Introduction
Naturally, the kids are curious. They begin exploring their environment and engaging with new objects as soon as they are mobile. But at the same time, while playing with fire or touching hot objects, they are likely to cause serious harm to themselves. Burn is characterised as damage to the skin or other organic tissue caused by thermal trauma, occurring when any or more of the skin cells or other tissue are killed by hot liquids, hot solids (contact burns), or flames (flame burns). Owing to radiation, radioactivity, strength, friction or chemical contact, burns are also considered to be skin or other organic tissue wounds.
Aim
To determine the current awareness of parents of children under five years with respect to first aid for burns and prevention. Evaluating the efficacy of planned awareness teaching among parents and to associate the knowledge with the selected demographic variables.
Materials and Methods
The present study was conducted in rural areas of Wardha, Maharashtra and 60 participants were recruited on the basis of inclusion criteria, using the purposeful technique of sampling. Structured questionnaires were the resources and the expected teaching was provided after the pre-test.
Results
According to the findings of the analysis in the score of pre-test information, 30% of parents of under five years kids had poor awareness score level, 70% of the parents of under five kids had average awareness score level, mean knowledge score was 5.20±1.97, post-test 10% of the parents of under five years kids had average, 80% good and 10% with an outstanding degree of knowledge score, the mean knowledge score was 10.30±1.87. Mean percentage score, pre-test was 32.50±12.32 and post-test, it improved to 64.37±11.73, thus indicating improved understanding of first aid for burns and its prevention for most parents.
Conclusion
It was statistically interpreted that the planned teaching program of the parents of children under five years on knowledge regarding emergency management and prevention of burns was very effective and has improved the knowledge significantly.
Introduction
In today’s world, injuries have become a normal occurrence. Road traffic accidents, domestic accidents, industrial accidents and rail accidents account for a high proportion of mortality, morbidity and disability rates. Burns are often known as a form of accident of all kinds and degrees [1]. Burns cause aesthetic issues as well as acute physical problems which may cause severe complications in the form of secondary bacterial infection, varying degrees of contractuation, if not taken proper care of [2]. Much of the impacted people are of low socio-economic status. The cost for the treatment of these injuries is high. The issue of burn injuries is more acute in developing countries because the treatment of burn victims requires specialist personnel and medical technologies that are costly and not always readily accessible. A burn is characterised as a skin injury caused by thermal trauma, occurring when hot fluid (scalds), hot solids (contact burns), or flames kill some or all of the cells in body or other tissues or tissues (flame burns). Owing to radiation, electricity, radioactivity, friction or chemical interaction, burns are also considered to be skin or other organic tissue wounds [3]. Superficial or first-degree burns, thermal burns, inhalational burns, burns of second degree or partial thickness, third degree or full thickness burns may be differentiated and graded as chemical burns, radiation burns, electrical burns [2], thermal burns, first degree or superficial burns, second-degree or partial-thickness burns, inhalational burns. Infants below one year of age are in a separate category. Scald burns are the most common type of burns that occur. That tend to occur across geographical and economic classes among children younger than six years of age, upon observation. When a child pulls down a hot fluid container on his or her hands, such as a cup of coffee, typical scald burns occurs on the upper limb and trunk [2].
Roughly 10% of all accidental injury fatalities are due to fire related burns. According to World Health Organisation (WHO) statistics, studies from high income nations indicates that mortality from burns is the main determinant of house fires or other conflagrations. Smoke inhalation is closely correlated with mortality in children over three age years. The bulk of children’s burn-related deaths are caused by burns from fire, scalds and scales touch. The burns are the significant factor in overall burn morbidity and a significant cause of disability [2].
A study showed that in and around the house, 65% of childhood burns have occurred in four low-income countries. The most popular area of the house is generally the kitchen. Children will disrupt receptacles with hot liquids in this room by bursting shops, standing on hot coals, or splashed with hot oil for frying. Studies have also found that children whose parents smoke in bed are at greater risk of burns. Two peak periods of time were established for accidents involving burns, the late morning when domestic activities are carried out and the evening meal time [2]. Childhood burns are primarily ecologically disturbing and can be preventable. Therefore it would seem normal that a combination of environmental changes could concentrate on the prevention of burns. Particular attention needs to be paid to parental education and product protection in the kitchen.
Many times death occurs due to the postponement in hitting the victim to proper health services and poor first aid and recovery shortages skills. If assistance is offered to victims as soon as possible after the accident or injury, on the other hand, a life can be saved [4,5]. Also the first helper should have sufficient information and expertise for what he should be doing to support and reassure the victim. This helps to reduce rates of mortality and morbidity, complications caused by accident or treatment delay, and lowers the victim’s monetary burden [6]. Thus, basic first aid training and knowledge is desirable for all individuals [7-9].
Overall, children are at high risk of burn fatalities, with a worldwide rate of 3.9 deaths per 1,00,000 individuals [10]. Kids have the highest rates of death from burns among all people globally. Nearly 96,000 children under 20 years of age worldwide as a result of fire induced burns were estimated to be fatally burned in 2004 [2].
The second most significant cause of accidental death in children is burn injuries [11]. According to the WHO 2004 estimated just over 3,10,000 individuals died as a result of fire related burns, of which 30% were under 20 years of age. The 11th leading cause of death for children under five years of age is fire related burns.
The death rate was eleven times higher in low and middle income countries than in high income countries, 4.3 per 1, 00,000 compared to 0.4 per 1, 00,000. Fatalities associated with burns reflect great geographical variability. Among the WHO regions of Africa and South-East Asia and the eastern Mediterranean countries with low and medium income region, the majority of deaths occur in the world’s poorer nations. A research in India showed that only 22.8% of patients received ample first aid for their burns. The rest either received no first aid or were rubbed with improper care like, raw eggs, toothpaste, mashed potatoes or oil [11]. Training on the effects of the immediate use of cool water on burns as an effective first aid treatment should be widely encouraged [12].
Studies have shown that primary caregivers lack knowledge of scalds and burns in terms of home protection and first aid management [11,13,14]. In the event of a disaster, basic awareness of burn prevention and first aid strategies can help to minimise burn related morbidity and mortality rates in children under the age of five years [13]. Among primary caregivers, studies on awareness need to be performed. The researcher therefore decided to conduct a study on parents’ knowledge of first aid for burns and preventive measures that can be taken alone to avoid further complications, and it is believed that parents can benefit from the gain of knowledge so in preventing and treating burns, they can work effectively with infants [13].
The goal of the study is to estimate the effect of planned teaching on the awareness of parents and prevention of first aid for burns of children under the age of five years.
Hypothesis:
H1: In relation to first aid for burns and its prevention, among parents under five, there is a major distinction between pre-test and post-test awareness scores.
H2: A significant association exists between the level of parental knowledge and selected variables of socio-demographic nature.
Materials and Methods
The present pre-experimental, pre-test post-test study was conducted in the selected rural area of Wardha district, Sawangi, after obtaining the Ethical Committee Approval DMIMS(DU)/IEC/2017-18/6811. Data from parents of less than five years of age from a selected rural area in Wardha was collected. Quantitative research has been used to measure parents’ understanding of first aid management and burn prevention. Participants were chosen by means of a purposeful sampling technique. Sixty mothers were selected according to the inclusion criteria and availability.
Inclusion criteria: Parents of children under five years of age and ready to give consent.
Exclusion criteria: Parents who were not present during data collection or parents who were chronically ill.
They were given the demographic questionnaire. To evaluate the information concerning first aid for burning and its prevention, a standardised knowledge questionnaire was used. Initially the level of knowledge of mothers of children under five years of age regarding the first aid for burn and its prevention were assessed by administered questionnaire to mother and planned teaching was given on the same day and a post-test was accomplished on 7th day. Participants were cooperative and involved in part of this study and it was not difficult for the researcher to perform the study between participants.
Planned Teaching- Prevention of Burn
Meaning of burn- To destroy, damage or injured by fire or heat.
Causes and Risk of Burn
Flames.
Hot liquid or steam.
Warm metal, glass or other objects.
Electric currents.
X-ray radiation or cancer cure radiation therapy.
Sunlight from a sunlamp or tanning bed, or ultraviolet light.
Chemicals, such as potent acids, dye, paint or fuel thinner.
Misuse
First degree burn-
Superficial first degree burns affect either the epidermis or the outer skin layer. The location of the burn is red, painful, dry and without blisters. An example is mild sunburn. Long-term tissue damage is uncommon and typically increased or reduced skin colour.
Second degree burns-
Second degree burns the epidermis and dermis affect (partial thickness burns) (lower layer of skin). Pain, redness, swelling and blistering are caused by them.
Third degree burns-
Burns of the third degree go through the dermis (burns of maximum thickness) and affect deeper tissues. They result in skin that may be numb that is white or blackened, burnt.
Fourth degree burn-
There is a charred looking appearance in the affected region. The colour of the exposed bone and muscle tissue can also be white. In comparison to first or second degree burns, fourth degree burns aren’t painful.
Symptoms
There are signs that may include:
Blisters.
Profound redness.
The burned area can appear shiny and wet.
Skin that is painful to touch.
In an irregular pattern, the burn can be white or discoloured.
First aid of Burn
Stopping the process of fire.
Run cool water through the burn.
Do not immediately use ice on the burn wound.
Home remedies/ointments should not apply.
Cover a clean bandage or cloth with the burn.
For pain, take Ibuprofen or Acetaminophen.
If required, seek medical attention.
Flame burning-
Keep the burned area under cool running water (not cold) or apply a cool wet compress until the pain is relieved. From the burned area, remove rings or other tight objects. Before the area swells, strive to do this rapidly and gently.
Complication
Curling’s ulcer is an acute gastric erosion that results from extreme burns as a complication when decreased plasma volume leads to gastric mucosa ischemia and cell necrosis (sloughing). First described in 1823, the disease was named after a physician, Thomas Blizard Curling, who observed ten such patients in 1842.
Protection of the burn area
(a) The burning area should be covered by a clean, dry cloth.
(b) Dressing, to avoid pollution
(c) Do not sever any shaped blisters
The best home remedies for burns
Air for refrigeration. The first thing you should do when you get a mild burn is to run cool (not cold water) for about 20 minutes over the burn area.
Cool compresses.
Ointments of antibiotics.
Aloe vera.
Honey.
Reduced exposure to the sun.
Take a pain reliever from over-the-counter.
Medical Emergency Care
Cover the area with a clean, soft cloth or towel, if the burned area is large:
The burns caused by a fire, an electric wire or plug, or chemicals.
The burn is on the face, hands, feet, joints, or genitals [14].
The burn appears infected (with swelling, pus, or increasing redness or red streaking of the skin near the wound) [14].
Prevention
Be vigilant when using candles, space heaters, and curling irons
Holding kids away from radiators.
Be careful with hot drinks.
Prior to placing a child in the tub, check the temperature of the bathing water.
Study the smoke alarm batteries at least once a month.
Hold a kitchen fire extinguisher
Do not allow tiny children to play in the kitchen while someone is cooking.
Results
The frequency and percentage wise distribution of parents below the age of five years old children are shown in [Table/Fig-1] in terms of age, parental schooling, type of family, monthly family income, parental employment status. The distribution of parents of children under five years according to their age in years indicates that 30.0% of them belonged to the age group 25-30, 50.0% to the age group 31-35, 10.0% to the age group 36-40, and 10% to the age group 40-plus. The distribution, according to their educational background, of parents of children under five years indicates that 40% of them were trained up to primary, 10% up to secondary, 40% up to graduate, and only 10% of them were trained up to and above post-graduation. The distribution of parents of children under five years according to their family type shows that 30% of them belonged to nuclear families and 70% belonged to joint families.
Percentage wise distribution of parents of children under five years according to their demographic characteristics.
| Demographic variables | No. of mothers (n=60) | Percentage (%) |
|---|
| Age (years) |
| 25-30 | 18 | 30.0 |
| 31-35 | 30 | 50.0 |
| 36-40 | 6 | 10.0 |
| Above 40 | 6 | 10.0 |
| Educational qualification of parents |
| Primary education | 24 | 40.0 |
| Higher secondary education | 6 | 10.0 |
| Graduate | 24 | 40.0 |
| Post graduate | 6 | 10.0 |
| Type of family |
| Nuclear | 18 | 30.0 |
| Joint | 42 | 70.0 |
| Extended | 0 | 0 |
| Family income per month(rs)/Father income |
| 5000-10000 | 24 | 40.0 |
| 10000-15000 | 24 | 40.0 |
| 15000-20000 | 0 | 0.0 |
| 20000 rs Above | 12 | 20.0 |
| Occupational status of parents |
| Government employee | 12 | 20.0 |
| Private employee | 30 | 50.0 |
| Others | 18 | 30.0 |
The distribution of parents of children less than five years of age, according to their monthly family income in rupees, indicates that 40% had an income of 5000-10000 rupees, 40% in the range of 10000-15000 rupees, and 20% of them had a monthly income of more than 20000 rupees and above per month.
The distribution of parents of children under five years of age shows that 20% of them were supervised, according to their occupational status. Fifty percent of the staff were private and other professionals, and 30% were private workers.
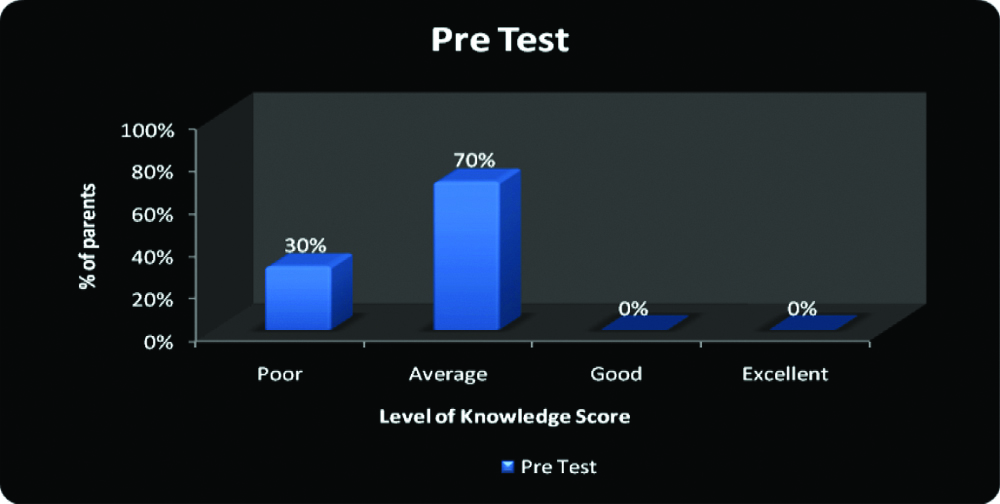
Pre-test Knowledge Score of parents of children under five years of age-on the basis of structured questionnaire.
The results of the pre-test results showed that 30% of parents of children under five years of age had a poor level of knowledge score, 70% had an acceptable level of knowledge score, and none had a good and outstanding level of knowledge score. The minimum score was 1 and the maximum score was 8. For mean, the score was 5.20±1.97 with a mean percentage score of 32.50±12.32 [Table/Fig-2].
Assessment with pre-test Knowledge score.
n=60
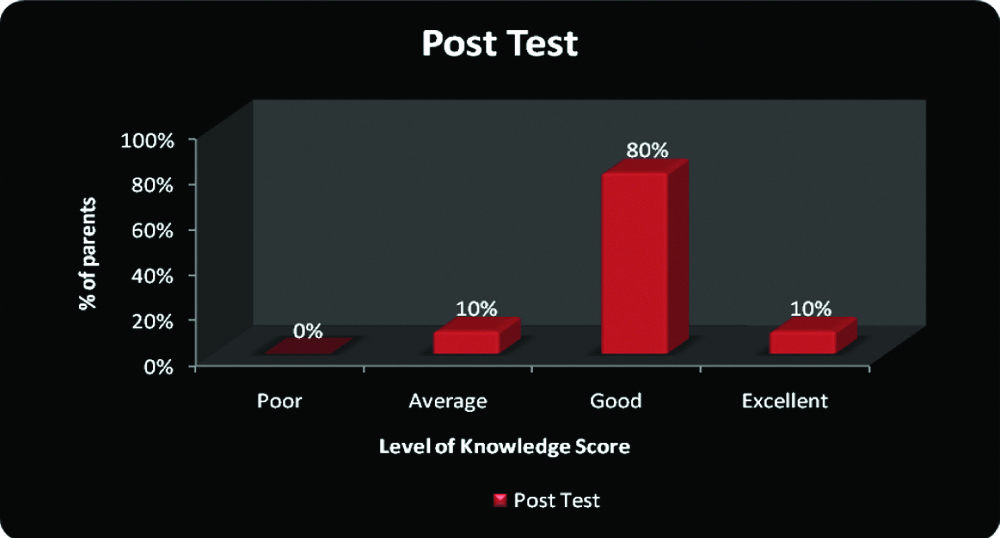
Post-test Knowledge Score of parents of children under five years of age-on the basis of planned teaching
The findings of the post-test results show that 10% of parents with less than five children had an average knowledge score, 80% had a good knowledge score, and 10% had an excellent knowledge score. The minimum score was 7 and the maximum score was 13. The mean score was 10.30±1.87 after comparing the pre-test and post-test, with a mean percentage score of 64.37±11.73. which indicates that there was an improvement in the post-test [Table/Fig-3].
Post-test level of knowledge score of parents of children under five years of age.
n=60
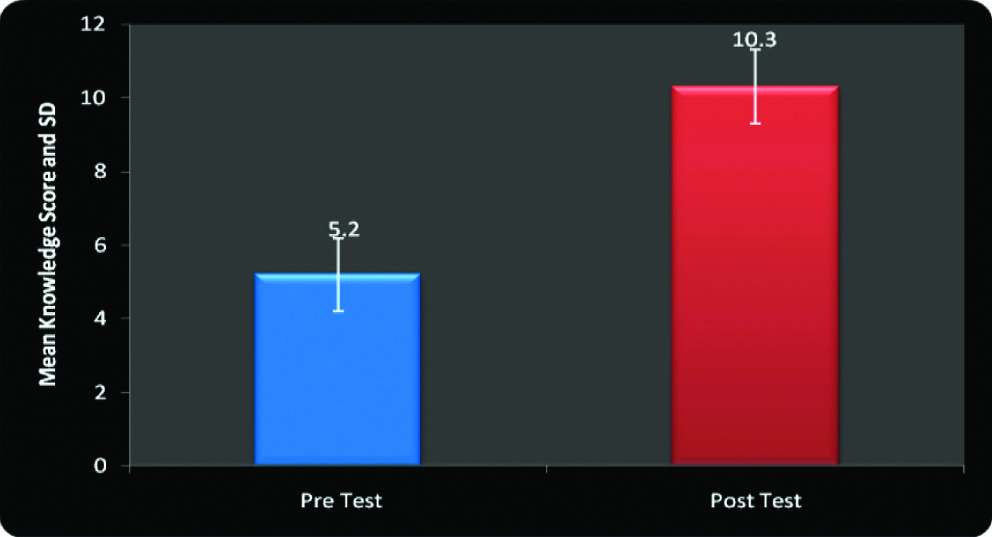
Comparison of parents of the Wardha district’s pre-test and post-test awareness scores, children regarding first aid for burning and its preventive measures is shown in [Table/Fig-4]. Mean, standard deviation and mean difference values are compared and student’s paired ‘t’ test is applied at 5% level of significance. For n=60, i.e., 29 degrees of freedom, the tabulated value was 2.05. At 5% significance level, the calculated ‘t’ value is much higher than the tabulated value for the overall knowledge score of parents of children the level of significance which is statistically appropriate. It is therefore statistically interpreted that the planned knowledge teaching concerning first aid for burning and its Wardha district preventive measures is effective. H1 is thus accepted.
Effectiveness of planned teaching regarding First aid for burn and its preventive measures.
n=60
Discussion
The present study was performed in Wardha’s rural area and the subjects were selected without probability using a convenient sampling technique. A questionnaire on structural knowledge was the tool for data collection. The pre-test was administered on the first day, followed by scheduled instruction, and the post-test was performed on the seventh day.
A supported study was conducted in Muradabad by Mr. Madan Mohan Gupta and Mr. Rohit Gautam [15], the pre-test post-test result revealed that the pre-test knowledge score of mothers of under five years children 9 (15%) having good knowledge score, 51 (85%) mothers were having average knowledge score and none were having poor knowledge. In post-test knowledge score 56 (93.33%) mothers had good knowledge score, 4 (6.7%) mothers were having average knowledge score and none had poor knowledge. The mean score of pre-test score was 2.15 and post-test mean score was 2.93, Standard deviation of pre-test was 0.36 and post-test standard deviation was 0.251 while “t” value was found to be 19.946 which is significant at 0.05 level at the table value 2.00. This indicates that there will be a significant difference between the knowledge score of the pre-test and the post-test test, so H1 is accepted.
It is therefore known that the STP on burn prevention and first aid management among mothers of children under the age of five was successful in improving the awareness score for mothers of under the age of five.
In the current study, pre-test results showed that 30% of parents of children under five years of age had a bad level of knowledge score, 70% had an average level of knowledge score, and none of them had a decent and outstanding level of knowledge score. The minimum score was 1 and the maximum score was 8. The mean score was 5.20±1.97 with a mean percentage score of 32.50±12.32. Post-test result findings showed that 10% of parents of children under five years of age were having average level of knowledge score, 80% of them had good level of knowledge score, and 10% of excellent level of knowledge score. The minimum score was 7 and 13 was the highest score. The mean score was 10.30±1.87 with a mean percentage score of 64.37±11.73. After evaluating pre-test and post-test it shows that teaching increased the knowledge of the parents in the study as expected quite significantly.
Nursing Implications
Nursing practices: Learning is an active method aimed at translating the abilities and values of experience into new behaviour. Nurses should test the awareness of parents visiting different paediatric clinics and in the community about burn first aid and its prevention. Therefore, different educational activities can be carried out for parents on the basis of needs that help to enhance the awareness of parents about first aid for burning and its prevention. Nurses will work to avoid secondary complications of community burning of infants in close partnership with health visitors, NGOs and other voluntary health organisations.
Nursing administration: Nurse as an administrator plays role in educating the professionals and policy making such as mass health education measures in the community. Being an administrator, one can arrange in-service education and special training program regarding first aid for burn and its prevention for staff and students in collaboration of both pediatric and community departments to upgrade knowledge of parents of children under five years of age. The hospital should have a policy to provide health education material to all in-patients and out-patients. In order to enhance parents’ awareness of first aid for burning and its prevention, nurses should encourage higher authorities to conduct outreach initiatives in the neighbourhood.
Nursing education: The nursing programme should include activities such as preparation of booklets, handouts, pamphlets, meal planning cards, diet plans that can be provided to health workers to circulate in the community and to parents attending pediatric clinics.
Conclusion(s)
The pre-experimental study has brought out an important relationship between the studies variables. The findings proved that the planned teaching regarding first aid for burn and its prevention has improved the knowledge. There is a statistically relevant correlation between post-test information scores and demographic variables, including age of the parents, educational qualification, type of family, family income per month, occupation of parents. Further a comparative study is recommended in future to determine parents’ awareness of burn first aid and its rural and urban prevention. A future research could be undertaken to determine the efficacy of the related problem of scheduled teaching.
In a broad community, comparative research can be carried out to determine the knowledge and parents’ actions about burning first aid and its avoidance.
[1]. NIMHANS BISB fact sheet child injury, Available from URL. http://www.censusidia.gov.in/census_data_2001/India_at_glanie/broad_aspx [Google Scholar]
[2]. Peden M, Ogegbite K, Ozanne-Smith J, Hyder AA, Branche C, Fazlur Rahman AKM, World report on child injury prevention, world health organization 2008, PP 79-93Available from URL: http://whqlibdoc.who.int/publications/2008/www [Google Scholar]
[3]. Facts about injuries: burns Genova, World Health Organization and international society for burn injuries, 2006. Available from URL: (http://www.who.int/entity/violence_injury_prevention/publications/other_injury/en/burns_factsheet.pdf.accessed17April2008) [Google Scholar]
[4]. Joyce BM, Jane HH, Annabelle KM, Medical Surgical NursingVol-26th Edition:1331-1338. [Google Scholar]
[5]. Chung ECH, Burn injuries in China: A one year survey at the united Christian HospitalHong Kong Practice 1996 18:631-36. [Google Scholar]
[6]. First aid to the injured St. Johns Ambulance association book published by volunteers of St. John’s ambulance brigade. Pg 5-6 [Google Scholar]
[7]. First aid to the injured Saint Johns Ambulance Association. Introduction to First Aid 1st Edition, published by lieutenant general R S Hoon, Pg 9-10 [Google Scholar]
[8]. Han J S, Kim DH, A study of the types of burns in children and mothers preventive attitudes to and knowledge of burnsKorean Journal of Child Health Nursing 1998 4(1):97-104. [Google Scholar]
[9]. Gulani KK, Community Health Nursing, principles and practicesfirst edition:390 [Google Scholar]
[10]. Lal P, Rahi M, Ingle GK, Epidemiological study of burn injuries in a slum community of delhiIndian Journal of Community Medicine 2006 31(2):96 [Google Scholar]
[11]. Olatain PB, Iyidobi EC, Olaitan JO, Ogbonnaya IS, Burns and Scalds: First-Aid Home Treatment and Implications at Enugu, NigeriaAnnuals of Burns and Disasters 2004 16(2):61-63.Available at: www.researchgate.net/publication/288255046_Burns_and_scalds_First-aid_home_treatment_and_implications_at_Enugu_Nigeria [Google Scholar]
[12]. Singer AJ, Gulla J, Thode HC Jr, Cronin KA, Department of emergency medicine, stong brook, USAPediatric first aid knowledge among parentsPediatric Emergency Care 2004 20(12):808-11.10.1097/01.pec.0000148028.53598.5c15572967 [Google Scholar] [CrossRef] [PubMed]
[13]. Justin-Temu M, Rimoy G, Premji Z, Matemu G, Department of pharmaceutics, MUHASCauses, magnitude and management of burns in under fives in district hospital in Dares salaam, TanzaniaEast African Journal of Public Health 2008 5(1):38-42.10.4314/eajph.v5i1.3897518669122 [Google Scholar] [CrossRef] [PubMed]
[14]. Brownell M, Friesen D, Mayer T, Childhood injury rates in ManitobaCan J Public Health 2002 93(suppl. 2):50-56.10.1007/BF034036196979765 [Google Scholar] [CrossRef] [PubMed]
[15]. Gupta MM, Gautam R, A Study to assess the Effectiveness of Structured Teaching Programme on Knowledge regarding Prevention and First Aid Management for Burns among Mothers of Under Five Children in selected community area at MoradabadJNPE 2019 5(1):01-04.Available at: http://www.ramauniversityjournal.com/nursing/pdf_march19/1.pdf [Google Scholar]