The coronavirus disease is a highly pathogenic viral infection caused by SARS-CoV-2. The initial cases of novel coronavirus (2019-nCoV)-infected pneumonia (NCIP) occurred in Wuhan, Hubei Province, China, in December 2019 and January 2020 [1]. The WHO announced that the official name of the 2019 novel coronavirus is Coronavirus Disease 2019 (COVID-19) [2]. The ongoing outbreak of COVID-19 infection has posed significant threats to international health and economy. On 30th January 2020, the World Health Organisation (WHO) declared it to be a Public Health Emergency of International Concern [3].
The COVID-19 infection symptoms appear after an incubation period of 5-6 days. The time period depends on the patient’s immune system and age [4]. The major risk factors for severe disease are age more than 60 years (increasing with age), underlying Non-communicable Diseases (NCDs), diabetes, hypertension, cardiac disease, chronic lung disease, cerebrovascular disease, chronic kidney disease, immune-suppression and cancer.
Human-to-human transmission via droplets as well as through contact with fomites seems to be the critical route of the virus spread. Even though the virus is causing mild disease in many, the course of illness may be severe, leading to hospitalisation and even death in elderly or those with co-morbid conditions. Infection can also occur if a person touches an infected surface and then touches his or her eyes, nose, or mouth [5].
The patients with mild symptoms usually recover within a week whereas severe cases have been reported to suffer from progressive respiratory failure due to alveolar damage which can lead to death as well. Time period between onset of COVID-19 symptoms to death ranges between 6-41 days with a 14-day median [6].
In India, the first case was confirmed in Kerala, Thrissur district and in Tamil Nadu, the first case was reported on 7th March 2020 in Kanchipuram district which is adjacent to Chengalpattu district. In Chengalpattu, the first case was reported on 25th March while our institution received its first case on 30th March 2020. Lying south of the state capital, Chengalpattu in Tamil Nadu has emerged on the national map of districts witnessing a surge in coronavirus cases after its proximity to Chennai made it easy for the virus to spread to the peripheral areas.
The objectives are to study the demographic and clinical status of COVID-19 patients at a Tertiary Care Hospital in Chengalpattu District, Tamil Nadu. To assess the co-morbid status and its influence on the outcome among the study population. To find the doubling rate and weekly trend of COVID-19 cases.
Materials and Methods
A cross-sectional study was conducted in Chengalpattu Medical College Hospital, Chengalpattu district among the COVID-19 patients from April 2020 to June 2020. By convenient (non-probability) sampling technique, all the COVID-19 patients (n=3028) admitted in the institution during the study period were included. Those who were not willing to participate in the study were excluded. A semi-structured questionnaire was administered to the patients and care taker of the patients by interview method to collect the data. The questionnaire had three sections A, B and C. Section A deals with sociodemographic details like age, gender, occupation, place and exposure history like living in the same household, living in the neighbourhood, occupational exposure, attending any public gatherings like market or festivities. Section B deals with clinical information like symptom status (fever, cough, breathlessness, sore throat, myalgia, anosmia, headache, diarrhoea), onset of symptoms, duration of hospital stay and co-morbid conditions like diabetes mellitus, systemic hypertension, respiratory illness, cardiovascular diseases, renal disorders, thyroid disorders and morbid obesity. Clinical progression and outcome were also observed. Section C deals with COVID Test results- Real-Time Reverse Transcription-Polymerase Chain Reaction (RT-PCR). Ethical clearance was obtained from the Institutional Ethics Committee (No. IEC-CMC/Approval/5945/2020). A person with laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms [7] was considered as COVID-19 case.
The doubling rate of an infectious disease or epidemic is referred to as the time taken for the total number of cases to double.
Doubling Rate Formula [8]

Statistical Analysis
Data was entered in MS Excel and appropriate descriptive and inferential statistical analysis was done using SPSS Software (version 21.0) and p-value <0.05 is taken as significant.
Results
Total number of positive cases in Chengalpattu district till 30.06.2020 was 5121 (100%) out of which 3028 (59%) were treated in our institution.
As mentioned in [Table/Fig-1] in the study population, the majority of age group affected was 21-40 years, 1489 (49%). The mean age was 38.55±16.21 years. Total 1932 (64%) of the study population were males. Majority of the COVID-19 patients were from urban setting 2574 (85%).
Sociodemographic profile of COVID-19 patients.
| Variables | Frequency | Percentage |
|---|
| Age group | <10 years | 109 | 4% |
| 11-20 years | 203 | 7% |
| 21-30 years | 740 | 24% |
| 31-40 years | 749 | 25% |
| 41-50 years | 523 | 17% |
| 51-60 years | 405 | 13% |
| 61-70 years | 215 | 7% |
| 71-80 years | 65 | 2% |
| >80 years | 19 | 1% |
| Sex | Male | 1932 | 64% |
| Female | 1096 | 36% |
| Place | Urban | 2574 | 85% |
| Rural | 454 | 15% |
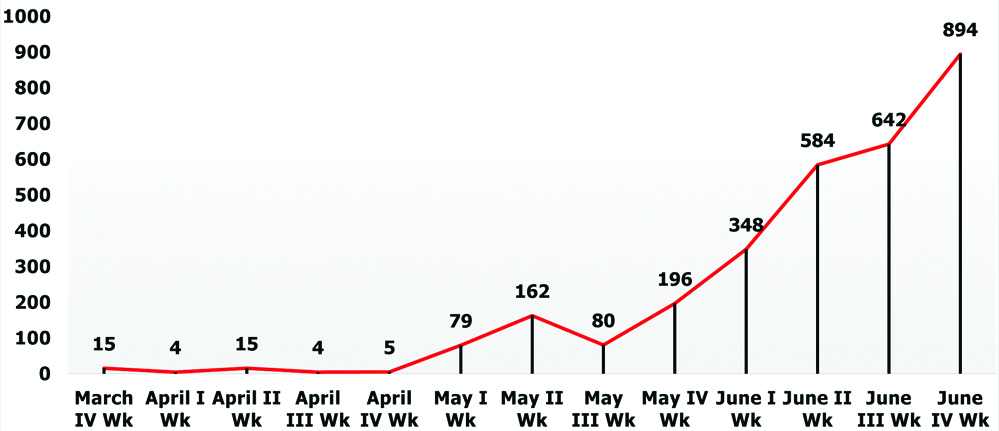
As shown in [Table/Fig-2], the weekly trend of COVID-19 cases shows a steady increase after 3rd week of May and the highest number of cases was recorded (894) in the 4th week of June 2020.
Weekly trend of COVID-19 cases.
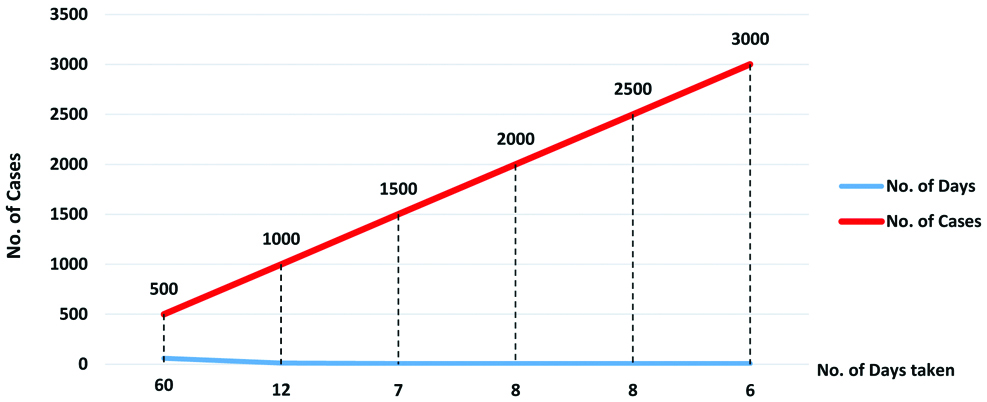
It took 60 days to reach the first 500 cases (index case to 500th case) while the final 500 cases (2500th to 3000th case) reached in six days, which implies the rampant spread of COVID-19 in the district [Table/Fig-3]. As mentioned in [Table/Fig-4] the majority of the study population were asymptomatic 1883 (62%) and 2316 (76%) did not have any co-morbidities.
Time trend of COVID-19 cases.
Clinical status of the COVID-19 patients.
| Variables | Frequency | Percentage |
|---|
| Symptomatic status | Symptomatic | 1145 | 38% |
| Asymptomatic | 1883 | 62% |
| Co-morbidity status | With Co-morbidity | 712 | 24% |
| Without Co-morbidity | 2316 | 76% |
The cumulative cases as of 23rd June 2020 was 2338 and on 30th June 2020 the cases counted upto 3028. Based on this data, using the aforementioned formula, the doubling rate was calculated to be 18.91. Provided the current trend continues, the number of cases is projected to double within a period of 19 days. Hence, the appropriate precautionary measures like strengthening of infrastructure and logistics is advised.
In the present study population, the sources of infections were traced back for 1647 cases out of which the predominant source of infection were living in the same household 891 (54.2%), followed by living in the neighbourhood 372 (22.5%), work environment 144 (8.74%), koyambedu market cluster 129 (7.83), healthcare facility 61 (3.70%) and others 50 (3.03%).
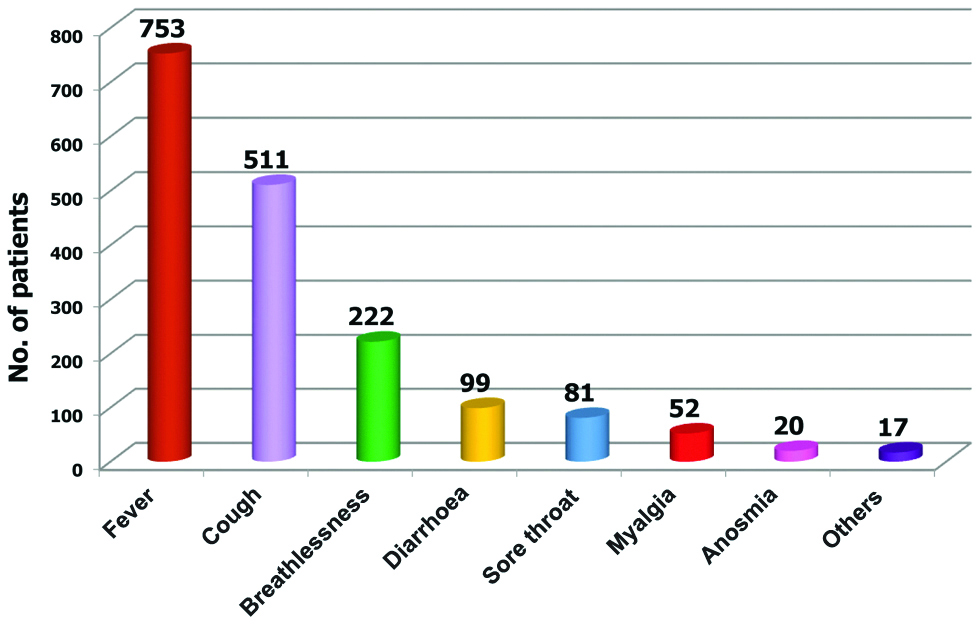
As mentioned in [Table/Fig-5], fever was found to be the predominant symptom followed by cough, breathlessness, diarrhoea, sore throat, myalgia and anosmia in the study population. Among the symptomatic patients, 612 (53.44%) patients were found to have more than one presenting symptom, the most common presentation being fever and cough 289 (25.24%) followed by cough and breathlessness 128 (11.17%), fever and breathlessness 113 (9.86%), fever and diarrhoea 56 (4.89%), fever and sore throat 26 (2.27%).
Symptom status of COVID-19 patients.
In the study population, diabetes mellitus was found to be the most common co-morbid condition followed by hypertension, respiratory illness, cardiac disorders, renal diseases, thyroid disorders, neurological conditions, liver diseases, malignancy and others.
The mean duration of hospital stay of COVID-19 patients was found to be 9.21±3.26 days. The mean duration of hospital stay among COVID-19 death patients was found to be 5.38±4.12 days.
As shown in [Table/Fig-6], the major blood groups were found to be O +ve 663 (38.56%) followed by B +ve 549 (31.93%), which reflects the national pattern of blood group distribution [9].
Blood group-wise distribution of COVID-19 patients (n=1719).
| Blood group | Frequency | Percentage |
|---|
| A+ | 333 | 19.37% |
| A- | 27 | 1.57% |
| B+ | 549 | 31.93% |
| B- | 45 | 2.65% |
| AB+ | 81 | 4.71% |
| AB- | 3 | 0.17% |
| O+ | 663 | 38.56% |
| O- | 18 | 1.04% |
| Total | 1719 | 100% |
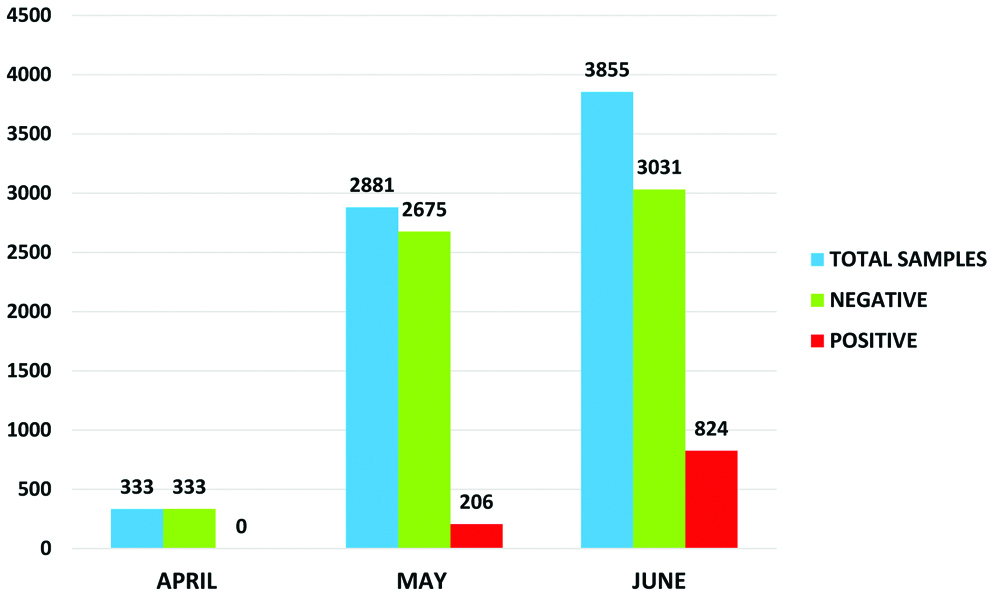
The swab positivity rate was 7% in May 2020 which tripled by June 2020 (21%). The overall swab positivity rate was 14.57% [Table/Fig-7].
Month-wise RT-PCR swab results.
Out of 75 deaths, 13 (17.3%) has been reported in the <50 years age group and 62 (82.7%) in the >50 years age group. There was a statistically significant difference (p-value=0.000) in mortality between these age groups.
The mortality was higher in the group with co-morbidity (9.56%) when compared to the group without co-morbidity (0.30%). There was a statistically significant difference (p-value=0.000) in mortality between these groups [Table/Fig-8].
Gender, age group, co-morbid status Vs outcome of COVID-19 patients.
| Variables | COVID-19 patient outcome | Test, value | p-value |
|---|
| Dead | Recovered |
|---|
| Gender | Male (1932) | 54 (2.80%) | 1878 (97.20%) | Chi-Square Test Value 2.2367df=1 | 0.134 |
| Female (1096) | 21 (1.91%) | 1075 (98.09%) |
| Age group | <50 years (2324) | 13 (0.56%) | 2311 (99.44%) | Chi-Square Test Value 152.15df=1 | <0.001* |
| >50 years (704) | 62 (8.80%) | 642 (91.20%) |
| Co-morbid status | With co-morbidity (712) | 68 (9.56%) | 644 (90.44%) | Chi-Square Test Value 192.83df=1 | <0.001* |
| Without co-morbidity (2316) | 7 (0.30%) | 2309 (99.70%) |
A total of 75 COVID-19 deaths were reported till 30th June 2020, out of which 54 (72%) of the deaths were males and 68 (91%) were associated with co-morbid conditions. There were no COVID-19 deaths in the month of April 2020. In May 2020, there were 12 COVID-19 deaths. The Case Fatality Rate (CFR) was 1.73% and in June 2020, there were 63 deaths (CFR-2.96%). The overall CFR was found to be 2.47%.
Discussion
In the study done in Wuhan by Li Q et al., the doubling time was 7.4 days, while in our study the doubling time was found to be 19 days as on June 2020, which was approximately three times that of the Wuhan study indicating a comparatively lower rate of spread in the population probably due to the strict containment measures by the government [1].
The major age group affected in the study was 20-40 years (49%) which is similar to the study done in Delhi by Gupta N et al., where the major age group affected was 20-40 years [5]. Majority of the economically productive and mobile population belong to this age group (20-40 years) in our population. While in the Wuhan study done by Xu XW et al., the major age group affected was 32-52 years [10] and in study done by Li Q et al., the major age group affected was 45-64 years which are different from the present study [1]. The mean age in the present study was found to be 38.55±16.21 years which is almost similar to the studies done by Gupta N et al., Xu XW et al., Wu J et al., where the mean ages were 40.3 years, 41 years, 46±15 years, respectively [5,10,11].
Males were predominantly affected (64%) in the index study alike the studies Gupta N et al., in which 66.7% of males were affected, Guan W et al., which shows 58%, Chen N et al., which shows 68%, Yang X et al., which shows 67% [5,12-14]. In our study, the most common symptom was fever (38%), alike the studies done in Delhi by Gupta N et al., fever and cough, in Beijing by Jin JM et al., fever and cough, in Wuhan by Zhang F et al., fever and cough [5,15,16]. In our study, family exposure was the most common source of infection, which is very similar to the study in Delhi by Gupta N et al., [5] implying overcrowding, potential risk of exposure due to the prolonged contact time. Duration of hospital stay in our study was 9±3.26 days which is approximate to the study done in Delhi by Gupta N et al., was 11.54 days [5]. In a study conducted by Richardson S et al., in New York, the mean duration of hospital stay was found to be 4.1 days. All these differences in mean duration of stay in hospital is due to the discharge policy of the respective Governments [17].
In our study, 24% of patients had co-morbidities, the most common conditions being Diabetes Mellitus (DM) and Hypertension (HT), which is similar to the study by Gupta N et al., Delhi in which 28% had co-morbidities, the most common being DM and HT, Jin JM et al., Wuhan- (HT and DM), Zhou F et al., Wuhan in which 48% had co-morbidities, the most common being DM and HT, which reflects the overall trend of non-communicable diseases in a global scenario [5,15,18].
In the Wuhan study, by Zhou F et al., 67% of COVID-19 deaths had co-morbidities which differ from our study, in which 91% of COVID-19 deaths had co-morbidities implying, those with underlying co-morbid conditions has an increasingly rapid and severe progression, often leading to death [18].
In the study by Zhang F et al., in China CFR was 8.9%, in contrast our CFR was 2.47% because of intensified contact tracing, tracking and treating by the Government [16]. Out of 75 deaths in our study, 9.3% was contributed by <40 years of age group, which is almost closer to Mexico, where 7.3% of deaths was contributed by <40 years age group according to the study done by Ioannidis JPA et al., [19]. In our study, majority of the deaths belonged to the 61-80 age group (34.37%). Similarly, majority of deaths belonged to the 61-80 age group (46.9%) in the study done by Richardson S et al., in New York, USA. Elderly people are at high risk of COVID-19 complications due to decreased immunity and body reserves as well as multiple associated co-morbidities. In our study, 72% of deaths were reported in males which is very similar to study done by Richardson S et al., in New York, USA which highlights the importance of Gender analysis and Gender- responsive Public health policies and measures to curb the pandemic [17].
Limitation(s)
This study was conducted in a single tertiary care centre in Tamil Nadu, whereas a multicentric study involving different states of India will give a better insight into the demographic and clinical status of COVID-19.
We were not able to analyse the laboratory investigations like D-dimer, IL6, serum ferritin due to financial constraints.
Keeping in mind the aforementioned limitations a sufficiently funded, multicentric, case-control study (mild and severe COVID-19 cases) is recommended for future research.
Special focus to be given to the people aged >50 years and with co-morbid conditions.
Always comply with the preventive measures like social distancing, wearing mask, cough etiquette, hand hygiene and surface hygiene.
People should be cautious about the COVID-19 symptoms and report to the nearest healthcare facility at the earliest.
Behavioural Change Communication (BCC) should be intensified among the public regarding preventive and promotive aspects of COVID-19.
Sensitise the communities against stigmas related to COVID-19 and counsel them to deal with it.
Conclusion(s)
This study clearly revealed that those with age >50 years and patients with co-morbid conditions are at more risk of developing complications and mortality from the COVID-19 than others. So, special focus to be given for the vulnerable groups mentioned above. In our study, the doubling rate was found to be 19 days. Hence, strict containment measures are recommended to lengthen the doubling rate.