Injuries among children are increasingly becoming a major global health problem with long bone fractures constituting a significant subset of these injuries [1,2]. Moreover, fracture of the forearm bones account for the larger proportion of childhood fractures. It accounts for about 30% of all the fractures [3,4].
Children with forearm fractures are attracting research interest because of the possibility of deficiency of vitamin D and many of these studies were carried out mostly in temperate regions. Studies among healthy white children who had forearm fractures demonstrate an association with lower Bone Mineral Density (BMD) compared with peers without forearm fractures [5,6]. Similar study in Afro-American children with forearm fractures also showed a correlation with low serum 25-hydroxyvitamin D and low BMD [7]. Studies above were done in the temperate region which found an association between forearm fractures in children and low serum vitamin D3. Study in our environment have shown low levels of 25(OH)D in normal Nigerian children, but the association with forearm fractures has not been studied [8].
Although low 25-hydroxyvitamin D{25(OH)D} levels are associated with lower BMD and increased risk of osteoporotic fractures in adults, the association of 25-hydroxyvitamin D level with forearm fracture risk in children has not been previously reported in our environment as we are not expected to have deficient or insufficient levels of vitamin D due to our tropical location with its attendant abundant sunshine. So, the present study was aimed to determine the serum vitamin D levels in children with forearm fractures comparing with controls of the same age group without fractures and whether an association exists between serum vitamin D level and occurrence of forearm fracture [9,10].
Materials and Methods
This was a case control study conducted over a year from January 2018 to December 2018 at a tertiary health facility in South-West Nigeria among paediatric patients. Ethical approval was obtained from the Ethics and Research Committee of the institution (ERC/2017/01/05). Informed consent was obtained from the parents or care givers of the children in both the study and control groups.
There was a study group comprising of 30 patients aged 0-15 years who presented with forearm fracture(s) at the paediatric emergency unit and the control group were 30 paediatric patients of same age range presenting with other non-fracture related complaints at the paediatric child welfare and out-patient clinics. In the present study, 0-15 year age group was chosen inorder to cover all the paediatric age groups. However, the lowest age group in the study was from two years.
Sample size was estimated based on the formula for comparing the means between two groups using outcome variables from a previous work on vitamin D3 [11,12]. The power of our study was however set at 80% with statistical significance set at 0.05.
Inclusion criteria: Included were patients within the ages 0-15 years presenting at the children emergency wards of the institution with forearm fractures, (Study Group) and similar age group of 30 children without fractures (Control group) whose parents consented to the study.
Exclusion criteria: Children on therapeutic vitamin D supplement, rickets, antiepileptic medication and chronic illness that can affect the bone density were excluded. Serial recruitment of consenting patients was done into the groups. Based on the inclusion criteria, only low and moderate energy causes of fractures were recruited.
Data collection was quantitative in nature. Children and their parent(s) or care provider(s) were interviewed as appropriate to obtain the socio-demographic data, anthropometric, mechanism of injury and other relevant clinical information. Moreover, antero-posterior and lateral view radiographs were obtained to characterize the fracture. Blood samples were collected and analysed using the direct Enzyme Link Immunosorbent Assay (Direct ELISA test kit: Accubind; Monobindinc. Lake Forest CA 92630, USA) technique to determine the value of the serum 25-hydroxyl vitamin D for each child that presented with forearm fractures and the controls without fractures. Closed reduction of the fracture was done and reduced fractures were retained in above elbow plaster cast. The patients were followed up in the clinic with serial plain radiographs, till union was achieved for an average of four to six weeks.
Statistical Analysis
Statistical analysis was performed using the IBM Statistical Package for the Social Sciences (SPSS) version 22. A pre-determined p-value of <0.05 was set for statistical significance corresponding to the confidence level of 95%. Univariate and multivariate analysis of variables was done. Also, multivariable logistic regression was performed to test for the association of fracture status with 25-hydroxyvitamin D levels while controlling for potential confounders based on previously published studies (age, sex, religion, body mass index percentile, outdoor playing time, month or season of the year) [7,13].
Results
A total of 60 patients were recruited; 30 patients with forearm fractures (study) and 30 patients without forearm fractures (control) groups. The mean age of the study group (5.4±1.9 years) and the control group (5.9±2.1 years) are comparable (p=0.299). Both the study and control groups have similar socio-demographic attributes as seen in [Table/Fig-1].
Socio-demographic characteristics of the patients.
| Characteristics | Study n (%) | Control n (%) | χ2 test |
|---|
| Sex |
| Male | 19 (63.3) | 17 (56.7) | p=0.278 |
| Female | 11 (36.7) | 13 (43.3) | p=0.598 |
| Total | 30 (100) | 30 (100) | |
| BMI percentile class |
| Underweight (<5th percentile) | 6 (20) | 5 (16.7) | LR=1.564 |
| Normal weight (5th-<85th percentile) | 22 (73.3) | 24 (80) | p=0.668 |
| Overweight (85th-<95th percentile) | 1 (3.3) | 0(0) | |
| Obese (>95th) Total | 1 (3.3) 30 (100) | 1(3.3) 30 (100) | |
| Age range (in years) |
| 0-4 | 10 (33.3) | 12 (40) | |
| 5-9 | 18 (51.4) | 17 (56.7) | LR=0.550 |
| 10 and above | 2 (6.7) | 1 (3.3) | p=0.759 |
| Religion |
| Christianity | 23 (76.7) | 23 (76.7) | χ2=0.000 |
| Islam | 7 (23.3) | 7 (23.3) | p=1.000 |
| Educational level |
| Pre-school | 5 (16.7) | 9 (30) | |
| Basic | 25 (83.3) | 20 (66.7) | LR=3.182 |
| Postbasic | 0 (0) | 1 (3.3) | p=0.212 |
| Total | 30 (100%) | 30 (100%) | |
χ2 test=Chi-square test; LR: Likelihood ratio
Majority of the patients are in the basic school (75%, n=45). Multivariate analysis of the educational level and the forearm status showed no statistical significance; (p=0.212). Majority of the patients are right-handed in both the study 27 (90%) and control 28 (93.3%) groups. All the left-handed patients 3 (10%) in the study group had a left forearm involvement. Multivariate analysis of handedness in the study group was statistically significant with a p-value of 0.019.
Majority of the forearm fractures occurred during the afternoon (53.3%) and evening (33.3%) period. Most of the fractures occurred between the 8th and the 10th month of the year. Most injuries occurred at home (60%) and mainly involved a fall on the outstretched hand (50%) [Table/Fig-2].
Characteristics of the forearm fracture in the study group.
| Characteristics | Frequency, n=30 (%) |
|---|
| Time of injury |
| Morning | 3 (10) |
| Afternoon | 16 (53.3) |
| Evening | 10 (33.3) |
| Night | 1(3.3) |
| Location of injury |
| Home | 18 (60) |
| School | 3(10) |
| Playground | 9 (30) |
| Mechanism of injury |
| Fall from height | 12 (40) |
| Direct trauma | 3 (10) |
| Fall on outstretched hand from ground level | 15 (50) |
| Degree of trauma |
| Low energy | 24 (80) |
| Moderate energy | 6 (20) |
| Involved forearm |
| Right | 17 (56.7) |
| Left | 13 (43.3) |
| Involved bone(s) |
| Radius | 7 (23.3) |
| Ulna | 4 (13.3) |
| Both | 19 (63.3) |
| Pattern of fracture |
| Transverse | 19 (63.3) |
| Oblique | 4 (13.3) |
| Comminuted | 2 (6.7) |
| Incomplete | 5 (16.7) |
| Level of fracture |
| Proximal | 9 (30) |
| Middle | 9 (30) |
| Distal | 12 (40) |
About 15 patients (50%) had fall on the outstretched hand at ground level accounting for the majority of the mechanisms of injury. Most fractured segment of the forearm is the distal portion which was recorded in 12 (40%) patients. With the likelihood ratio of 17.730, there was a high association between the mechanism of injury and the level of the fractured forearm (p=0.001). There was a slightly higher incidence of middle forearm fractures in girls compared to boys, but other levels of fractures are more common in boys than girls. However, this was not statistically significant (p=0.324) [Table/Fig-3].
Analysis of fracture level, sex and mechanism of injury.
| Variables | n=30(%) | Total | χ2 test |
|---|
| Involved forearm | Handedness in the study group | |
| Right | Left | | |
| Right | 17 (56.7) | 0 (0) | 17 (56.7) | LR=5.460p=0.019 |
| Left | 10 (33.3) | 3 (10) | 13 (43.3) |
| Total | 27 (90) | 3 (10) | 30 (100) |
| Level of injury | Mechanism of fracture n (%) | |
| Fall from height | Direct trauma | Fall on outstretched hand at ground level | |
| Proximal | 2 (6.7) | 1 (3.3) | 6 (20) | LR=17.730p=0.001 |
| Middle | 8 (6.7) | 1 (3.3) | 0 (0) |
| Distal | 2 (6.7) | 1 (1,1) | 9 (30) |
| Level of fracture | Sex distribution n (%) | |
| Male | Female | | |
| Proximal | 7 (23.3) | 2 (6.7) | 9 (30) | LR=2.253 p=0.324 |
| Middle | 4 (13.3) | 5 (16.7) | 9 (30) |
| Distal | 8 (26.7) | 4 (13.3) | 12 (40) |
| Total | 19 (63.3) | 11 (36.7) | 30 (100) | |
All the patients in the Control group had sufficient levels of serum 25(OH)D and only one patient (3.3%) in the study group had an insufficient level of vitamin D, 26.950 ng/mL. However, there was higher mean value in the control group compared to the study group which was found to be statistically significant [Table/Fig-4].
Mean serum 25 OH vitamin D levels in the two patient groups.
| Patient group | Serum Vitamin D levels | |
|---|
| Mean±SD (ng/mL) | Range (ng/mL) | |
|---|
| Control | 95.506±19.489 | 70.150–130.210 | F=2.962*p=0.001+(Independent t test) |
| Study | 60.751±15.041 | 26.950–85.045 |
*Independent samples T-Test, +statistically significant p-value at 95% confidence interval
In order to take into consideration of other potential confounders of forearm fractures in children like, the age, sex, outdoor playing time, religion, months of the year and body mass percentile; a logistic regression model was used. Only serum 25(OH)D level had a significant p-value (0.002). This shows that only 25(OH)D level has a strong correlation to the presence or absence of forearm fractures. Moreover, with a B (slope of the regression line) value of -0.177, signifies an inverse relationship between the serum 25(OH)D level and the risk of sustaining a forearm fracture; the higher the serum level of 25(OH)D, the lower the risk of paediatric forearm fracture. This is also buttressed by the odds ratio of less than 1 {(EXP(B)=0.838}, which translates to that for every one unit decrease in serum 25(OH)D level, there is about 16% chance of a child sustaining a forearm fracture [Table/Fig-5]. The fracture/recruitment of cases and controls in different months of the year is shown in [Table/Fig-6].
Logistic regression model of Serum vitamin D level, and other confounders to the presence or absence of forearm fracture.
| B* | p-value | Exp(B) | 95% CI for Exp(B) |
|---|
| Lower | Upper |
|---|
| Age | 0.184 | 0.590 | 1.202 | 0.615 | 2.351 |
| Sex (1) | 0.540 | 0.624 | 1.716 | 0.198 | 14.837 |
| EL (1) | -20.486 | 1.000 | - | - | |
| Religion | | 0.526 | 0.306 | 0.008 | 11.842 |
| BMIP | -1.184 | 0.740 | 0.993 | 0.951 | 1.036 |
| OPT | -0.007 | 0.519 | 2.090 | 0.222 | 19.647 |
| Vit D | 0.737 | 0.002+ | 0.838 | 0.751 | 0.935 |
| Months | -0.177 -0.024 | 0.860 | 1.024 | 0.784 | 1.339 |
EL: Educational level; BMIP: Body mass index percentile; OPT: Outdoor playing time; Vit D: Serum 25 OH vitamin D level; Months: Month of the year; +Significant p-values; B* Logistic Regression, Exp(B)- Odds ratio
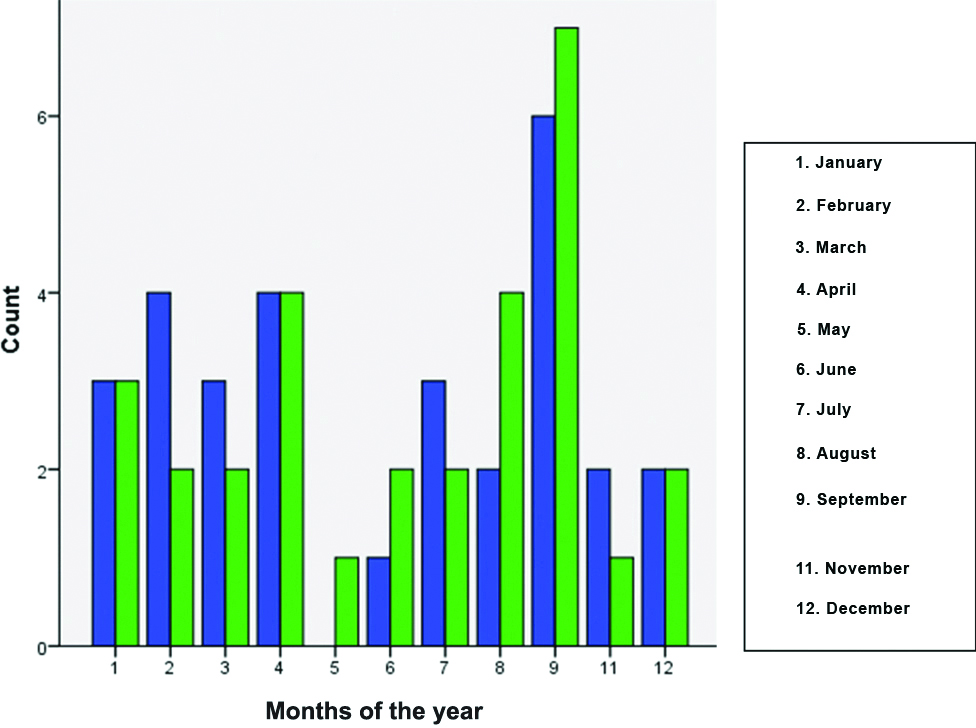
Months of the year of fracture/recruitment of cases and controls.
No recruitment was done in the 10th month (October)
Discussion
This study revealed the mean age of patients with forearm fracture to be similar to what was earlier found in Nigeria and Iran [2,3,14]. However, in a study in Washington, DC, Ryan et al found a slightly higher mean age value of 8.3±3.9 years [14]. Boys are usually more prone to suffer fractures globally, in particular, forearm fractures. Most series documented a higher percentage of forearm fractures in boys (between 58% to 70%) [2-4,13,15,16]. A similar proportion of boys were encountered in this study. Boys are more likely to engage in fracture prone activities than girls, however, this is not statistically significant (p>0.05).
The mean serum 25(OH)Vit D level in patients with forearm fractures were significantly lower compared with what was obtained in patients without fractures. Though these were still in the sufficient level range of serum vitamin D levels, this has a strong relationship as to the odds risk of having forearm fracture or not (p=0.002 and OR of 0.838). This implies that for every unit decrease in serum vitamin D level, there is a 16% increase in the risk of having forearm fracture. This mean value (60.751±15.041 ng/mL) obtained in this study is well above both insufficient and deficient range of serum vitamin D3. A study by Ryan LM et al., found a higher rate of low serum vitamin D level in both the cases and the control groups; 21.9±7.3 ng/mL and 22.6±7.2 ng/mL, respectively, while another study done in Egypt showed 33% of the children were found to have vitamin D insufficiency [15,16]. A significant association of serum vitamin D level and the odds ratio of having forearm fractures were found in these studies. However, a study from Iran found no significant relationship between the serum vitamin D level and the risk of having forearm fractures [14]. Though there was a higher prevalence of deficiency of serum vitamin D levels in both the cases and control groups 17.22±13.42 ng/mL and 17.88±11.21 ng/mL, respectively in the study.
The study by Saglam in Istanbul, Turkey has similar number of cases and controls similar to our study. However, they studied only distal forearm fractures in children aged 5 years to 10 years. They found a significantly lower vitamin D level in the children with fractures compared to those without, which is similar to our study. But, the mean serum vitamin D3 levels in both the cases and controls were in the insufficient/deficient range [17].
In a study that extended the age range to involve children younger than 18 years, the mean serum vitamin D was similar in the cases and control groups both falling within sufficient range (26.7 vs 25.45 ng/mL, p=0.84) [18]. They however, found that vitamin D sufficiency was not a significant predictor of fracture status [18]. In our study, mean serum levels of vitamin D in both case and control groups were within normal range, but significantly lower in children with forearm fractures. In contrast to their study, ours showed a positive relationship with forearm fractures as obtained in some other studies [7,17].
The abundance of sunshine in the tropical region of the study may be responsible for the higher mean value of serum vitamin D3 in this study in contrast to all the other studies done in temperate regions of the world. El- El-Sakka A et al., found four children with no sun exposure to have vitamin D deficiency and this underscores the importance of sun light exposure to vitamin D sufficiency [16].
This study showed that serum vitamin D3 level in children with forearm fractures is significantly lower than in children without forearm fractures despite the fact that both values are within the acceptable normal range as documented in the literature [7,16,17]. Higher values of serum vitamin D3 seems to be protective against fractures. Children with low energy fractures should be evaluated for evidence of hypovitaminosis D3 and treated if they are found to be deficient. Minkowitz B et al., found that lower vitamin D level in children predicts severe fractures and proposed a target of at least 40 ng/mL as against the 30 ng/mL currently in use for the treatment of such children under the age of 18 years [19]. The findings from this study raises a question and points to the fact that the cut-off level of adequacy or otherwise of vitamin D3 may defer from region to region in the world.
Limitation(s)
The present study was conducted in one region only, a multi-regional and multi-racial spread would have been ideal.
Conclusion(s)
Children with forearm fracture have relatively lower serum vitamin D3 levels with correspondingly increased odd risk of sustaining forearm fractures than children with no forearm fracture.
χ2 test=Chi-square test; LR: Likelihood ratio
*Independent samples T-Test, +statistically significant p-value at 95% confidence interval
EL: Educational level; BMIP: Body mass index percentile; OPT: Outdoor playing time; Vit D: Serum 25 OH vitamin D level; Months: Month of the year; +Significant p-values; B* Logistic Regression, Exp(B)- Odds ratio