The Kidney is one of the most highly differentiated organs in the body. Its cellular diversity modulates a variety of complex physiologic processes [1]. The approximate incidence of end-stage renal disease is 150-200 pmp, and the prevalence of chronic kidney disease is 800 per million population (pmp) [2]. The kidneys are affected by various disease processes, some resulting in permanent damage leading to surgical removal of the organ i.e., nephrectomy. Symptomatic chronic infections, obstruction calculous disease or severe traumatic injury may cause end stage renal damage, ultimately requiring nephrectomy. Nephrectomy is also done for treatment of renovascular hypertension, severe parenchymal damage resulting from nephrosclerosis, pylelonephritis, vesicoureteric reflux, congenital dysplasia and benign and malignant tumours [3,4].
Chronic pylelonephritis with hydronephrosis is the most common type of nephrectomy specimen for non-neoplastic conditions due to increase in the incidence of Pelviureteric Junction Obstruction (PUJO) by upper ureteric calculi, whereas in the neoplastic group, Renal Cell Carcinoma (RCC) is the most common, due to increase in the incidence in chronic smokers. Most of the patients with Chronic Pyelonephritis (CPN) lead to permanent and progressive damage to the renal parenchyma ending up with nonfunctioning kidney [3].
Indication for nephrectomy may show geographic variations with different urologic causes in different countries worldwide. In India, non-neoplastic conditions affecting kidney leading to ESRD followed by nephrectomy are more common as compared to other developed countries where malignant tumours are the major cause of nephrectomy. Hence, the objectives of this study were to determine the various kidney lesions requiring nephrectomy in southern Rajasthan and to compare with studies done in different parts of India and worldwide.
Materials and Methods
This cross-sectional study was conducted in the Department of Pathology, Geetanjali Medical College and Hospital (GMCH), Udaipur, Rajasthan. The study was done from January 2015 to March 2020.
Inclusion criteria: All the simple, partial and radical nephrectomy specimens received in Pathology department were included during study period.
Exclusion criteria: Small incisional biopsies were not included.
All histopathological data pertaining to nephrectomy cases, which was being maintained in the histopathology section were retrieved and reviewed. Data was collected based on demographic profile; like age at presentation, gender, symptomatology, laboratory investigations and imaging studies. All the specimens were fixed in 10% buffered formalin, representative bits taken were processed according to standard operating protocol. Sections were cut at 3-4 micron, stained with Haematoxylin and Eosin (H&E) and microscopic details were noted.
Results
The present study included 121 nephrectomy cases received during the period of January 2015 to March 2020. Age of patients ranged from 18 months to 85 years [Table/Fig-1]. Highest incidence was observed in 6th decade, 34 cases (28.09%) followed by 3rd decade, 22 cases (18.18%) and least cases were observed in 9th decade, 1 case (0.82%) with approximately equal preponderance of male (60 cases) and female (61 cases) in the ratio of 0.98:1.
Age wise distribution of nephrectomy lesions.
| Age (Years) | No. of cases | Percentage |
|---|
| 0-10 | 09 | 7.4 |
| 11-20 | 04 | 3.3 |
| 21-30 | 22 | 18.18 |
| 31-40 | 18 | 14.87 |
| 41-50 | 14 | 11.57 |
| 51-60 | 34 | 28.09 |
| 61-70 | 13 | 10.74 |
| 71-80 | 06 | 4.95 |
| 81-90 | 01 | 0.82 |
| Total | 121 | |
Out of 121 nephrectomy cases, 88 (72.7%) of the cases were non-neoplastic lesions and 33 (27.27%) of the cases were neoplastic lesions. Out of these 88 cases, maximum numbers 83 cases (94.31%) were found to have CPN [Table/Fig-2]. Out of these 83 CPN cases, maximum number of cases, 51 cases (61.44 %) were found to be associated with nephrolithiasis (calculi) [Table/Fig-3].
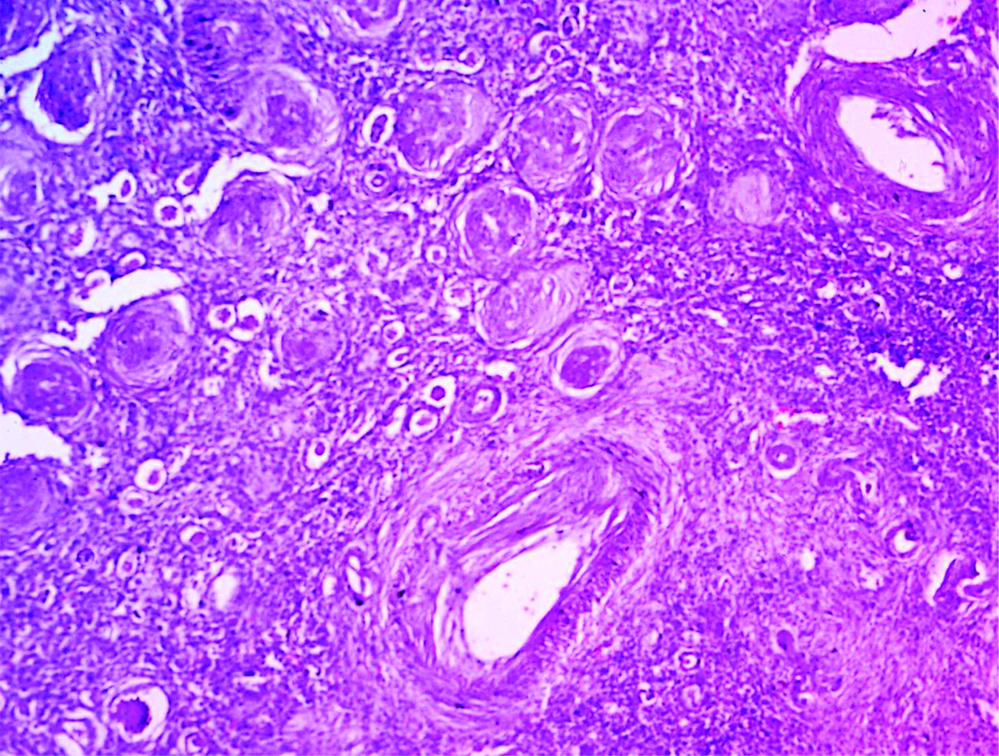
Chronic pyelonephritis showing sclerotic glomeruli, thyrodization of tubules, interstitial chronic inflammatory infilterate and thickened Arteries. (H&E 10X).
Histopathological diagnosis of non-neoplastic lesions.
| S. No. | Lesion | No. of cases | Percentage |
|---|
| 1. | CPN + Nephrolithiasis + Hydronephrosis | 38 | 43.1 |
| 2. | CPN + Nephrolithiasis | 12 | 13.6 |
| 3. | CPN + Hydronephrosis | 18 | 20.4 |
| 4. | CPN | 11 | 12.5 |
| 5. | CPN + Pyonephrosis | 02 | 2.27 |
| 6. | CPN + granulomatous changes | 02 | 2.27 |
| 7. | Hydronephrosis | 01 | 1.13 |
| 8. | Xanthogranulomatous pyelonephritis with Nephrolithiasis | 01 | 1.13 |
| 9. | Cystic lesion | 02 | 2.27 |
| 10. | Traumatic kidney | 01 | 1.13 |
| Total | 88 | |
CPN: Chronic pyelonephritis
In this study, among 88 cases of non-neoplastic aetiology, predominant number of cases were with loss of cortico-medullary junction with dilation of pelvicalyceal system 57 cases (64.77%) and 51 cases (57.9%) cases had calculi on gross. 33 cases (27.27%) with neoplastic aetiology showed tumour growth.
Malignant tumour was the indication for nephrectomy in 33 cases (27.27%). RCC was found in 27 kidney samples (81.8%) [Table/Fig-4,5]. Nephroblastoma was found in two cases (6.06%). The other three malignant tumours consisted of Spindle cell sarcoma, Malignant rhabdoid tumour and Well differentiated liposarcoma pertaining to one case each. Benign tumour oncocytoma accounted for only one case [Table/Fig-6].
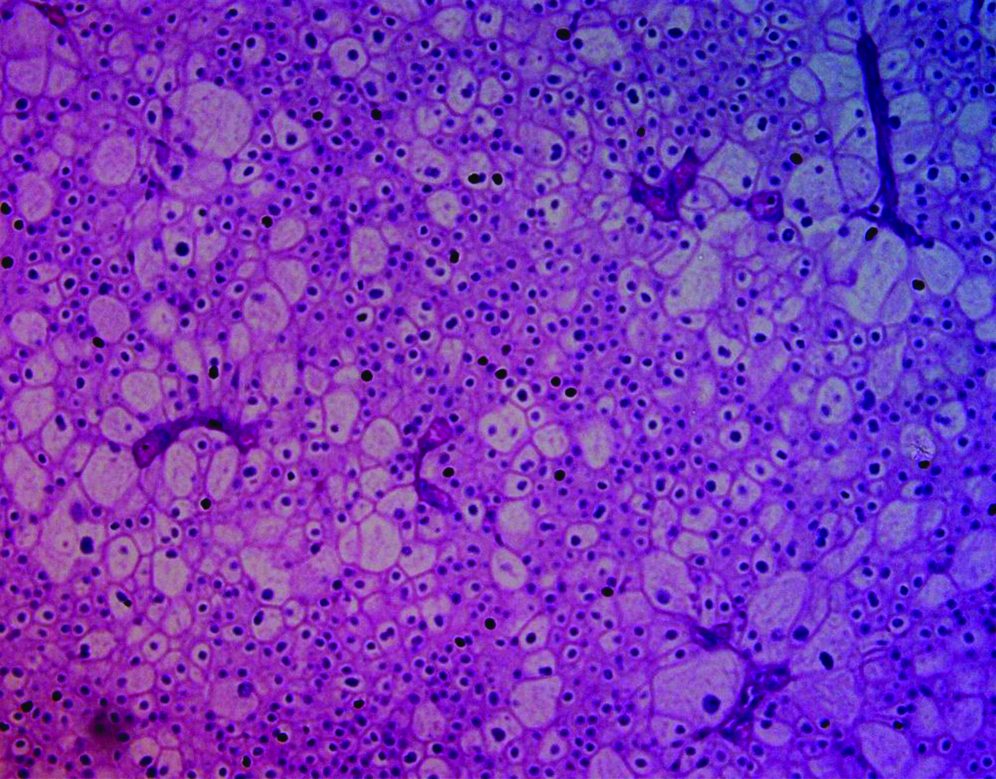
Chromophobe RCC showing tumour cells with cell borders, finely reticular Pale cytoplasm, perinuclear halos and wrinkled raisinoid nuclei. (H&E 20X).
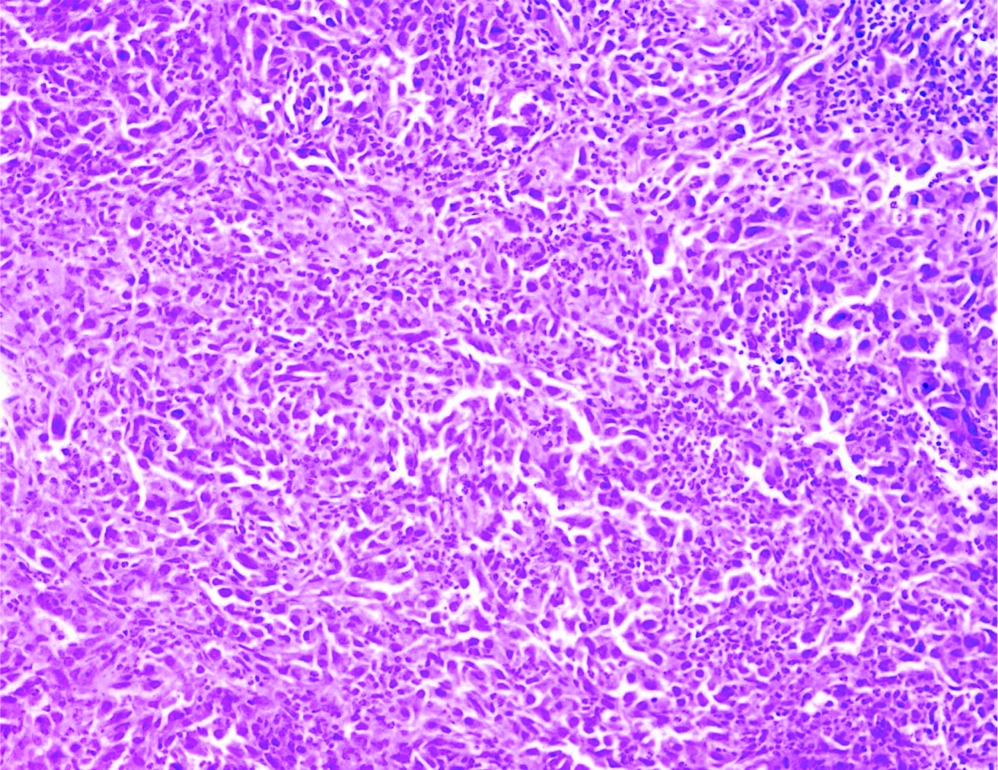
Unclassified RCC showing sarcomatoid component composed Pleomorphic atypical spindle cells. (H&E 20X).
Histopathological diagnosis of neoplastic lesions.
| Tumour | No. of cases | Percentage |
|---|
| Clear cell renal cell carcinoma | 20 | 60.6 |
| Papillary renal cell carcinoma | 04 | 12.1 |
| Chromophobe renal cell carcinoma | 02 | 6.06 |
| Unclassified renal cell carcinoma | 01 | 3.03 |
| Spindle cell sarcoma | 01 | 3.03 |
| Malignant rhabdoid tumour | 01 | 3.03 |
| Well differentiated liposarcoma | 01 | 3.03 |
| Wilm’s tumour (Nephroblastoma) | 02 | 6.06 |
| Oncocytoma | 01 | 3.03 |
| Total | 33 | |
In this study majority, 81 cases (66.94%) presented with flank pain followed by haematuria and fever 73 cases (60.33%), however 11 cases (9.09%) had burning micturition. 25 cases (20.66%) who presented with haematuria had malignant lesions.
In this study, most of the malignant cases, 12 cases (36.36%) were seen in the 6th decade followed by nine cases (27.27%) in 5th decade. Male to female ratio for malignant cases was 1.2:1. It was observed that the right kidney was involved in 23 cases (69.69%) while left was involved in 10 cases (30.30%).
Discussion
A wide array of renal diseases employs nephrectomy as a common procedure for both benign and malignant conditions. Different geographical regions and institutions display distinct causes of nephrectomy. Hence, nephrectomy specimens are analysed histopathologically and only then are treatment guidelines specified particular to the geographic area. In present study, out of 121 nephrectomy cases, 88 (72.7%) were non-neoplastic, and 33 (27.27%) were neoplastic. Similar findings were observed by Aiman A et al., and Shaila S et al., [4,5]. In the present study, majority of nephrectomies were done in the 6th decade (28.09%), followed by the 3rd decade (18.18%). This is in concordance with the study done by Shanmugasamy K and Anandrajvaithy, and Ajmera S and Ajmera R, where most common age group affected was 5th to 6th decade [3,6].
Among the nephrectomy cases, 60 cases (49.58%) were male and 61 cases (50.41%) were female. This finding is variable to study done by Divyashree B et al., and Bashir N et al., [7,8]. In this study, the most common lesion observed was CPN 83 cases (68.59%), followed by RCC 27 cases (22.31%), which is in concordance with the study done by Popat V et al., [9]. In the present study, two cystic lesions and one traumatic kidney were documented, which is similar to the study conducted by Divyashree B et al., [7]. Among 83 cases of CPN gross, majority of cases show dilatation of pelvicalyceal system and loss of corticomedullary junction 57 cases (64.77%) and 51 cases (57.9%) had calculi on gross, which is in concordance with the study conducted by Shanmugasamy K and Anandrajvaithy [3].
Out of 83 cases of CPN, 38 cases were diagnosed with CPN with nephrolithiasis and hydronephrosis, 12 cases of CPN with nephrolithiasis, one case with xanthogranulomatous change and other associated findings include pyonephrosis and cystic lesions, similar to study done by Shanmugasamy K [3] and Chandwale SS et al [10]. Out of 121 cases, neoplastic cases were 33 in number (27.27%). Malignant tumours (32 cases) were more as compared to benign cases (one case). Among the malignant ones, clear cell carcinoma (20 cases i.e., 60.6%) was the most frequent [Table/Fig-7]. This was similar to the study done by Shaila S et al., [5].
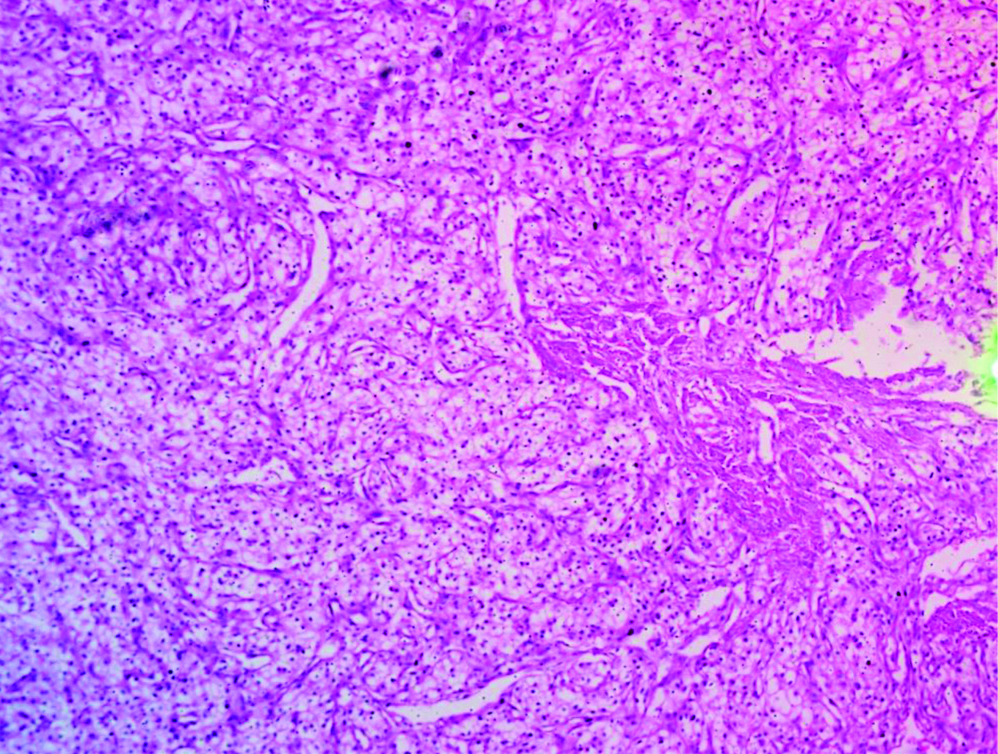
Clear cell RCC showing sheets of tumour cells having clear Cytoplasm and round to oval nuclei. (H&E 10X).
The results of this study enable us to pathologically classify the indications for nephrectomy in Southern Rajasthan and compare the results with those of other workers. Through these findings, the authors have deduced in this article, with sufficient data, that there is a clear variation in patients of nephrectomy housing in different geographic terrain. The main factors largely affecting this are the socioeconomic conditions and health care accessibility. Ghalayini IF, from Sudan reported 423 consecutive nephrectomies performed in general hospital, 70% of which were performed for benign (non-neoplastic) conditions [11]. Malik EF et al., from Saudi Arabia made a report of 77.6% cases of nephrectomies done for benign (non-neoplastic) conditions including 85 cases [12]. Similarly, in a series of 135 nephrectomies reported from Pakistan [13], Rafique M, stated that 76.6% cases were due to benign causes.
Vinay KS and Sujatha S, from Bangalore, India reported a series of 71 nephrectomy cases, out of which 88.73% cases were non-neoplastic and 11.2% cases were neoplastic [14]. Similarly Gupta A and Bhardwaj S, from India made a report of 55 nephrectomies performed in Government Medical College, Jammu, where 80% cases were non-neoplastic, while 20% cases were of neoplastic aetiology [15]. In the present series of 121 nephrectomies performed during the study period of five years, 88 cases (72.7%) were performed for benign conditions, whereas 33 cases (27.27%) were performed for malignant diseases of the kidney. Stone related aetiology was responsible in 51 cases (57.9%), and neglected PUJO was responsible for 18 cases (20.45%).
In most of the reported series from developed countries, malignant diseases of the kidney were the leading causes of nephrectomy. An increased number of nephrectomies were performed for malignant conditions of the kidney which was the result of change in the indication of nephrectomy during the last few decades in Norway, as reported by Beisland C et al., [16]. Badmus TA et al., from Nigeria reported a series of adult nephrectomies, in which 63.3% cases were performed for malignant conditions of the kidney [17]. It was observed in a study from Korea [18], that in earlier times 13.75% cases of nephrectomy were done for renal tumour. In addition to that, 57.12% cases of nephrectomy were done for renal tumours in early 2000. This indicates the decreasing trend of non-neoplastic lesions [Table/Fig-8] [3,11-18].
Comparison between non-neoplastic and neoplastic lesions in the different parts of India and other countries [3,11-18].
| Authors | Part of India | Other countries | Non-neoplastic Lesions (percentage) | Neoplastic Lesions (percentage) |
|---|
| Malik EF et al., [12] | | Saudi Arabia | 77.6 | 22.4 |
| Ghalayini IF [11] | | Sudan | 70.4 | 29.6 |
| Beisland C et al., [16] | | Norway | 32 | 68 |
| Rafique M [13] | | Pakistan | 76.6 | 23.4 |
| Badmus TA et al., [17] | | Nigeria | 36.7 | 63.3 |
| Datta B et al., [18] | North East India | - | 60.2 | 39.8 |
| Shanmugasamy K and Anandrajvaithy [3] | South India | - | 75 | 25 |
| Vinay KS and Sujatha S [14] | South India | - | 88.73 | 11.26 |
| Gupta A and Bhardwaj S [15] | North India | - | 80 | 20 |
| Present study | Southern Rajasthan, India | - | 72.7 | 27.27 |
In contrast, this series mostly consisted of nephrectomies performed for benign diseases of the kidney. Reports from developing countries such as Sudan, Saudi Arabia and Pakistan exhibited benign diseases as the leading cause of nephrectomy, essentially like this series, but this was unlike most study reports which showed malignant conditions as the leading cause of nephrectomy. On critical evaluation, majority of the CPN cases have calculi. It is due to various factors like dietary, genetic and sedentary life style. Commonly, patient develops calcium oxalate stones which occur due to consumption of hard water, super saturation of calcium oxalate and lower urinary citrate concentration [19,20].
Limitation(s)
This study was limited by the possibility of referral bias and population migration, since it was based on ESRD patients evaluated in this particular hospital and with the supposition that all ESRD patients coming in that area were coming to this particular hospital.
Conclusion(s)
Various pathological disease processes lead to permanent damage to kidney, for which nephrectomy is the only mainstay. In this study, most common affected age group was sixth decade of life. Non-neoplastic lesions were the most common cause for nephrectomies, CPN with hydronephrotic changes being the most common cause and clear cell renal carcinoma being common among malignant tumours. Malignant disease nephrectomies are most common in developed countries, but in variation to this, benign conditions of the kidney are the leading cause in the developing world. Our center reported extensive stone disease and neglected PUJO causing diminution followed by complete loss of renal function as the most common cases.
CPN: Chronic pyelonephritis