical ICDAS scores and radiographic ICDAS/ICCMS radiographic scores was analysed using Spearman’s correlation.
Results
The present study included a total of 100 primary mandibular molars having proximal cavitated lesions including 60 first and 40 second primary molars.
In the present study, comparative assessment of the caries prevalence between first and second primary mandibular molars on basis of ICDAS caries merged category scores and ICDAS radiographic scores was done. It was observed that the first primary molar had more lesions with ICDAS caries merged category score and ICDAS radiographic score of 5 and 6 in 40 and 44 lesions respectively as compared to second primary molar. The difference was also found to be statistically significant both clinically and radiographically (p-value≤0.001) [Table/Fig-2].
Topographical distribution of cavitated lesion (tooth involved and proximal surface involved) according to ICDAS clinical score and ICDAS/ICCMS radiographic score.
| Tooth involved | ICDAS score | ICDAS/ICCMS Radiographic score |
|---|
| 2 | 3 and 4 | 5 and 6 | 2 and 3 | 4 | 5 and 6 |
|---|
| First Primary molar | 0 | 20 | 40 | 9 | 7 | 44 |
| Second Primary Molar | 4 | 17 | 19 | 19 | 2 | 19 |
| Total | 4 | 37 | 59 | 28 | 9 | 63 |
| p-value | <0.001* | <0.001* |
| Proximal site of cavitation | ICDAS SCORE | ICDAS/ICCMS Radiographic score |
| 2 | 3 and 4 | 5 and 6 | 2 and 3 | 4 | 5 and 6 |
| Mesial | 4 | 15 | 14 | 17 | 2 | 14 |
| Distal | 0 | 22 | 45 | 11 | 7 | 49 |
| Total | 4 | 37 | 59 | 28 | 9 | 63 |
| p-value | 0.003* | 0.003* |
*denotes statistically significant using Chi-square test; ICDAS: International caries detection and assessment system; ICCMS: International caries classification and management system
Assessment of the topographical distribution of the proximally cavitated lesion on the mandibular molar tooth surface revealed that the distal surface of the tooth had a higher prevalence of caries (67) when compared to the mesial surface (33) which was found to be statistically significant (p-value=0.003) [Table/Fig-2].
When observing clinical ICDAS caries merged category scores and ICDAS radiographic scores for proximal cavitated lesions it was seen that ICDAS caries merged category score and ICDAS radiographic score of 5 and 6 were highest for both mesial and distal surface. On statistical analysis significant value was observed using Chi-square test for both clinical and radiographical analysis (p-value=0.003) [Table/Fig-2].
When comparing the clinical (ICDAS caries merged category scores) and radiographic (ICDAS radiographic scores), it was observed that there was a strong positive and statistically significant correlation between the scores (p-value≤0.001). The clinical (ICDAS caries merged category) score of 2 showed maximum correlation with ICDAS radiographic score of 2 and 3. ICDAS caries merged category score of 3 and 4 showed correlation with ICDAS radiographic score of 2 and 3 whereas ICDAS caries merged category score of 5 and 6 showed maximum correlation with ICDAS radiographic score of 5 and 6 [Table/Fig-3].
Correlation between ICDAS clinical score and ICDAS/ICCMS radiographic score.
| ICDAS/ICCMS Radiographic score | ICDAS score | Total | Correlation value | p-value |
|---|
| 2 | 3 and 4 | 5 and 6 |
|---|
| 2 and 3 | 4 | 24 | 0 | 28 | 0.861 | <0.001* |
| 4 | 0 | 9 | 0 | 9 |
| 5 and 6 | 0 | 4 | 59 | 63 |
| Total | 4 | 37 | 59 | 100 |
Denotes statistically significant using Spearman’s correlation; A strong positive correlation is seen between ICCMS score and ICDAS score and the correlation is statistically significant using Spearman’s correlation (R-value=0.861); ICDAS: International caries detection and assessment system; ICCMS: International caries classification and management system
Discussion
In paediatric dentistry, foundation for evidence based planning lies in early detection of carious lesions [20]. Early and accurate diagnosis would permit the use of various preventive therapies such as pit and fissure sealants, resin infiltration and fluorides, thereby reducing the need for drilling and filling and improving the overall dental health significantly [21].
In the present study, ICDAS/ICCMS system was used due to its ability to detect and manage early lesions and its validity and reliability to detect dental caries [8,22]. This helped to overcome shortcomings of other traditional caries classification methods such as DMFT/DMFS that classifies only cavitated and restored lesions as disease [23].
However, its reliability for proximal lesions of primary molars is not well documented. In the past, limited studies have been done comparing the clinical scores and radiographic scores for proximal cavitated lesions especially in primary molars. The present study was thus conducted to comparatively evaluate clinical diagnostic method used in detecting proximal caries in primary teeth with radiographic methods.
In the present study, right mandibular quadrant was observed to have more caries prevalence when compared to the left side. This finding can be associated to work by Cakur B et al., who reported that right-handed individuals had better oral hygiene because of their brushing efficiency and manual dexterity as compared to left handed individuals [24]. However, on the contrary, Tezel A et al., Ozgoz M et al., and Addy M have shown that left handers had an overall better oral condition [13,25,26].
Another finding of the present study was that on the basis of the topographic distribution, distal surface of primary mandibular molar was more prevalent to caries as compared to the mesial surface. It can be attributed to the tight contact points between proximal surfaces of primary molars which lead to higher plaque accumulation thus contributing to initiation and progression of proximal carious lesions [3].
Another reason for the aforementioned finding can be the presence or absence of generalised spaces (Baume spaces) in primary dentition. Primate spaces mesial to upper canine and distal to lower primary canine occur in mandibular arch. Owing to this, in mandibular primary first molar (D), distal surface has tight proximal contacts in comparison to the mesial surface thus leading to increased prevalence of caries [27].
Another observation in the study was that the first primary mandibular molar had more caries prevalence when compared to the second molar. It can be attributed to the eruption sequelae and timing. The second primary molar erupts 10-12 months later than the first primary molar. Hereby, first primary molar remains for an overall longer duration in the oral cavity, thus it is more prevalent to caries. It can also be due to the fact that until eruption of the first permanent molars, the second primary molar has only one proximal surface (mesial) in contact with another tooth. On the other hand first primary molar has contact points with both canine and second primary molar creating additional predilection site for developing proximal caries [28].
In the present study, when comparative evaluation of ICDAS clinical and ICDAS/ICCMS radiographic scores was done, a very strong positive correlation between the two was obtained using the Spearman correlation. Maximum correlation was seen between ICDAS score of 5 and 6 and its corresponding radiographic score of 5 and 6 respectively which is used for scoring of extensive lesions. Whereas, a minimum correlation was seen between clinical score of 2, 3 and 4 and its corresponding radiographic score of 2 and 3, respectively used for scoring of initial lesions.
Similar finding was reported by Subka S et al., Mitropoulos P et al., and Bhumireddy JR et al., who stated that the clinical and radiographic correlation increases in severe stages [3,14,29]. Radiographic examination was found to have lowest sensitivity at the initial demineralisation (initial white spot lesions) level of diagnosis. On the other hand, for detecting caries extending into dentin, radiographic examination showed highest sensitivity of all other diagnostic methods.
Limitation(s)
As caries is a multifactorial disease. The caries occurrence maybe affected by enumerable factors such as anatomical features, host factors such as diet, salivary flow rate among others and population group per se. So, these factors could have affected the distribution of dental caries within the population. Further in the present study only the topographical distribution of caries were only observed for proximal lesions on primary mandibular molar. Distribution of decay pattern on other primary tooth surfaces should also be observed.
Conclusion(s)
Mandibular primary first molar had significant prevalence of proximal cavitation compared to second molar along with distal surface being significantly involved in cavitation as compared to distal surface. Also, significant correlation was observed between clinical (ICDAS) and radiographic (ICDAS-ICMMS) scores for proximal cavitated lesions in primary mandibular molars with maximum reliability being observed as extended lesions.
*denotes statistically significant using Chi-square test; ICDAS: International caries detection and assessment system; ICCMS: International caries classification and management system
Denotes statistically significant using Spearman’s correlation; A strong positive correlation is seen between ICCMS score and ICDAS score and the correlation is statistically significant using Spearman’s correlation (R-value=0.861); ICDAS: International caries detection and assessment system; ICCMS: International caries classification and management system