The majority of Iran’s population is comprised of Muslims who fast during the holy month of Ramadan [1,2]. Fasting during Ramadan is one of the obligatory duties of healthy people. Eating, drinking, and using oral medications is not allowed during fasting from dawn to sunset (when the fast is broken, also known as Iftar) [3,4]. The religion of Islam has exempted people with chronic and morbid diseases from this duty as well as when fasting is considered hazardous for their health [5]. However, most diabetic patients tend not to accept their condition and are willing to fast [6], even though it is not clear whether fasting is harmful or has positive effects on their health. A large sample study (12,914 people) in 13 Muslim countries has shown that approximately 43% of type I and 79% of type II diabetic patients fast for at least 15 days during Ramadan with the proportion of subjects fasting for at least 15 days ranged from 57.8% in Turkey to 89.8% in Malaysia and Bangladesh [7].
Fasting has a direct impact on diabetes control by effecting a change in lifestyle, meal intervals, type of food, and medication timing [3]. Insufficient metabolic control increases the risk of complications in diabetic patients and fasting in high-risk diabetics may lead to hypoglycaemia, hyperglycaemia, dehydration, or diabetic ketoacidosis [7,8]. New eating patterns, due to fasting, increases the hypoglycaemia risk, 4.7 and 7.5 times in type I and type II diabetic patients, respectively. It also increases the risk of hyperglycaemia in type II diabetes by up to five times [9]. On the other hand, many studies have revealed that diabetic patients with good glycaemic control before Ramadan had uncomplicated fasting [3,5,10-12]. Diabetic subjects who desire to fast should be well instructed regarding their physical activity, eating patterns, regular blood glucose monitoring, dose, and timing of medications.
Primary care practitioners and family physicians have an important role in providing information, implementing guidelines, and enhancing diabetic patients’ care [13]. On the other hand, improper fasting and not eating food at dawn, iftar, and dinner can worsen blood sugar control in diabetic patients after the end of Ramadan [14]. The effect of fasting on sugar control has been seen in many studies, but there are also contradictory results in this regard [15-18]. In this study, in addition to blood sugar, Authors examined the effects of fasting on anthropometric indices, especially the conicity indices (abdominal obesity index), which is currently the most valuable index for assessing abdominal obesity [19,20]. Because obesity and even improper distribution of fat in different parts of the body can be effective in controlling blood sugar [21,22].
The current study aimed to investigate the effect of fasting during Ramadan on metabolic and anthropometric parameters in type II diabetic patients who were consulted by family physicians and had good blood glucose control before Ramadan.
Materials and Methods
This prospective observational study was conducted during Ramadan 2018 (17th May 2018-25th June 2018). The study population comprised of 45 diabetic patients. Patients who attended the academic outpatient diabetes clinics of Mazandaran University of Medical Sciences in Sari, Iran were enrolled in the study. The study was approved by the Imam Khomeini Hospital-Mazandaran University of Medical Sciences Ethics Committee (Approval ID: IR.MAZUMS.IMAMHOSPITAL.REC.1398.067). Written informed consent was obtained from all participants. The mean changes in blood sugar after fasting were used to calculate the sample size based on the results of a previous study in Iran [23], the following equation was employed for sample size calculation:
Alpha=0.05, Beta=0.20
Expected mean difference=20 mg/100, Expected standard deviation of difference=25,
The sample size of at least 27 people was calculated.
Inclusion criteria: The diabetes type II patients diagnosed for at least one year with HbA1c ≤8% and desire to fast during Ramadan.
Exclusion criteria: Patient with severe chronic diseases (kidney, liver, and heart failure based on patients’ medical records), a recent history of hypoglycaemia, pregnancy, uncontrolled hypertension (up to 160 mmHg systolic or up to 100 mmHg diastolic blood pressure), smoking, use of medications that affect blood glucose or lipid profile (such as corticosteroids, Oral Contraceptive Pills (OCP)), and fasting less than 15 days during Ramadan.
Finally, a total of 40 people remained in the study, which included 33 (82.5%) females and 7 (17.5%) males.
Demographic variables such as age, gender, occupation and education level were derived from patients’ records and updated in their first visit.
Laboratory data such as level of Thyroid Stimulating Hormone (TSH), Aspartate Transaminase (AST), Alanine Transaminase (ALT), Alkaline Phosphatase (ALP), Blood Urea Nitrogen (BUN), and Creatinine (Cr) were extracted from patients’ last measurement in their medical records. For all participants, baseline blood glucose profile (FBG, 2h PPG, HbA1c) and lipid profile {cholesterol, High-Density Lipoprotein-Cholesterol (HDL-C), Low-Density Lipoprotein-Cholesterol (LDL-C), Triglyceride (TG)}, were evaluated one month before Ramadan. Fasting venous blood samples (7cc) were collected from all the patients before Iftar on the 15th and the last day of Ramadan and blood glucose profiles were tested using Pars Azmoon Kit, Iran, and 24i Auto Analyser, Japan. Fasting lipids profiles were evaluated on the last day of Ramadan. Patients were requested to test their 2h PPG (two hours after Iftar) at home using a glucometer (CONTOURTM PLUS glucometer from Bayer, Germany, Damoun Tajhiz Teb Company).
Before fasting, patients were advised to eat food at dawn, iftar and dinner during Ramadan, but not to change their diet and activities during fasting. In order to accurately record the number of days the participants fasted, a timetable was given to all patients.
Height, weight, waist circumference, and hip circumference were measured before and after Ramadan. Clara 803 cluster digital balance scale, with a precision of 0.01 g, was used to weigh the patients. Height was measured using a Seca stadiometer without shoes with a sensitivity of 0.1 cm (Seca, Germany). Waist and hip circumference was measured using Seca strip model 201. All anthropometric measurements were performed according to the methodology provided by the World Health Organisation (WHO) standards [24]. During the study, the anthropometric indices were measured twice and the mean of the two measurements was entered. BMI of the individuals was also obtained using the relevant formula (BMI=(weight (kg))/{height (m)2}) [25]. The Waist-To-Hip Ratio (WHR) was calculated by dividing the waist circumference into the hip [26]. The conicity index, which is a marker for central obesity, has also been estimated in the following way before and after Ramadan [27].
Blood Pressure (BP) (using Riester BP device, Germany) was measured twice for each patient by a qualified nurse practitioner in the clinic. The type and dosage of anti-diabetic drugs were adjusted and the instructions for using the medications were explained to each patient according to the Ramadan fasting guidelines [6].
The participants were free to attend one of the 4 sessions of training programs that were held before Ramadan. The duration of each session was 3 hours and the duration of consultation for each patient lasted an average of 40 minutes. Every participant was visited by the research team to adjust their medication dosage and was given counselling about lifestyle changes.
The internal medicine specialist instructed patients on how to use their medications during the fasting period. The research fellow, family physician resident, explained to each patient individually about Self-Monitoring Blood Glucose (SMBG), hypo and hyperglycaemia symptoms, and home management of hypoglycaemia in addition to the conditions where fasting should be stopped. For this purpose, a CONTOUR™ PLUS meter and required strips were provided for every participant to help them test with ease. All the patients were trained to perform SMBG and recommended to measure their blood glucose 4 times a day (before and 2 hours after Iftar and dawn and any time there were signs of hypoglycaemia). Patients were advised to break their fast if their blood glucose was below 70 mg/dL or higher than 250 mg/dL during fasting. The family physician contacted all patients on the 15th and 29th of Ramadan for any questions or problems while fasting and also to remind them to perform the laboratory and SMBG tests. To facilitate contact with the family physician, a full-time telephone line was available for the patients.
Statistical Analysis
Descriptive statistics including percentages and frequencies were reported using demographic data. The normal distribution of variables was checked using the One-Sample Kolmogorov-Smirnov Normal Test. Paired samples test was employed for statistical analysis and the significance level was considered p<0.05. All statistical analyses were performed using SPSS software (version 24, IBM SPSS Statistics, Chicago, IL).
Results
Patient demographics and attributes are presented in [Table/Fig-1]. Out of the 40 study participants, there were 33 (82.5%) females and 7 (17.5%) males. A large majority (n=29; 72.5%) of the study subjects fasted for 30 days. No episode of hypoglycaemia was reported.
Patient demographics and attributes.
| Patient characteristics | All (n=40) |
|---|
| Gender | Male | 7 (17.5%) |
| Female | 33 (82.5%) |
| Age (year) (Mean±SD) | 55.23±9.29 |
| Job | Freelance | 2 (5%) |
| Employed | 4 (10%) |
| Housekeeper | 30 (75%) |
| Retired | 4 (10%) |
| Education | Illiterate | 9 (22.5%) |
| Under diploma | 19 (47.5%) |
| Diploma and higher | 12 (30.0%) |
| Laboratory data (Mean±SD) | AST (IU/L) | 19.68±9.22 |
| ALT (IU/L) | 22±14.43 |
| ALP (IU/L) | 173.95±52.12 |
| BUN (mg/dL) | 23.6±9.29 |
| Cr (mg/dL) | 0.92±0.18 |
| TSH (mIu/mL) | 2.13±1.1 |
| Duration of diabetes (years) (Mean±SD) | 7.5±6.35 |
| Medication | Metformin | 38 (95%) |
| Gliclazide | 22 (55%) |
| Repaglinide | 3 (7.5%) |
| Acarbose | 10 (25%) |
| Insulin | 1 (2.5%) |
| losartan | 12 (30%) |
| Metoral | 7 (17.5%) |
| Atorvastatin | 26 (65%) |
| ASA | 17 (42.5%) |
Thyroid stimulation hormone (TSH), Aspartate transaminase (AST), Alanine transaminase (ALT), alkaline phosphatase (ALP), Blood urea nitrogen (Bun), creatinine (Cr) and Acetyl Salicylic Acid (ASA)
Anthropometric variables of patients showed in [Table/Fig-2], including weight (pre: 74.9±12.7 vs. post-ramadan: 73.0±13.1 kg, p<0.001), BMI (pre: 29.9±5.2 vs. post-ramadan: 29.0±5.1 kg/m2, p=0.042), waist circumference (pre: 106.2±11.8 vs. post-ramadan: 105.3±11.6 cm, p<0.001), conicity index (pre: 9.94±0.96 vs post-ramadan: 9.80±0.99, p=0.085), systolic BP (pre: 118.5±10.6 vs. post-ramadan: 113.8±9.4 mmHg, p=0.018) and Diastolic blood pressure (pre: 72.0±7.9 vs. post-ramadan: 68.3±7.0 mmHg, p=0.02). For other variables such as conicity index, HbA1c, and 2h PPG changes were not statistically significant p>0.05 [Table/Fig-2,3].
Anthropometric data of 40 Type II diabetic patients before and after fasting.
| Variable | Pre-Ramadanmean±SD | Post-Ramadanmean±SD | Paired t-test value and p-value |
|---|
| Body Mass Index (BMI)(kg/m2) | 29.9±5.2 | 29.0±5.1 | t=2.100 and p=0.042* |
| Weight (kg) | 74.9±12.7 | 73. 0±13.1 | t=5.679 and p=0.0001** |
| Systolic blood pressure (mmHg) | 118.5±10.6 | 113.8±9.4 | t=2.481 and p=0.018* |
| Diastolic blood pressure (mmHg) | 72.0±7.9 | 68.3±7.0 | t=2.420 and p=0.02* |
| Waist to hip ratio | 0.98±0.05 | 0.97±0.04 | t=4.454 and p=0.0001** |
| Waist circumference (cm) | 106.2±11.8 | 105.3±11.6 | t=4.095 and p=0.0001** |
| Conicity index | 9.94±0.96 | 9.80±0.99 | t=-1.768 and p=0.085 |
p<0.05* statistically significant; p<0.001** statistically highly significant; Paired Samples Test
Glycaemic profile before, on the fifteenth day, and the end of Ramadan. paired sample t-test.
| Patient parameters | Pre-Ramadan | Mid-Ramadan | Post-Ramadan |
|---|
| Mean±SD | Mean±SD | Mean±SD |
|---|
| 2h PPG (mg/dL) | 180.8±51.7 | 176.1±62.0 | 178.6±60.5 |
| HbA1c | 6.3±0.7 | Not measured | 6.5±0.7 |
Comparison of all measurements (pre vs mid/post and mid vs post) were statistically nonsignificant, p>0.5; PPG: Post-prandial glucose
The changes in glycaemic profile during Ramadan are listed in the [Table/Fig-3].
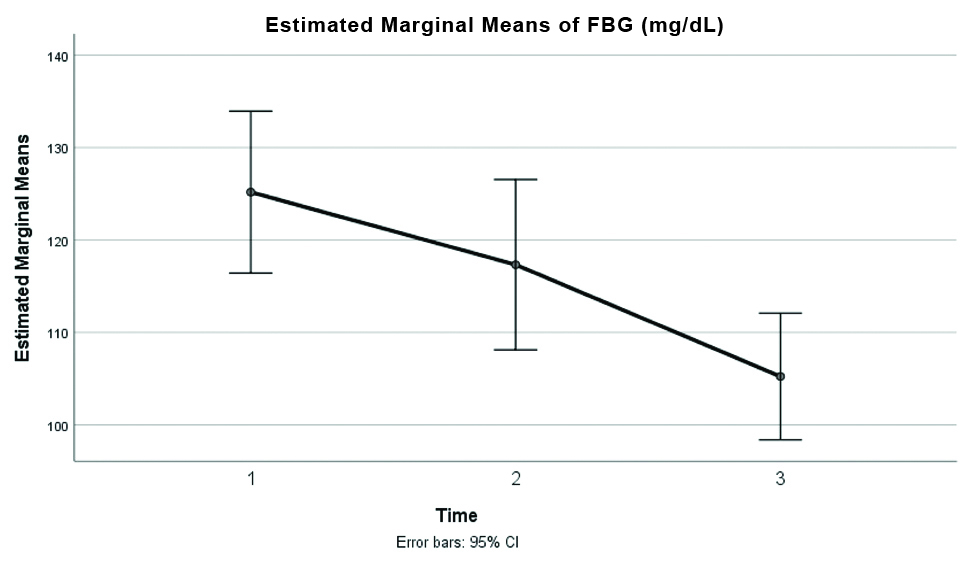
As shown in [Table/Fig-4,5], the FPG trend decreased during the three-time points (pre: 125.1±27.4, mid 117.3±28.8, post-ramadan: 105.2±21.4 mg/dL and was statistically significant between pre and post-Ramadan (p<0.001) and mid Ramadan and post-Ramadan (p=0.005).
Estimated marginal means of FBG in three-time points during the study period (pre, mid and post-Ramadan), p-value < 0.001**, The mean and standard deviation were 125.1±27.4, 117.3±28.8, and 105.2±21.4, respectively. FBG: Fasting blood glucose
Pairwise comparisons of FBG during the study period based on the estimated marginal means.
| FBG Measurements | Mean (mg/dL) | SD | Pair t-test value | p-value |
|---|
| Pre-Ramadan | 125.18 | 27.421 | 1.930 | 0.061 |
| Mid- Ramadan | 117.32 | 28.804 |
| Pre-Ramadan | 125.18 | 27.421 | 5.230 | <0.001** |
| Post-Ramadan | 105.23 | 21.427 |
| Mid- Ramadan | 117.32 | 28.804 | 3.014 | 0.005* |
| Post-Ramadan | 105.23 | 21.427 |
p<0.05* statistically significant
p<0.001** statistically highly significant
Paired Samples Test
Lipid profiles before and after fasting shown in [Table/Fig-6] demonstrated a significant increase in TG (127.5±45.5 vs. 166.5±53.5 mg/dL, p<0.001. None of the other components of the lipid profile showed a significant difference before and after fasting.
Lipid profile before and after fasting for 40 type II diabetic patients.
| Lipid profile | Pre-Ramadanmean±SD | Post-Ramadan mean±SD | Paired t-test value and p-value |
|---|
| TG mg/dL | 127.5±45.5 | 166.5±53.5 | t= -4.586 and p<0.001** |
| Cholesterol mg/dL | 154.8±29.0 | 157.9±39.6 | t= -0.527 and p=0.601 |
| HDL-c mg/dL | 41.8±7.0 | 40.0±6.2 | t=1.768 and p=0.085 |
| LDL-c mg/dL | 81.9±21.5 | 88.2±29.2 | t= -1.504 and p=0.141 |
p<0.05* statistically significant; p<0.001** statistically highly significant; Paired Samples Test; TG: Triglycerides; HDL-c: High density lipoprotein-cholesterol; LDL-c-: Low density lipoprotein-cholesterol
Discussion
In this study, the effects of fasting on metabolic and anthropometric indices in type II diabetic patients were investigated during Ramadan. Participants were given appropriate instructions on lifestyle, medication, and physical activity.
The results of the present study showed that patients’ BMI, weight, systolic and diastolic blood pressures, WHR, and waist circumference, reduced significantly after one month of fasting (p-value<0.05). Similar results were demonstrated in a study by Paul AK et al., in which all the participants had to fast a minimum of 25 days. The findings showed that the mean weight of 52 diabetic patients decreased significantly during Ramadan after one month fasting (p-value <0.001) [28]. In a study conducted by Bravis V et al., an average weight loss of 0.7 kg occurred in the intervention group vs. 0.6 kg in the control group after Ramadan (p-value <0.001) [29]. McEwen LN’s study also showed a significant decrease in BMI and weight in the intervention group (pre: -1.1±2.4 kg/m2 vs. post-ramadan: -0.2±1.7 kg/m2, p<0.0001) [30]. Moreover, in Khaled BM and Belbraouet S study on anthropometric parameters and food consumption in 276 type II diabetic obese women in Algeria showed a significant decrease in weight at the end of Ramadan (p<0.01) [3].
Another study by Nachvak SM et al., on the effects of Ramadan in food intake, body composition, glucose homeostasis, and lipid profiles showed a significant decrease in blood glucose, BMI, and weight at the end of Ramadan (all p <0.001). Evaluation of food intake of various food groups showed that the consumption of food groups other than carbohydrates had decreased during Ramadan. The results of Nachvak SM et al., study are consistent with findings of the present study, except the triglyceride level which was increased significantly (p <0.001) [17].
Yarahmadi S et al., studied anthropometric and biochemical variables of 57 type II diabetic patients during Ramadan. Their results indicated that BMI and WHR reduced in men (p<0.01) but BMI increased in women (p<0.03). On the other hand, BP, FPG, and serum fructosamine concentrations did not change during the study, whereas total cholesterol, LDL concentrations were significantly increased in all patients (p<0.03) [31]. In this study, the conicity indices, indicating central obesity and distribution of fat in the body, decreased after Ramadan but the results were not statistically significant.
The Conicity indices is used to measure abdominal obesity and its functional value is higher than the waist [20]. This indicator is used to determine abdominal obesity and fat distribution in the body, and focuses on more central obesity than general obesity, which this research found, they are different in central obesity in diabetic patients before and after Ramadan. Therefore, it is possible that fasting in diabetic patients can reduce the risk of many diabetic complications, including cardiovascular disease, by reducing anthropometric indices, especially conicity indices (abdominal obesity) [19].
In this study, a significant decrease in systolic and diastolic blood pressure during pre and post-Ramadan was found (p-value <0.05). According to Azizi F, fasting affects BP and may lead to hypotension [32]. According to Erdem Y et al., intermittent fasting resulted in a significant decrease in office BP values and ABPM (ambulatory BP monitoring) measurements (p-value <0.001) [33]. In some studies, no significant changes in systolic and diastolic BP during this month were reported (p>0.05) [23,31]. Paul AK et al., mentioned that one month fasting lowered diastolic (p-value=0.08) and systolic blood pressure (p-value: 0.17) but the reduction was not significant [28].
Regarding blood glucose parameters, a significant reduction in FBG occurred during Ramadan (p-value <0.001). However, the 2h PPG level did not show any significant difference between the start and the end of Ramadan (p-value >0.05). HbA1c also increased slightly after Ramadan, but was not statistically significant (p-value >0.05).
Kalantary S evaluated the impact of Islamic fasting on blood glucose level in type II diabetic patients in Gilan province in Iran. They demonstrated none of the type II diabetic patients on oral medications or diet developed hypoglycaemic episodes. The mean FBG level before and during Ramadan was 152.35±56.25 mg/dL and 140.18±25.29 mg/dL, which showed a slight decrease, but was not statistically significant (p-value >0.05) [16]. In a study by Sahin SB et al., on blood sugar control among fasting Muslims with type II diabetes mellitus in 122 diabetic patients, there was no significant difference between blood glucose before and after Ramadan [18]. The overall result of Aydin N et al., meta-analysis of 19 clinical trials showed a significant decrease in FBG values during Ramadan (p-value <0.001) [15].
Zainudin SB et al., conducted a study on diabetes training and modifying medication for self-management during Ramadan fasting with 29 participants (75.9% female and 24.1% male). Patients’ HbA1c and weight at the end of the fasting period revealed a significant decrease (p-value <0.01) [34]. In another study by Tibora G, where the metabolic parameters of 80 type 2 diabetic patients were evaluated during Ramadan, changes in fasting blood sugar were not significant (p-value=0.7) [35]. M’guil M et al., focused on the safety of Ramadan fasting and its effect on the clinical and biochemical parameters of type II diabetes patients. The results showed that the blood glucose index did not change significantly at the end of the fasting period (p-value >0.05) [36]. Celik S et al., investigated the effects of Ramadan fasting on daily life and metabolic conditions of type II diabetic patients; 26 patients did not develop any changes in blood glucose index (p-value=0.62) [37].
Evaluating patients’ lipid profiles in the present study before and after fasting showed a significant increase in patients’ triglycerides level. However, cholesterol, HDL, and LDL did not change significantly. The study by Zare A et al., on the effect of fasting during Ramadan on lipid profile showed a significant decline in TG, Cholesterol, LDL level, and elevation of HDL (p-value <0.001) [38]. In Tiboura G et al., study, total cholesterol levels decreased (p-value=0.19), and triglyceride increased slightly (p-value=0.15) but HDL-C decreased significantly (p-value=0.03) [35]. In Khaled BM et al., survey on Ramadan fasting showed modifications in some serum components in 60 obese women with type II diabetes, suggesting that fasting reduced HDL (p-value <0.001) and increased cholesterol (p-value <0.001), triglyceride (p-value <0.003), and LDL (p-value <0.0001) [39]. The elevation in blood TG after fasting during Ramadan may be the result of increased lipolysis of fat tissues [40]. Another possible explanation for increased triglyceride levels in the present study could be decreased physical activity during Ramadan [41]. Also, the time of blood sampling in the evening may affect the triglyceride level due to the nature of diurnal triglyceride changes [42].
Authors did not observe any episode of hypoglycaemia during the study, however in another study it was reported that 10% of 150 diabetic patients experienced hypoglycaemia during the Ramadan [43]. Medical advice before starting of the Ramadan can prevent hypoglycaemic events. Therefore, it was essential to guide the patients about their diet, physical activities, and medication timing before the start of Ramadan fasting [30,43].
Limitation(s)
This study had some limitations, including the unequal proportion of male participants compared with women. More studies with a wider population will be needed to better understand the possible differences between different sexes. Due to the impossibility of intravenous blood sampling two hours after Iftar, 2h PPG was measured with the same glucometer brand in all participants with the devices that were initially provided.
Conclusion(s)
The results of this study indicated that type II diabetic patients who had well-controlled blood sugar before Ramadan and were given consultation by healthcare professionals (for their diet, physical activity, medications, blood glucose monitoring, and symptoms of hypoglycaemia), can have safe fasting during the holy month of Ramadan.
Thyroid stimulation hormone (TSH), Aspartate transaminase (AST), Alanine transaminase (ALT), alkaline phosphatase (ALP), Blood urea nitrogen (Bun), creatinine (Cr) and Acetyl Salicylic Acid (ASA)
p<0.05* statistically significant; p<0.001** statistically highly significant; Paired Samples Test
Comparison of all measurements (pre vs mid/post and mid vs post) were statistically nonsignificant, p>0.5; PPG: Post-prandial glucose
p<0.05* statistically significant
p<0.001** statistically highly significant
Paired Samples Test
p<0.05* statistically significant; p<0.001** statistically highly significant; Paired Samples Test; TG: Triglycerides; HDL-c: High density lipoprotein-cholesterol; LDL-c-: Low density lipoprotein-cholesterol