Metastatic Carcinoma Breast Presenting as Appendicular Abscess: A Case Report
Meenakshi Yeola (Pate)1, Kushagra Singh2, Darshana Tote3, Azeem Javed Aalam4, Pankaj Gharde5
1 Professor and Head, Department of Surgery, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
2 Postgraduate Student, Department of Surgery, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
3 Professor, Department of Surgery, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
4 Postgraduate Student, Department of Surgery, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
5 Professor, Department of Surgery, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kushagra Singh, Postgraduate Student, Department of Surgery, AVBRH, JNMC, DMIMS, Sawangi (M), Wardha, Maharashtra, India.
E-mail: dr.kushagrasingh@gmail.com
Breast cancer is the most common cancer in females worldwide and presents mostly as a hard painless lump in the breast. Authors report a case of a 59-year-old female who presented to emergency department with complaints of pain and lump in right iliac fossa, high grade fever with chills and rigor, multiple episodes of vomiting. She was febrile having tachycardia with normal blood pressure. Examination revealed a firm tender lump in right iliac fossa with guarding of abdomen. Incidental finding of a large left sided breast lump was noted. Radiological investigations revealed appendicular abscess. She was undertaken for emergency diagnostic laparoscopy followed by appendectomy. Surprisingly, histopathology revealed deposits of ductal carcinoma in appendix. She developed a faecal fistula at the incision site. On further evaluation of left breast lump, it was diagnosed as a locally advanced breast carcinoma. Patient was managed with neoadjuvant chemotherapy followed by left sided Modified Radical Mastectomy (MRM) and adjuvant chemotherapy. She was on regular follow-up since then. Appendicular metastasis is one of the rare sites of metastasis of breast malignancy and presentation as appendicular abscess made the diagnosis and management challenging.
Appendicitis, Appendix, Cancer, Malignancy, Metastasis
Case Report
A 59-year-old female presented to emergency department of tertiary care hospital at midnight with complaints of pain and lump in right iliac fossa, high grade fever with chills and rigor since two weeks and multiple episodes of vomiting since two days. There was no history of any chronic illness or previous operative interventions. On examination the patient was febrile with 101°F temperature, pulse was 120/min with a blood pressure of 116/74 mmHg. Per abdomen examination revealed a firm, tender lump in right iliac fossa with guarding of abdomen. Systemic examination revealed incidental findings of a large lump in left breast, approximate size of 6x6 cms involving all quadrants of left breast. It was non-tender with no local rise in temperature, firm in consistency, had smooth surface and was mobile. The skin overlying the lump was normal. There was an ipsilateral axillary lymphadenopathy with a single node palpable which was non-tender, firm in consistency and mobile. On evaluation contralateral breast and axilla were normal.
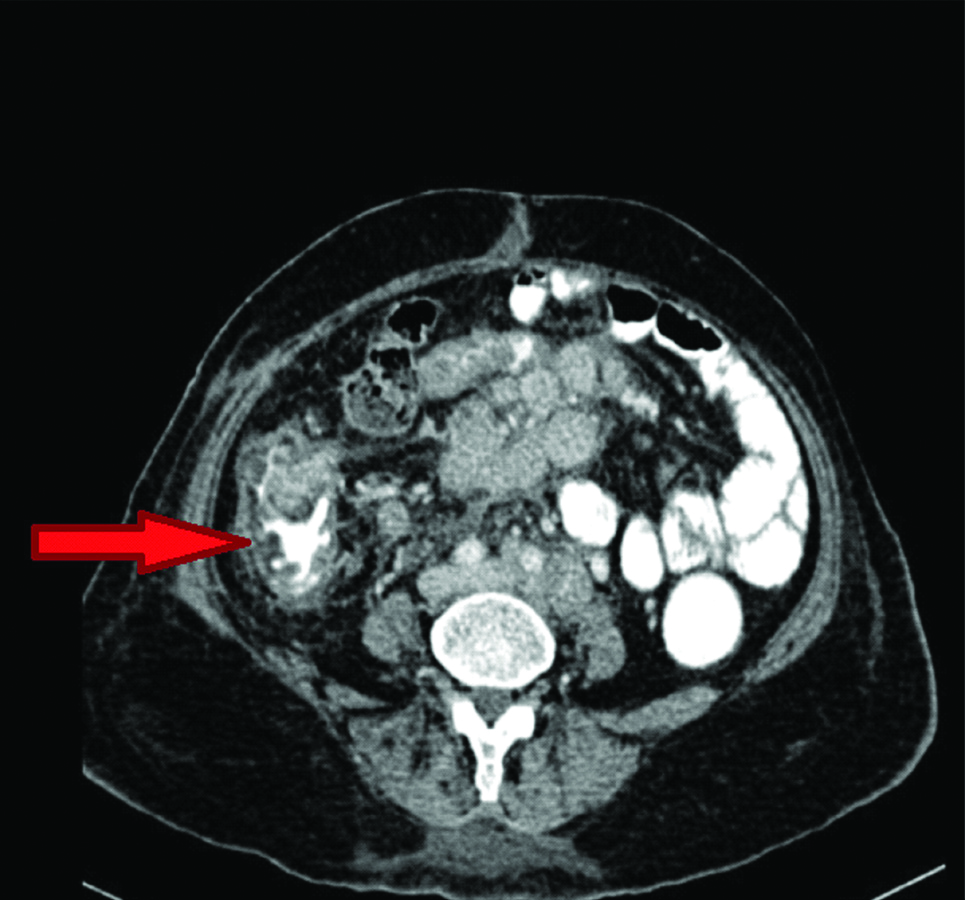
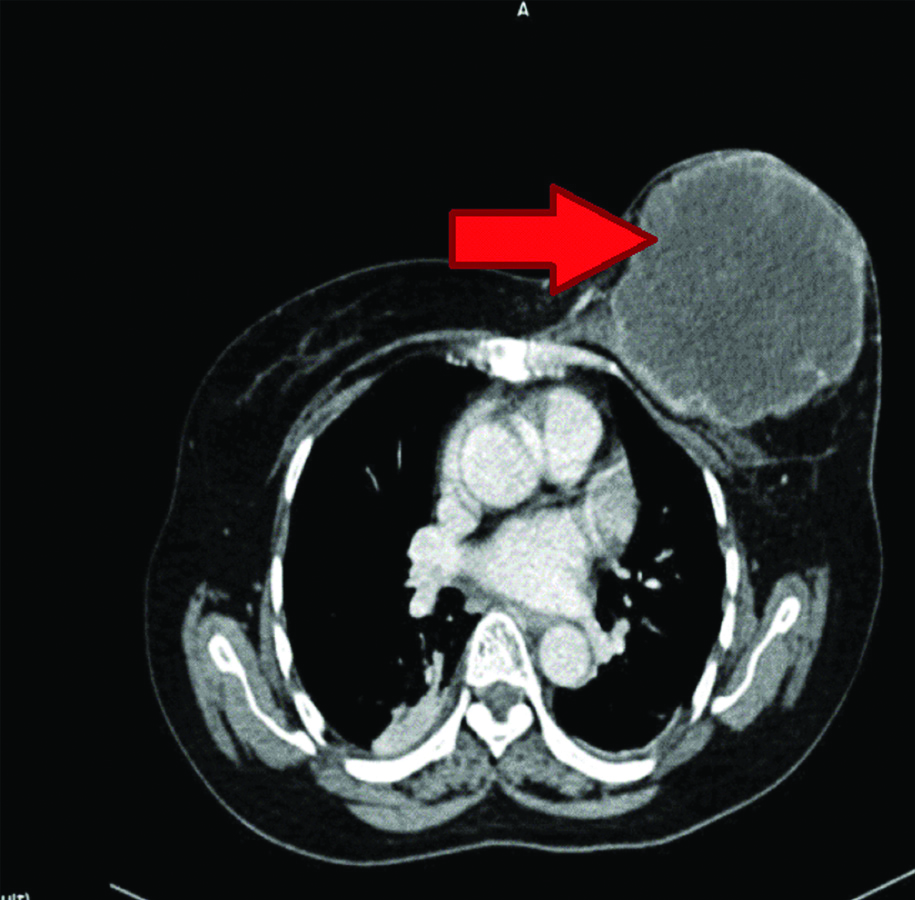
An ultrasonography (USG) of abdomen and pelvis was done a day before which was suggestive of right adnexal mass with free fluid in pelvis. Patient was admitted under Gynaecology Department and a repeat USG revealed a hypoechoic lesion of size 23×20 mm in medial wall of caecum with associated abscess in right iliac fossa, multiple retroperitoneal lymph nodes (largest of 25×25 mm), mesenteric and right iliac lymphadenopathy. For further evaluation a Contrast-Enhanced Computed Tomography (CECT) scan of abdomen and pelvis was done which was suggestive of appendicular abscess with extensive intra-abdominal lymphadenopathy and free fluid in pelvis [Table/Fig-1]. Thoracic cuts of CECT revealed a large lump in left breast (Breast Imaging Reporting and Database System score (BIRADS) IV-V [Table/Fig-2]) [1]. Patient was transferred to Department of Surgery for further management.
CECT Abdomen showing abscess in region of appendix.
Thoracic cuts of CECT showing large left sided breast lesion (BIRADS IV-V).
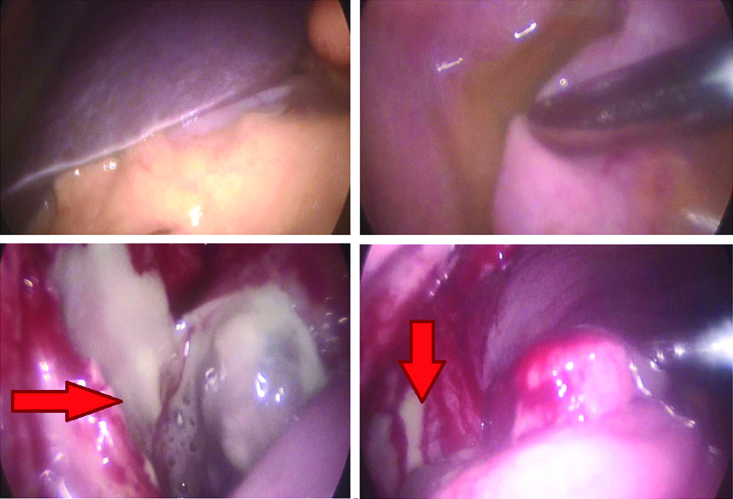
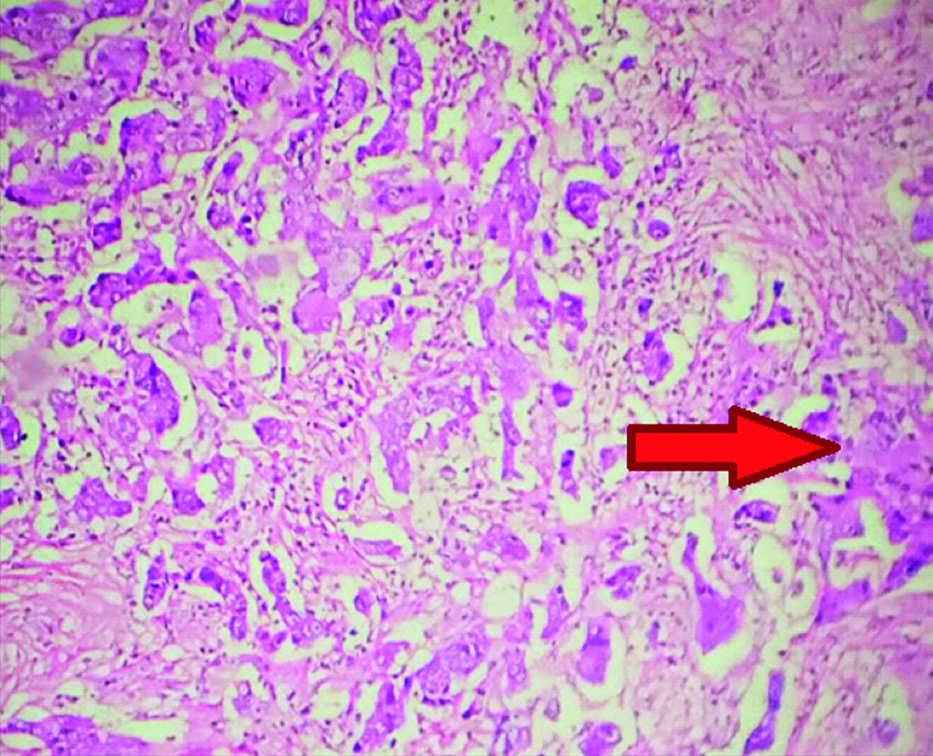
Haematological investigations revealed an elevated leucocyte count of 18000 cells/mm3. As the patient presented with features of appendicular abscess, it was given priority over the breast lump. Patient was undertaken for emergency diagnostic laparoscopy. Intra-operatively there was appendicular abscess with adhesions in right iliac fossa [Table/Fig-3]. Abscess was drained and laparoscopic appendectomy was attempted but adhesiolysis resulted in multiple small ileal perforations. The procedure was converted to open surgery through grid-iron incision and appendectomy was done with repair of ileal perforation. Post-operatively patient’s vitals stabilised. But she developed a faecal fistula through the grid-iron incision. The histopathology report surprisingly revealed deposits of ductal carcinoma with desmoplastic reaction in the body of appendix with acute inflammatory changes with leucocytic infiltration [Table/Fig-4,5]. Tumor markers CA-125 was raised (198.4 U/mL) and Carcinoembryonic Antigen (CEA) was normal (0.7 nG/mL).
Intraoperative images showing appendicular abscess with pus in pelvis (red arrows).
Showing ductal deposits in appendix (H&E,10X).
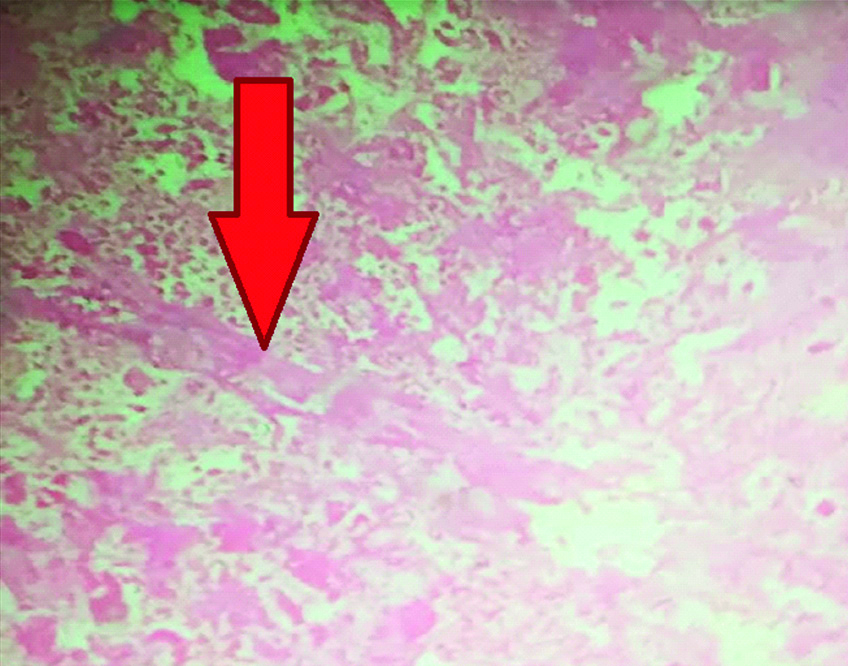
Showing ductal deposits in appendix (H&E,40X).
On further evaluation, USG and Fine Needle Aspiration Cytology (FNAC) from left breast lump revealed ductal malignancy. As the patient was having locally advanced breast carcinoma, she was subjected to neoadjuvant chemotherapy in the form of Adriamycin + Cyclophosphamide (AC)+paclitaxel regimen. After two cycles of chemotherapy, the faecal fistula healed completely. Postoperative formation of faecal fistula from incision site was in favour of malignancy and the miraculous cessation of fistula after chemotherapy for breast carcinoma further confirmed that the metastasis to appendix were of ductal origin. Following which she underwent left sided RM. Histopathology from left MRM specimen came out to be infiltrating ductal carcinoma with triple negative status. Postoperatively she was given adjuvant chemotherapy in the form of AC+paclitaxel regimen and radiotherapy. She became asymptomatic and is on close follow-up since past two years with no recurrence or new metastasis of breast cancer.
Discussion
Breast cancer accounts to approximately 25% of all the cancers and is the most common female cancer worldwide with an estimated 1.6 million new cancer cases diagnosed annually. In India, incidence rate of breast cancer is 25.8 per 100,000 with mortality rate of 12.7 per 100,000 [2,3]. Distant metastasis of breast carcinoma presenting as first presentation is uncommon [4-6]. Infiltrating ductal carcinomas of breast usually tend to metastasise to more common sites such as bone, lung and liver [7]. Spread of carcinoma breast to appendix is documented in only few literatures [7-10]. Numan L et al., reported a case of previously diagnosed Stage IV breast carcinoma who presented with acute appendicitis and small bowel obstruction three years after the diagnosis. Intraoperative presence of peritoneal deposits lead to suspicion of metastasis of breast carcinoma [7]. A right hemicolectomy was performed for the same. Araujo JL et al., reported a case of breast carcinoma with metastasis to ovary and appendix resulting in acute appendicitis and subsequent abscess [8]. Kwan E et al., reported a case of previously diagnosed metastatic breast carcinoma on chemotherapy presenting with acute appendicitis. [9] Mori R et al., also reported a similar case previously diagnosed stage IV breast carcinoma with metastasis to appendix [10]. In present case appendicitis with appendicular abscess was the presenting feature and considering the haemodynamic instability the patient was undertaken for exploration before the histopathology of breast lump arrived. Intraoperatively there were no peritoneal deposits or other features of metastasis hence, only appendectomy was done. Previously diagnosed breast carcinoma or features of metastasis intraoperatively would have warranted a hemicolectomy with clear margins and it would have been a better choice.
Appendicitis is a common cause of right iliac fossa pain. Other causes of right iliac fossa pain and tenderness include right sided ureteric colic, colitis, Meckel’s diverticulitis, irritable bowel syndrome, right sided haemorrhagic ovarian cyst, pelvic inflammatory disease and other rare causes [11]. Appendicitis can be clinically diagnosed with a history of pain around the umbilicus later migrating to McBurney’s point. Other features include rebound tenderness, vomiting and tachycardia. A ultrasonography or CECT abdomen confirms the diagnosis [11]. Connor SJ et al., reported that appendicular tumor after emergency appendectomy has a very low incidence of only 0.9% and even rarer is to find metastatic lesions in appendix which account for only 14.8% of the above [12]. The proposed pathophysiology for appendicular metastasis is that the metastatic cells deposit in the serosa of the appendix which then progress to infiltrate the lumen ultimately causing luminal obstruction. This results in acute inflammation of appendix. Unchecked inflammation may result in abscess, perforation and ultimately perforation peritonitis [13].
The patient can present with nausea, vomiting, anorexia, and right lower abdominal pain. Physical examination may reveal fever and localised right iliac fossa tenderness. Patients may or may not have leukocytosis. CT abdomen and pelvis is the choice of radiological investigation. Salient features of acute appendicitis on CT include thickened appendiceal wall, peri-appendiceal fat stranding, appendiceal wall enhancement, and a calcified appendicolith in up to 30% of the patients [14].
As the patient presented with features of appendicular abscess, it was given priority over the breast lump. The histopathology report of ductal metastasis in appendix came out to be surprising. Cytology from left breast lump also confirmed ductal malignancy. Postoperative formation of faecal fistula from incision site was in favour of malignancy and the miraculous cessation of fistula after chemotherapy for breast carcinoma further confirmed the possibility of metastasis of breast carcinoma to appendix. Post-chemotherapy the patient was asymptomatic and was on regular follow-up since two years.
Conclusion(s)
Breast carcinoma is a systemic disease and this unusual case confirms it. Further studies are required for formulating a protocol for the management of similar cases. The recurrence rate and five-year survival rate have also not been defined which makes prognosis difficult to understand and communicate. High index of suspicion, thorough history and clinical examination and possibility of rare aetiologies for appendicitis should be considered while deciding the line of management and a wider dissection (hemicolectomy) should be considered.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Apr 08, 2020
Manual Googling: Jul 23, 2020
iThenticate Software: Dec 18, 2020 (8%)
[1]. D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA, ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System 2013 Reston, VAAmerican College of Radiology [Google Scholar]
[2]. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012Int J Cancer 2015 136(5):E359-86.10.1002/ijc.2921025220842 [Google Scholar] [CrossRef] [PubMed]
[3]. Gupta A, Shridhar K, Dhillon PK, A review of breast cancer awareness among women in India: Cancer literate or awareness deficit?Eur J Cancer 2015 51(14):2058-66.10.1016/j.ejca.2015.07.00826232859 [Google Scholar] [CrossRef] [PubMed]
[4]. Martins Figueiredo L, Horta DV, Reis JA, A rare presentation of breast cancerGE Port J Gastroenterol 2019 26(6):438-40.10.1159/00049704331832500 [Google Scholar] [CrossRef] [PubMed]
[5]. Li L, Secondary Parkinson disease caused by breast cancer during pregnancy: A case reportWorld J Clin Cases 2019 7(23):4052-56.10.12998/wjcc.v7.i23.405231832408 [Google Scholar] [CrossRef] [PubMed]
[6]. Mosiun JA, Idris MSB, Teoh LY, Teh MS, Chandran PA, See MH, Gastrointestinal tract metastasis presenting as intussusception in invasive lobular carcinoma of the breast: A case reportInt J Surg Case Rep 2019 64:109-12.10.1016/j.ijscr.2019.10.00331629292 [Google Scholar] [CrossRef] [PubMed]
[7]. Numan L, Asif S, Abughanimeh OK, Acute appendicitis and small bowel obstruction secondary to metastatic breast cancerCureus 2019 11(5):e470610.7759/cureus.4706 [Google Scholar] [CrossRef]
[8]. Araujo JL, Cavalcanti BSM, Soares MCDV, Sousa UW, Medeiros GPD, Metastases of breast cancer causing acute appendicitis: A case reportCancer Rep Rev 210.15761/CRR.1000155 [Google Scholar] [CrossRef]
[9]. Kwan E, Houli N, Pitcher M, Wong S, Appendiceal metastasis in a patient with advanced breast cancer on hormonal therapyInt J Cancer Clin Res3:05910.23937/2378-3419/3/3/1059 [Google Scholar] [CrossRef]
[10]. Mori R, Futamura M, Morimitsu K, Yoshida K, Appendicitis caused by the metastasis of HER2-positive breast cancerSurg Case Rep 2016 2(1):10410.1186/s40792-016-0235-527683008 [Google Scholar] [CrossRef] [PubMed]
[11]. Agrawal A, Govil A, Lakdawala M, Unusual case of right iliac fossa pain: A case reportJournal of Mahatma Gandhi Institute of Medical Sciences 2015 20(1):9410.4103/0971-9903.151742 [Google Scholar] [CrossRef]
[12]. Connor SJ, Hanna GB, Frizelle FA, Appendiceal tumors: Retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomiesDis Colon Rectum 1998 41(1):75-80.10.1007/BF022368999510314 [Google Scholar] [CrossRef] [PubMed]
[13]. Capper RS, Cheek JH, Acute appendicitis secondary to metastatic carcinoma of the breastAMA Arch Surg 1956 73:220-23.10.1001/archsurg.1956.0128002003400713354113 [Google Scholar] [CrossRef] [PubMed]
[14]. Whitley S, Sookur P, McLean A, Power N, The appendix on CTClin Radiol 2009 64:190-99.10.1016/j.crad.2008.06.01519103350 [Google Scholar] [CrossRef] [PubMed]