Collaboration between Paediatrician and Orthopaedician in Management of Congenitial Talipes Equino Varus by Ponseti Method
JB Santhosha1, SP Akshatha2
1 Assistant Professor, Department of Orthopaedics, ADI Chunchanagiri Institute of Medical Sciences (AIMS), Mandya, Karnataka, India.
2 Assistant Professor, Department of Paediatrics, ADI Chunchanagiri Institute of Medical Sciences (AIMS), Mandya, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: SP Akshatha, Assistant Professor, ADI Chunchanagiri Institute of Medical Sciences (AIMS), BG Nagar, Nagamangala (Taluk), Mandya, Karnataka, India.
E-mail: foryourhelp55@gmail.com
Introduction
Congenital Talipes Equino Varus (CTEV) or Clubfoot is one of the commonest orthopaedic problems observed in infants. Deformity involving in utero malalignment of calcaneo-talar-navicular complex of the foot is known as CTEV. Due to lack of treatment capacity and less knowledge about “Appearance, Pulse, Grimace, Activity, and Respiration.” (APGAR) Score in low income countries, CTEV end up with neglected clubfoot deformity (untreated children >2 years). About 1-2/1000 live births is the estimated incidence of idiopathic clubfoot.
Aim
To assess the clinical profile and efficacy of Ponseti technique in the management and treatment of CTEV by Paediatrician and Orthopaedician collaboration.
Materials and Methods
The observational study was conducted at AdiChunchanagiri Institute of Medical Sciences (AIMS). The data was recorded in a standard predesigned proforma which contained all details of patients like name, age, sex, parent details, address, family history, pregnancy and delivery details of mother, any prior treatment taken for clubfoot and examination details of spine, hips, upper and lower limbs with both feet and also other systems for associated clinical problems. The parents of the patients visiting Paediatric Out Patient’s Department (OPD) with CTEV were informed regarding the deformity and were sent to Orthopaedic Department. In Orthopaedic Department, after counselling of the parents regarding the ponseti method, all patients were treated and managed. All patients were followed over a two year period and assessed for any deformities which were subsequently managed surgically. All the data was documented, statistically analysed using suitable statistical methods.
Results
Total 53 patients had 81 idiopathic CTEV or Clubfoot between the period of three years from 2015 to 2018. The age of patients varied upto one year after birth. Among 53 patients, 38 (72%) were males and 15 (28%) were females. Out of 53 infants, 35 had one clubfoot and 23 had bilateral clubfoot (total 81 clubfoot in 53 infants). The mean age of initial presentation to treatment was 3.5 weeks, 11 out of 53 infants came in 1st week of life. Out of 53 infants, 21,14,6,5,4,2 were followed-up for 7-12 months, 13-18 months, 0-6 months, 25-30 months, 19-24 months and 31-36 months, respectively. Out of 81 clubfoot; 76 (93.83%) had achieved near normal correction, five clubfoot (6.17%) required posteromedial soft tissue release, 67 foot (82.71%) had undergone percuteneoustenotomy and nine foot (11.11%) got corrected without tenotomy.
Conclusion
CTEV or clubfoot is treated very safely and effectively by using ponseti method. It is rapidly decreasing the necessity of extensive surgery. This method should be encouraged to be set as the gold standard treatment of congenital clubfoot or CTEV by national efforts.
Clubfoot, Congenital, Surgery
Introduction
The CTEV or Clubfoot is one of the commonest orthopaedic problems observed in infants. Deformity involving in utero malalignment of calcaneo-talar-navicular complex of the foot is known as CTEV [1]. Due to lack of treatment capacity and less knowledge about APGAR Score in low income countries CTEV end up with neglected clubfoot deformity (untreated children >2 years). About 1-2/1000 live births is the estimated incidence of idiopathic clubfoot [2]. CTEV has male predominance of 2:1 and an incidence of bilateralness estimated to be about 50% [3]. About 30000 per year children born in India with clubfoot or CTEV according to the Global Clubfoot Initiative report [4]. With least interruption of socioeconomic of the parent and child CTEV or clubfoot treated to correct all the components within the minimum time duration to obtain plantigrade, painless, pliable, cosmetically and functionally acceptable foot [5,6]. Worldwide, Low and Middle Income Countries (LMICs) have 80% of children born with clubfoot [7]. Maximum cases of clubfoot remains untreated or poorly treated, leaving them to face a life of disability. This may lead to causes crushing physical, social, psychological and financial burdens on the patients, their families and society [8]. The aetiology of clubfoot is classified into two categories: idiopathic clubfoot, where there is only foot deformity and the rest of the musculoskeletal system is normal and non-idiopathic clubfoot where the foot deformity is a local manifestation of associated systemic skeletal deformities [9]. Small heel drawn up with foot points plantar. midfootcavus, hind footvarus, ankle equinus and forefoot adductus are four components of deformity [5]. On the concave medial and plantar aspect skin creases deeply, skin creases on lateral dorsum of the foot is thinned, stretched and creases disappear. Patients exhibit calf atrophy and the degree of flexibility varies. In untreated cases subsequently it lead to gait abnormality after the deformity progressively increases, ambulation being difficult and resulting in limb length discrepancy [1,10]. After the disturbing failure and complications patients must undergo extensive corrective surgery. Revision of extensive corrective surgery are more common. After surgery the foot looks better but stiff, weak and often painful too. The crippling becomes often and pain increases after adolescence [11]. Regardless of the severity of the deformity, the clubfoot should be initially treated by non-operative methods.
A method of clubfoot correction was developed by the late Dr. Ignacio Ponseti which realigns the clubfoot in infants without extensive and major surgery. It is done by manipulation and casting on the basis of the fundamentals of kinematics and pathoanatomy of the deformity [12]. Ponseti method is a non-surgical technique which was used to treat clubfoot successfully in 90% to 98% of cases [13,14]. This method of treatment is taken as gold standard for clubfoot deformity [15]. This method was first described by Dr. Ponseti in 1950s and hundreds of children were successfully treated. To achieve mobile foot with normal function, the treatment of clubfoot should be started immediately after birth of the child. Basically there are two methods of management: conservative management and surgical correction [1,10]. Conservative management of treatment should be used in the first visit of the neglected child. Tapping, strapping, manipulation and serial casting are included in the techniques [6,16-18]. The exact following of the individual treatment steps performed by a qualified orthopaedist and also the early beginning of treatment defines the success of this method. The treatment should be started within two weeks after baby’s birth and the feet device must be adequately used for more than two years. In this process of treatment, the paediatrician plays the key role by determining the eqinovarus foot, monitoring the child actively and looking for the correct administration of the device treatment. The aim of this study is to assess the clinical profile and efficacy of Ponseti technique in the management and treatment of CTEV by paediatrician and orthopaedician collaboration.
Materials and Methods
This observational study was conducted at AIMS in which total 53 patients had 81 idiopathic CTEV or Clubfoot between the period of three years from 2015 to 2018. The newborns and infants with CTEV, visiting paediatric OPD were included in the study, while patients suffering from other congenital malformation were excluded. The age of patients varied up to first year after birth. The Institutional Ethical Committee (ethical clearance no-ACIMS/ER/OD/2341) approval was taken and the patient informed written consent was also taken from the patient’s parents. The data was recorded in a standard predesigned proforma which contained all details of patients like name, age, sex, parent details, address, family history, pregnancy and delivery details of mother, any prior treatment taken for clubfoot and examination details of spine, hips, upper and lower limbs with both feet and also other systems for associated clinical problems. The parents of the patients visiting paediatric OPD with CTEV were informed regarding the deformity and were sent to orthopaedic department. In orthopaedic department, after counselling of the parents regarding the ponseti method, all patients were treated and further managed. Pirani score of pre and post casting for all patients with clubfoot was calculated. Pirani score is a 0-6 point scale; the higher score defines the more severe deformity. All patients were followed over a two year period and assessed for any deformities which were subsequently managed surgically.
Statistical Analysis
All the data was documented, statistically analysed using Statistical Package for Social Sciences (SPSS) version 20. Pearson’s Chi-square test of significance was used and p-value <0.05 was considered significant.
The steps of Ponseti method of management are presented in [Table/Fig-1]:
A specific method of manipulation
A specific method of castings
Percutaneous method of tenotomy
A specific method of bracing with Denis Brown splint for two to three year period
Follow-up for recurrence
A specific method of treating recurrence
Showing the steps involved in Ponseti method of manipulative correction of CTEV or Clubfoot.
| Clinical feature | Pathology | Corrective manipulation | Cast number |
|---|
| Cavus | Plantar flexed 1st metatarsal | Dorsi flex 1st metatarsal | 1 |
| Adductus | Medial subluxation of talo-navicular joint | Abduct foot | 2, 3, 4 |
| Varus | Calcaneal inversion | Adduct calcaneus | 2, 3, 4 |
| Equinus | Calcaneal flexion | Abduct calcaneus | 2, 3, 4 |
| Tibio-talar flexion | Percutaneous tenotomy and cast in maximal abduction and 10-20 degree extension | 5 |
Results
Between the three years period from 2015 to 2018, a total of 53 patients had idiopathic CTEVs or clubfoot. Patients ranged in age from up to first year after birth. Total 38 (72%) of the 53 patients were men and 15 (28%) were women.
Out of 53 infants, 35 had one clubfoot and 23 had bilateral clubfoot (total 81 clubfoot in 53 infants). The mean age of initial presentation to treatment was 3.5 weeks, 11 out of 53 infants came on first week of life. Depending upon the response to Ponseti method of management, the number of castings required prior to tenotomy varied with each patient.
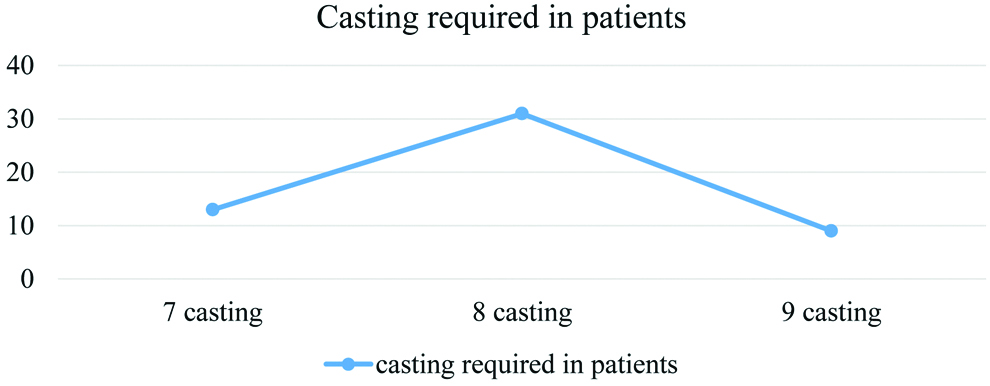
Out of 53 infants, seven castings were required in 13 infants, eight castings in 31 infants and up to nine castings in nine infants [Table/Fig-2].
Figure shows casting required in patients.
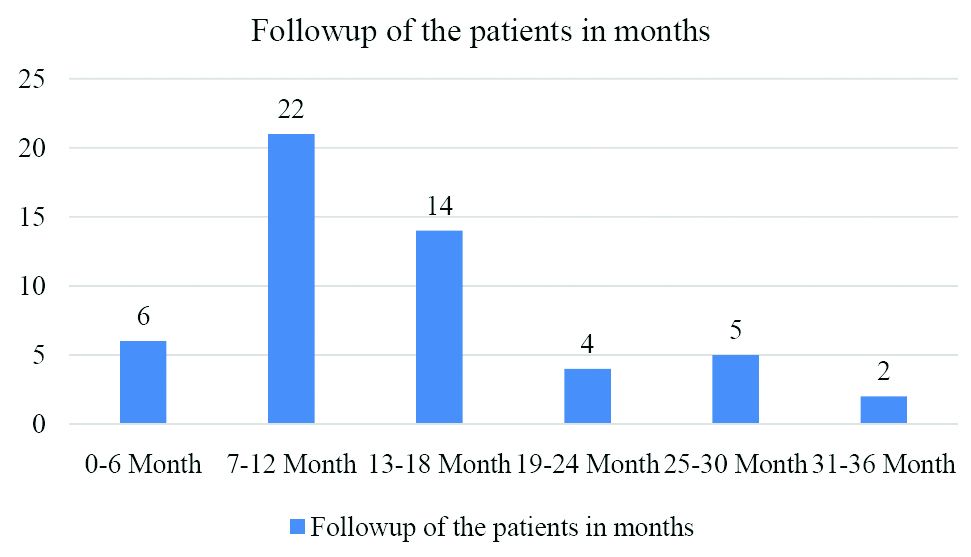
Maximum patients were followed-up for 7-12 months followed by 13-18 months and only two patients were followed-up 31-36 months [Table/Fig-3].
Figure shows duration of follow-up in months of the clubfoot patients.
Out of 81 CTEV or clubfoot; 76 (93.83%) had achieved near normal correction, Achilles tenotomy was needed in 59 (72.83%) feet [Table/Fig-4], five clubfoot (6.17%) required posteromedial soft tissue release, 67 foot (82.71%) had undergone percuteneous tenotomy and 9 foot (11.11%) got corrected without tenotomy.
Showing results of other variables and outcome as determined by Pirani score.
| Variables | n | Percentage |
|---|
| Percutaneous tenotomy of Achille’s tendon | 59 | 72.83% |
| Patients with calf abnormality (thin) n=81 | 43 | 53.08% |
| Patients with positive family history | 04 | 7.54% |
| Pirani score before treatment | Range | Mean |
| 3-6 | 5.03±0.48 |
|---|
| Pirani score after treatment i.e., <0.5 | Frequency | Percentage |
| 76 | 93.83% |
All the foot were applied with Denis Brown splint for two years and followed-up for two year period for any relapses. Out of 81 clubfoot, 17 (20.98%) had relapses; 11 (13.58%) relapses of equinus and five (6.17%) relapses of equino-cavo-varus were observed and were corrected with repeat tenotomy and serial POP castings.
Discussion
Early stage treatment of idiopathic clubfoot by ponseti method was the most successful method which had minimum need for further extensive corrective surgery. Many similar studies using ponseti method are comparable with present study shown in [Table/Fig-5] [6,19-24].
Comparison of present study from other study [6,19-24].
| S. No. | Name of the author | Year of study | Success rate (%) |
|---|
| 1 | Bor N et al., [19] | 2009 | 89 |
| 2 | Jowett CR et al., [20] | 2011 | 90 |
| 3 | Eberhardt O et al., [21] | 2013 | 89 |
| 4 | Colburn M and Williams M, [6] | 2003 | 95 |
| 5 | Morcunde JA et al., [22] | 2004 | 98 |
| 6 | Seger E et al., [23] | 2005 | 94 |
| 7 | Lasebikan OA et al., [24] | 2019 | 96.6 |
Similar above studies had less success rate than this study comparatively, the reason was that we started treating early after birth but studies conducted by Dobbs MB et al., and Lehman WB et al., had >95% success which was better success rate comparatively to this study because of non-compliance with the abduction brace by the care takers at home which was not done in this study, it was done in hospital in case of this study [25,26]. The clubfoot almost looked usual for the parents of 32 patients (65.30%) and it was nearly normal for the parents of 12 patients (24.49%) according to the similar study done by Porecha MM et al., [27]. Among 49 patients who responded to initial Ponseti casting, 14 patients 28.57% (19 clubfeet 28.35%) had relapse at different age; where nine patients 64.29% (10 clubfeet 52.63%) were resistant to the Ponseti casting procedure, while five patients 35.71% (9 clubfeet 47.37%) were resistant to Ponseti method.
The CTEV treatment by ponseti method gives good results, therefore it has been gaining popularity day by day [26,28]. This method of treatment is taken as gold standard for clubfoot deformity as it is easy, effective, in expensive and it does not include surgery as well as it has success rate of 90-98% [29]. The rate of complications and chances of recurrence is low in ponseti method. Adequate correction was achieved In Malawi in 98 of 100 feet in 75 children. An 11.5 weeks was the mean age reported by Tindall AJ et al., [18].
The poor socioeconomic status, rural background of the parents and lack of knowledge could be the reason of the relapses in this study. Out of 81 clubfoot, 17 (20.98%) had relapses; 11 (13.58%) relapses of equinus and 5 (6.17%) relapses of equinocavovarus were observed and were corrected with repeat tenotomy and serial POP castings, which is similar to the study done by Morcuende JA et al., they reported 11% relapse rate, another similar conducted by Porecha MM et al., reported 28.35 relapse rate in different ages [22,27].
Difficulties like social and style of life pattern and others could not be solved by paediatrician alone as these are because of lack of knowledge of the parents. But the paediatrician guidance to the parents regarding the necessary treatment and timely visit of the patients to the orthopaedist would be very useful for fast and better recovery. Both the orthopaedist and paediatrician should have the knowledge about the diseases and its stages for the proper treatment.
Limitation(s)
The study had some limitations: The sample size was small. Longer follow-up would have been necessary, ideal but taking into account the difficulties of acquiring follow-up in developing and poor country with high transportation cost it was not possible.
Conclusion(s)
The CTEV or clubfoot is treated very safely and effectively by using ponseti method. It is rapidly decreasing the necessity of extensive surgery, this method should be encouraged to be set as the gold standard treatment of congenital clubfoot or CTEV by national efforts. The orthopaedist is obliged to this treatment however the collaboration with a paediatrician will increase the success rate of the treatment. Ponseti method does not include surgery, it is minimum invasive, simple, affordable and effective. It does not require general anaesthesia and can ideally be performed at OPD even in neonatal period.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 22, 2020
Manual Googling: Oct 09, 2020
iThenticate Software: Nov 25, 2020 (12%)
[1]. Nelson text book of pediatrics, 18th edition, chapter 673.3; 2007, vol 2, Pp. 2777-78 [Google Scholar]
[2]. Arif M, Inam M, Sattar A, Shabir M, Usefulness of Ponseti technique in management of congenital telipes equino-varusJ Pak Orthop Assoc 2011 23:62-64. [Google Scholar]
[3]. Staheli L, Clubfoot: Ponseti Management 2003 Seattle, WA, USAGlobal HELP Publications:4-5. [Google Scholar]
[4]. Globalclubfoot. India | Global Clubfoot Initiative. 2018. Available online: http://globalclubfoot.com/countries/india/ (accessed on 31 March 2018) [Google Scholar]
[5]. Ponseti IV, Clubfoot managementJ Pediatr Orthop 2000 20:699-700.10.1097/01241398-200011000-0000111097239 [Google Scholar] [CrossRef] [PubMed]
[6]. Colburn M, Williams M, Evaluation of the treatment of idiopathic clubfoot by using the Ponseti methodJ Foot Ankle Surg 2003 42:259-67.10.1016/S1067-2516(03)00312-0 [Google Scholar] [CrossRef]
[7]. Africa Clubfoot Training Project. Chapter 2 Africa Clubfoot Training Basic and Advanced Clubfoot Treatment Provider Courses-Participant Manual; Africa Clubfoot Training Project. Oxford, UK: University of Oxford:2017 [Google Scholar]
[8]. Kelly DM, Congenital anomalies of the lower extremityIn Campbell’s Operative Orthopaedics, 12th ed.; Canale, S., Beaty, J., Eds. 2013 Philadelphia, PA, USAMosby Elsevier:994-1012. [Google Scholar]
[9]. Wainwright AM, Auld T, Benson MK, Theologis TN, The classification of congenital talipes equinovarusJ Bone Joint Surg Br 2002 84(7):1020-24.10.1302/0301-620X.84B7.084102012358365 [Google Scholar] [CrossRef] [PubMed]
[10]. Campbell: Operative orthopedics, 12th edition, 2012; vol 2; 994-1012 [Google Scholar]
[11]. Morcuende J, Dolan L, Dietz F, Ponseti I, Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti methodPediatrics 2004 113:37610.1542/peds.113.2.37614754952 [Google Scholar] [CrossRef] [PubMed]
[12]. Ponseti IV, Smoley EN, Congenital clubfoot: The results of treatmentJ. Bone Joint Surg 1963 45:261-344.10.2106/00004623-196345020-00004 [Google Scholar] [CrossRef]
[13]. Cooper DM, Dietz FR, Treatment of idiopathic clubfoot. A thirty-year follow-up noteJ Bone Joint Surg Am 1995 77:1477-89.10.2106/00004623-199510000-000027593056 [Google Scholar] [CrossRef] [PubMed]
[14]. Maripuri SN, Gallacher PD, Bridgens J, Kuiper JH, Kiely NT, Ponseti casting for club foot- above- or below-knee? A prospective randomised clinical trialBone Joint J 2013 95B:1570-74.10.1302/0301-620X.95B11.3189924151281 [Google Scholar] [CrossRef] [PubMed]
[15]. Mahan ST, Spencer SA, May CJ, Prete VI, Kasser JR, Club foot relapse: Does presentation differ based on age at initial relapse?J Child Orthop 2017 11:367-72.10.1302/1863-2548.11.1700162908185 [Google Scholar] [CrossRef] [PubMed]
[16]. Dobbs MB, Mocuende JA, Gurnett CA, Ponseti IV, Treatment of idiopathic clubfoot; a historical reviewIOWA Orthopedic J 2000 20:59-64. [Google Scholar]
[17]. Dobbs MB, Rudzki JR, Purcell DB, Walton T, Porter KR, Gurnett CA, Factors predictive of outcome after the use of Ponseti method for the treatment of idiopathic clubfootJ Bone Joint surg Am 2004 86(1):22-27.10.2106/00004623-200401000-0000514711941 [Google Scholar] [CrossRef] [PubMed]
[18]. Tindall AJ, Steinlechner CWB, Lavy CBD, Mannion S, Mkandawire N, Results of manipulation of idiopathic clubfoot deformity in malawi by orthopedic clinical officers using ponseti method; a realistic alternative for developing world?J Pediatric Orthop 2005 25:627-29.10.1097/01.bpo.0000164876.97949.6b16199944 [Google Scholar] [CrossRef] [PubMed]
[19]. Bor N, Coplan JA, Herzenberg JE, Ponseti method for idiopathic clubfoot; min 5 year follow upClin orthop Relat Res 2009 467(5):1263-70.10.1007/s11999-008-0683-819130158 [Google Scholar] [CrossRef] [PubMed]
[20]. Jowett CR, Morcuende JA, Ramachandran M, Management of CTEV using Ponseti method; A systematic reviewJ Bone & Joint Surg Br 2011 93(9):1160-64.10.1302/0301-620X.93B9.2694721911524 [Google Scholar] [CrossRef] [PubMed]
[21]. Eberherdt O, Peterlein CD, Fernandaz FF, Wirth T, Midterm results of idiopathic clubfoot treated by Ponseti methodJ Orthop Unfall 2012 150(2):190-97.10.1055/s-0031-129827122354441 [Google Scholar] [CrossRef] [PubMed]
[22]. Morcuende JA, Dolon LA, Dietz FR, Ponseti methodPediatrics 2004 113:376-800.10.1542/peds.113.2.37614754952 [Google Scholar] [CrossRef] [PubMed]
[23]. Segar E, Keret D, Lokiec F, Yavor A, Wientroub S, Ezra E, Early experience with Ponseti method for the treatment of congenital idiopathic clubfootIsr Med Assoc J 2005 7(5):307-10. [Google Scholar]
[24]. Lasebikan OA, Anikwe IA, Onyemaechi NO, Chukwujindu ED, Nwadinigwe CU, Omoke NI, Ponseti clubfoot management method: Initial experience with 273 clubfeet treated in a clubfoot clinic of a Nigerian regional orthopedic hospitalNiger J Clin Pract 2019 22:1266-70.10.4103/njcp.njcp_401_1831489864 [Google Scholar] [CrossRef] [PubMed]
[25]. Dobbs MB, Gordon JE, Walton T, Schoenecker P, Bleeding complication following percutaneous tendoachilles tenotomy in the treatment of clubfoot deformityJ Pediatr Orthop 2004 24:353-57.10.1097/01241398-200407000-0000215205614 [Google Scholar] [CrossRef] [PubMed]
[26]. Lehman WB, Mohaideen A, Madan S, Scher DM, Van Bosse HJP, Iannacone M, A method for the early evaluation of the Ponseti (Iowa) technique for the treatment of idiopathic clubfootJ Pediatr Orthop B 2003 12:133-40.10.1097/01202412-200303000-00011 [Google Scholar] [CrossRef]
[27]. Porecha MM, Parmar DS, Chavda HR, Mid-term results of Ponseti method for the treatment of congenital idiopathic clubfoot- (a study of 67 clubfeet with mean five year follow-up)J Orthop Surg Res 2011 6:310.1186/1749-799X-6-321226940 [Google Scholar] [CrossRef] [PubMed]
[28]. Miedzybrodzka Z, Congetial Talips equino-varus (club foot) a disorder of the foot but not the handJ Anat 2003 202:37-42.10.1046/j.1469-7580.2003.00147.x12587918 [Google Scholar] [CrossRef] [PubMed]
[29]. Halanski MA, Davison JE, Huang Ponseti method compared with surgical treatment of clubfoot; A prospective comparisionJ Bone Joint Surg Am 2010 92:270-78.10.2106/JBJS.H.0156020124052 [Google Scholar] [CrossRef] [PubMed]