Osteogenesis Imperfecta: Dreadful Infantile Dysplasia
Bhushita Guru1, Bhushan N Lakhkar2, Bhavana B Lakhkar3
1 Associate Professor, Department of Radiology, Datta Meghe Institue of Medical Sciences, Wardha, Maharastra, India.
2 Professor, Department of Radiology, Datta Meghe Institue of Medical Sciences, Wardha, Maharastra, India.
3 Professor, Department of Paediatrics, Datta Meghe Institue of Medical Sciences, Wardha, Maharastra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Bhushita Guru, Flat No. 204, Datta Residency, Gokul Builders, Sawangi (Meghe), Bldeu Campu, Sholapur Road, Wardha, Maharashtra, India.
E-mail: bhushitalakhkar@gmail.com
Deformity, Demineralisation, Fractures, Newborn
A male newborn was presented with deformities of lower limb noticed at birth. Baby was full term, delivered normally in a Tertiary Care Hospital, cried immediately after birth and was feeding normally, apparently irritable while handling but could be consoled on feeding. There was history of short stature in father with history of fractures in lower limb twice. Previous baby was born with multiple deformities and had multiple swellings along the rib cage however he didn’t survive beyond six months. Antenatal ultrasound was done at 30 weeks which showed two fractures with bent bones one each in both femurs.
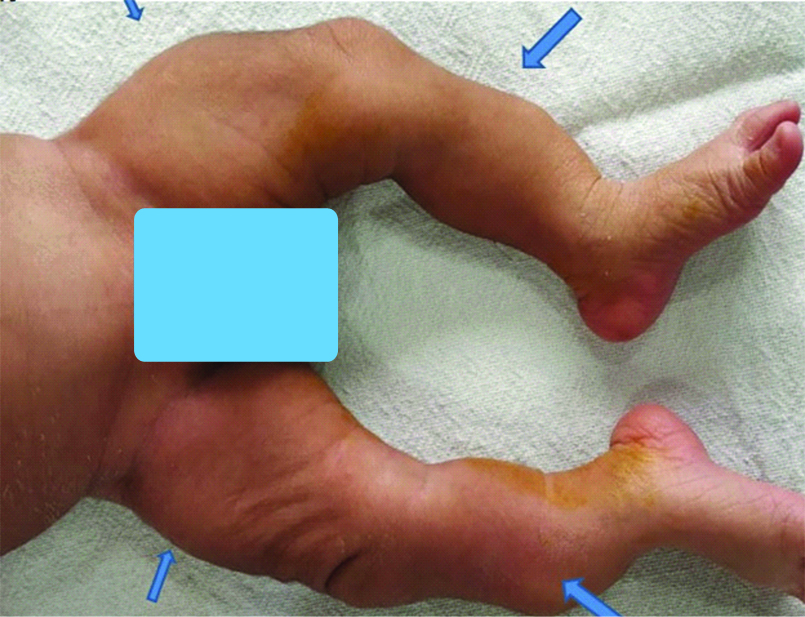
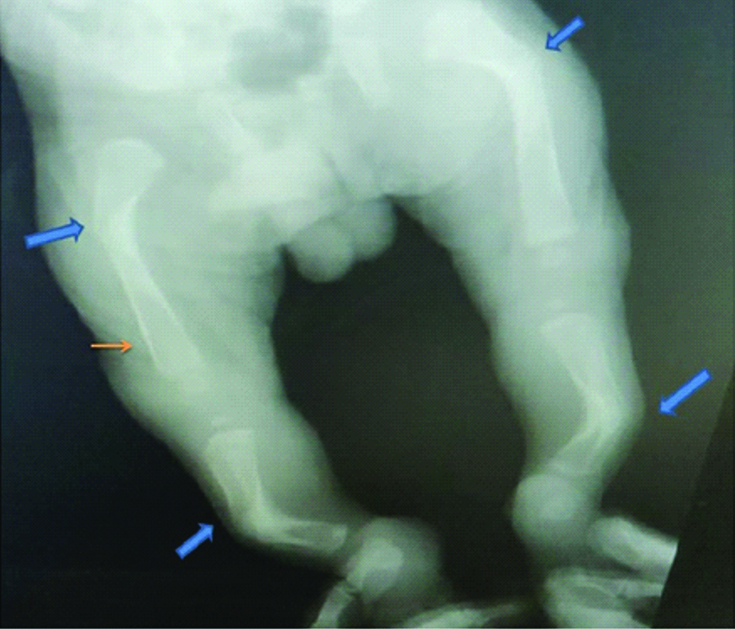
On clinical examination, there were bony irregularities and thickness felt on both femurs and tibia [Table/Fig-1]. Rest of examination was normal. X-ray of bilateral lower limbs showed thinned out cortex with demineralisation. It was also associated with multiple fractures in all the bones of lower limbs [Table/Fig-2]. However, sclera was normal. All these factors were diagnostic of Osteogenesis Imperfecta (OI) type II. The baby died on 6th day with respiratory infection. The genetic examination was not done as parents didn’t give consent for it.
A new born baby with multiple deformities in bilateral limbs (Blue arrows show sites of deformities which were palpable also).
Radiograph of both lower limbs in newborn with deformed limbs shows multiple nonhealed fractures of bilateral femur, tibia and fibula (blue arrows). The bones show demineralisation with thinned out cortex(orange arrow).
Osteogenesis Imperfecta (OI) is an autosomal dominant condition with typical presentation of X-rays and family history. OI is also known as a brittle bone disease and its mostly characterised by increased bone fragility and decreased density due to abnormalities of type I collagen [1]. It’s a rare autosomal dominant disorder affecting every 10000-20000 births [1]. However, no particular data as such is available from India. The incidence of type I OI has been reported between 2.35 to 4.7 in 100000 worldwide, incidence of type II OI is between 1 in 40,000 to 1.4 in 100000 live births. However, the exact incidence of types III and IV OI is not known [2].
It is a fatal dysplasia usually diagnosed antenatally by around 17 weeks [3]. Ultrasound usually shows abnormalities of skull, limbs, ribs and spine in form of decreased echogenicity (due to decreased bone mineralisation), deformities due to fractures and callus formations [4]. Usually such pregnancies are terminated due to fatal prognosis of the babies. When termination of pregnancy is performed postmortem radiographs are very useful in confirming the diagnosis and specifying foetal bone abnormalities [1]. However, in our case the anomaly was missed on anomaly scan of the fetus and was later diagnosed at 30 weeks. Hence, the patient couldn’t terminate the pregnancy.
A common finding on X-ray is osteopenia of bones followed by bone fractures, callus formations and deformity. Fractures are most commonly seen in diaphysis of long bones. Thinning and bending of long bones are seen which are often complicated by fractures at the concave aspect of bones. The healed fractures lead to angulations with callus formations which further leads to formation of deformities [3].
The most common differential diagnosis of OI is non-accidental injuries. Non-accidental injury can be differentiated from the former by presence of metaphyseal corner fractures, different age of fractures and no evidence of osteopenia [5]. OI is a rare fatal dysplasia and can be diagnosed at the anomaly scan at 18 to 20 weeks antenatally. It should be suspected in all children presenting with increased bone fragility, including fractures that occur with little or no trauma. Positive diagnosis is made on the basis of personal and familial medical history, physical examination (preferably with a clinician who is familiar with OI), radiography and, in some cases, complementary investigations such as bone densitometry, biochemical tests or DNA-based sequencing.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 05, 2020
Manual Googling: Nov 17, 2020
iThenticate Software: Dec 21, 2020 (4%)
[1]. Renaud A, Aucourt J, Weill J, Bigot J, Dieux A, Devisme L, Radiographic features of osteogenesisimperfectInsights Imaging 2013 4(4):417-29.Published online 2013 May 1910.1007/s13244-013-0258-423686748 [Google Scholar] [CrossRef] [PubMed]
[2]. Sillence D, Osteogenesisimperfecta: An expanding panorama of variantsClinOrthopRelat Res 1981 (159):11-25.10.1097/00003086-198109000-00004 [Google Scholar] [CrossRef]
[3]. Borić I, Vučković RP, Imaging in osteogenesisimperfectaPaediatr Croat 2017 61:122-28. [Google Scholar]
[4]. Bulas DI, Stern HJ, Rosenbaum KN, Fonda JA, Glass RB, Tift C, Variable prenatal appearance of osteogenesisimperfectaJ Ultrasound Med 1994 13:419-27.10.7863/jum.1994.13.6.4198083940 [Google Scholar] [CrossRef] [PubMed]
[5]. Offiah A, van Rijn RR, Perez-Rossello JM, Kleinman PK, Skeletal imaging in child abuse (non-accidental injury)Pediatr Radiol 2009 39:461-70.10.1007/s00247-009-1157-119238374 [Google Scholar] [CrossRef] [PubMed]