Primary Thyroid Lymphoma in an Adult Male: A Rare Presentation
Poonam Dambhare-Wasnik1, Ashish Kumar Gupta2
1 Senior Resident, Department of Pathology and Lab Medicine, AIIMS Raipur, Raipur, Chhattisgarh, India.
2 Assistant Professor, Department of Pathology and Lab Medicine, AIIMS Raipur, Raipur, Chhattisgarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Poonam Dambhare-Wasnik, Flat 702, Type 5A Building, AIIMS Residential Complex, Kabir Nagar, Raipur, Chhattisgarh, India.
E-mail: poonampwasnik@gmail.com
Primary Thyroid Lymphoma (PTL) is a rare entity prevalent in middle to old aged females. They are predominantly B-cell Non-Hodgkin’s Lymphoma (NHL), among which Diffuse Large B-Cell Lymphoma (DLBCL) is the most common subtype. Here, the authors have described a case of PTL in a male patient which is extremely rare. The patient presented with a swelling over anterior aspect of neck and dysphagia since two months. Fine Needle Aspiration Cytology (FNAC) of thyroid swelling and following immunocytochemistry showed B-cell NHL. Histopathological and Immunohistochemical (IHC) examination was also done thereafter on right hemithyroidectomy specimen, which revealed a non-germinal centre type of DLBCL. Histopathological examination revealed an antecedent chronic lymphocytic thyroiditis in this patient. With this case, it was evident that early diagnosis of thyroid lymphoma can be possible with FNAC. However, false negative diagnosis can occur on non-representative aspiration sample. Besides this, it is challenging for a pathologist to subtype the lymphoma on cytology smear. Hence, histopathological examination along with Immunohistochemistry (IHC) is imperative for accurate diagnosis of PTL. The patient had received three cycles of chemotherapy and follow-up of 11 months was uneventful.
Biopsy, Diffuse large B-cell lymphoma, Fine needle aspiration cytology
Case Report
A 52-year-old male presented in OPD with progressive swelling over anterior aspect of neck since two months. Patient had dysphagia for both solid and liquid food since six days. On examination, a diffuse non-tender thyroid swelling was noted, measuring 4×3 cm over left lobe and 3×3 cm over right lobe of thyroid, which was moving with deglutition [Table/Fig-1]. Local ultrasound of neck showed enlarged bilateral lobes of thyroid, right greater than left, with large lobulated hypoechoic lesion suggestive of neoplastic mass.
Clinical image of patient showed diffuse swelling over anterior aspect of neck.

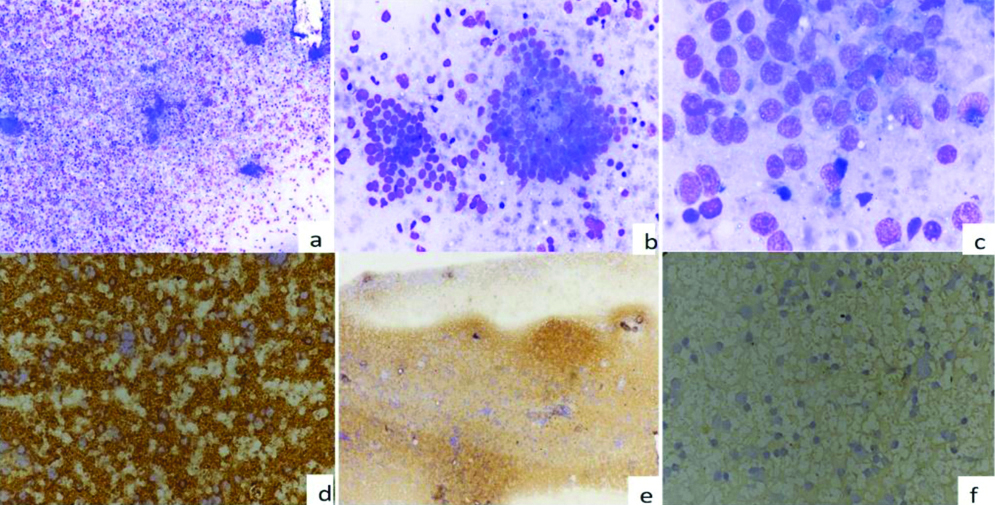
The FNAC of the thyroid swelling was done. FNA smears were cellular [Table/Fig-2a]. Smears showed monomorphic population of medium to large sized lymphoid cells which were discretely arranged [Table/Fig-2b]. The cells showed high nucleus-cytoplasm (N:C) ratio, fine chromatin with prominent single to multiple nucleoli. Mature lymphocytes, plasma cells and lymphoglandular bodies were noted in the background [Table/Fig-2c]. Occasional aggregates of benign thyroid follicular cells were noted. Immunocytochemistry revealed CD45 positivity [Table/Fig-2d] and CD20 positivity [Table/Fig-2e] with absent immunoreactivity for TTF-1 [Table/Fig-2f] and PAX8. Diagnosis of Non-hodgkin’s Lymphoma (NHL) B-cell type (Bethesda category VI) was suggested.
FNAC microphotograph showing: a) cellular smears (x100, Giemsa); b) monomorphic population of medium to large sized lymphoid cells which were discretely arranged (x400, Giemsa); c) cells have high nucleus-cytoplasm (N:C) ratio, fine chromatin with prominent single to multiple nucleoli (x1000, Giemsa); Immunocytochemistry showing; d) CD45: positive (x400); e) CD20: positive (x100); f) TTF-1: negative (x400).
The patient was evaluated for primary versus secondary lymphoma of thyroid. This patient was not reported with fever, pain, change in voice, palpitations and cold or heat intolerance. He was euthyroid with no past history of thyroid disease or medications for it. His complete blood count was normal. Patient was not immunocompromised. He reported no personal or family history of autoimmune disorder, no cervical irradiation or family history of thyroid cancer. Lymphadenopathy and hepatosplenomegaly were absent. Contrast-Enhanced Computed Tomography (CECT) revealed a large poorly enhancing solid mass in both thyroid lobes measuring 4.2×5.3×6.6 cm, extending to pre and paravertebral region, multiple similar small rounded soft tissue nodules noted in right lobe of thyroid. However, minimal extrathyroidal extension seen in left thyroid lobe, associated with insignificant reactive lymphadenopathy. Whole body imaging was done which excluded other foci of lymphomas.
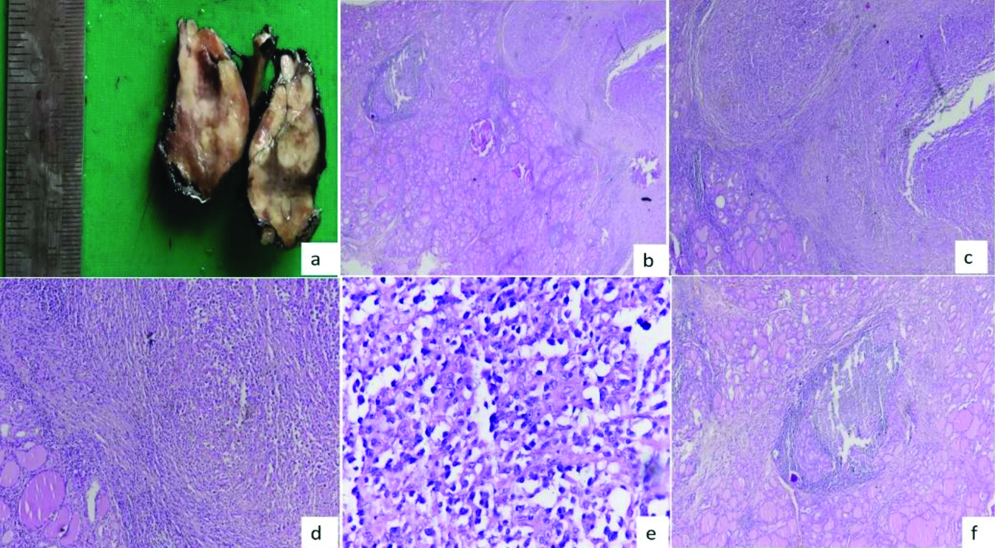
Patient underwent right hemithyroidectomy for further evaluation of lymphoma. Macroscopically, the specimen was soft globular measuring 4×2.5×2.5 cm. Cut-section showed conglomerated grey-white nodules, altogether approximately 2×1.7×1.4 cm [Table/Fig-3a]. Haematoxylin and eosin stained section showed tumour mass and adjacent thyroid parenchyma [Table/Fig-3b]. Tumour mass showed cells arranged in sheets [Table/Fig-3c,d]. Tumour cells showed high N:C ratio, large irregular hyperchromatic nuclei, prominent nucleoli and moderate amount of cytoplasm [Table/Fig-3e]. Infiltration and destruction of thyroid follicles by tumour cells were seen. Foci of chronic lymphocytic thyroiditis was noted in adjacent thyroid parenchyma [Table/Fig-3b,f]. The differential diagnosis was lymphoma and anaplastic carcinoma of thyroid. Presence of large cells with numerous lymphoglandular bodies in the background was suggestive of lymphoma. IHC was done with the available markers to rule out anaplastic carcinoma. IHC [Table/Fig-4] showed diffuse intense immunopositivity with CD45, CD20 and PAX-5, focal positivity for MUM1 and negative for CD3, CD10, BCL-6 and Thyroid transcription factor 1. Reactive T-Cells were highlighted by CD3. The biopsy with IHC analysis confirmed DLBCL, non-germinal cell type, which was primary in thyroid. According to the Ann Arbor guideline for PTL, the patient had stage IE disease at diagnosis (involvement of thyroid gland). The patient was treated with three cycles of CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone). He is now under 11 months of follow-up which was uneventful.
a) Macroscopic feature of right lobe of thyroid, showing greyish-white conglomerated nodules on cut surface. Microphotograph of Haematoxylin and eosin stained sections showing; b) tumour mass and adjacent thyroid parenchyma (x20, H&E); c) Tumour mass arranged in sheets (x40, H&E); d) Infiltration and destruction of thyroid follicles by tumour cells (x100); e) Atypical lymphoid cells with high N:C ratio, large irregular hyperchromatic nuclei, prominent nucleoli and moderate amount of cytoplasm (x400); f) Focus of chronic lymphocytic thyroiditis (x40, H&E).
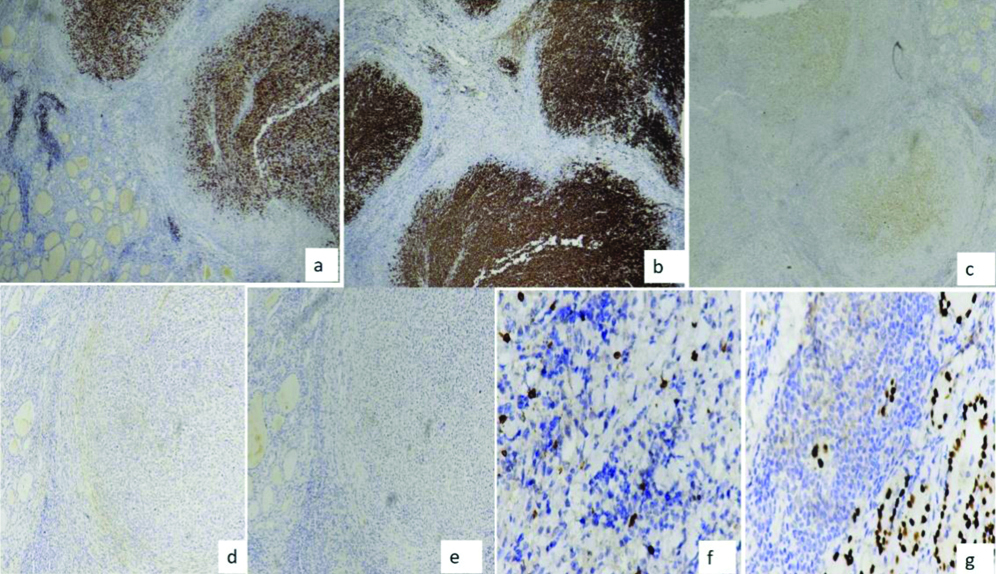
Immunohistochemistry showing: a) PAX-5: strongly positive (x400); b) CD20: strongly positive (x400); c) MUM-1: positive (x400); d) CD10: negative (x100); e) BCL-6: negative (x100); f) CD3: negative (x400); g) TTF-1: negative (x400).
Discussion
Occurrence of PTL in male patient is extremely rare. This case was unique as found in male patient who presented with progressive thyroid swelling without previous thyroid abnormality or medication for it. PTL refers to a lymphomatous involvement of thyroid gland at diagnosis with or without involving regional neck lymph nodes and without contiguous spread or distant metastases from other site [1-3]. PTL is comprising of 1-5% of thyroid malignancy, and 1-2.5% of all malignant lymphomas. PTL is more prevalent in females in their seventh decade of life [4-6]. The annual incidence rate of PTL is 2:1 persons per million [7]. Most PTL are NHL, among which DLBCL is predominant accounting for 50-80% of PTL and 20- 30% by Mucosa Associated Lymphoid Tissue lymphoma (MALT) predominantly extranodal marginal type [8,9]. Other PTL that can occur are follicular lymphoma, Small Lymphocytic Lymphoma (SLL), Burkitt’s lymphoma, Hodgkin’s and T-cell lymphoma [10-12]. It presents with a rapidly enlarging swelling and may appear like anaplastic thyroid carcinoma both clinically and histopathologically [7-9,12]. Dyspnea, dysphagia and change in voice are the common symptoms in PTL [10,11]. Secondary Thyroid Lymphoma (STL) indicates lymphoma that comes from non-thyroidal tissue and metastasise to thyroid gland. Patients with STL have higher mortality rate as opposed to PTL [2,6].
Presence of Hashimoto’s Thyroiditis (HT)/Chronic Lymphocytic Thyroiditis (CLT) increases the risk for developing PTL around 40-80 times greater as compared to general population. It is probably due to chronic antigenic stimulation which leads to malignant transformation [6-8]. Evaluation of HT to PTL can occur in around 0.5% of cases, which may take around 25 to 30 years [3,5]. In this case, CLT was detected antecedently during histopathological examination which may be the cause for lymphoma. Most patients of PTL are euthyroid, but hypothyroidism can occur due to replacement of thyroid parenchyma by lymphomatous process [3,8].
It is a difficult task for a pathologist to diagnose PTL on FNA cytological smear. [2,8]. In this case it could be possible due to presence of many large dyscohesive cells, pleomorphism with prominent nucleoli, mitotic figures and presence of lymphoglandular bodies in the background and with the help of Immunocytochemistry (ICC). Anaplastic carcinoma is the close differential diagnosis, which generally shows dyscohesive pleomorphic round to oval or spindle shaped cells with lack of lymphoglandular bodies [7].
Ultrasonography guided FNAC is preferred to overcome false negative diagnosis [1-3]. FNA material can also be utilised for flow cytometry, IHC study and in molecular technique like polymerase chain reaction [3,6]. Inspite of recent advances in radiological imaging, histopathological examination remains the gold standard for diagnosing PTL [1,11].
Chemoradiotherapy in combination is the gold standard for aggressive PTL. PTL is highly radiosensitive [5,10]. R-CHOP alone in young patients or with radiotherapy in patients >60 years of age, is the standard treatment of localised aggressive lymphoma [1,7,9]. Surgical management has no added benefit in patient with DLBCL [2,8,11].
Lymphoma arising primarily from the thyroid gland has better prognosis compared to lymphoma involving other organ [10]. According to Ann Arbor staging criteria, this patient was at stage IE (involvement of thyroid gland) and doing well after 11 months of treatment. Long-term follow-up is essential as recurrence may occur [2,3,10].
Conclusion(s)
The diagnostic accuracy of FNAC of thyroid swelling is not uniform for the diseases. Biopsy together with immunohistochemistry remains the gold standard for diagnosis of lymphoma. A rapidly enlarging thyroid swelling should be considered in differential diagnosis of lymphoma. Multimodality approach is necessary for the management of PTL. Further studies are required which can help to assess the risk of evaluation of chronic lymphocytic thyroiditis to lymphoma.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? NA
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 15, 2020
Manual Googling: Nov 11, 2020
iThenticate Software: Dec 07, 2020 (11%)
[1]. Kakkar A, Purkait S, Agarwal S, Mallick S, Gogia A, Karak AK, Primary thyroid lymphoma: A series from a tertiary care center in Northen IndiaCancer Journal 2019 15(3):669-75.10.4103/jcrt.JCRT_135_1731169238 [Google Scholar] [CrossRef] [PubMed]
[2]. Peixoto R, Pinto JC, Soares V, Koch P, Gomes AT, Primary thyroid lymphoma: A case report and review of the literatureAnn Med Surg (Lond) 2017 13:29-33.10.1016/j.amsu.2016.12.02328053701 [Google Scholar] [CrossRef] [PubMed]
[3]. Gupta N, Nijhawan R, Srinivasan R, Rajwanshi A, Dutta P, Bhansaliy A, Fine needle aspiration cytology of primary thyroid lymphoma: A report of ten casesCyto Journal 2005 2:2110.1186/1742-6413-2-2116336672 [Google Scholar] [CrossRef] [PubMed]
[4]. Shultz CL, Guerrero MA, Primary thyroid lymphoma: A comprehensive review of contemporary managementJ Surgery 2013 1(1):6 [Google Scholar]
[5]. Onal C, Li XY, Miller RC, Poortmans P, Constantinou N, Weber DC, Treatment results and prognostic factors in primary thyroid lymphoma patients: A Rare Cancer Network studyAnnals of Oncology 2011 2:156-64.10.1093/annonc/mdq31020587509 [Google Scholar] [CrossRef] [PubMed]
[6]. Alyami H, Alsofyanib T, Bshaitc MB, Al-Osaila EM, Primary Diffuse B-Cell Thyroid LymphomaCase Rep Oncol 2018 11:505-10.10.1159/00049088330140214 [Google Scholar] [CrossRef] [PubMed]
[7]. Verma D, Puri V, Agarwal S, Bhaskar A, Primary thyroid lymphoma: A rare diseaseJ Cytol 2014 31:218-20.10.4103/0970-9371.15113925745292 [Google Scholar] [CrossRef] [PubMed]
[8]. Papadakis G, Tertipi A, Papazian M, Moustakas K, Pappas A, Case report: Primary thyroid lymphoma presenting as a rapidly enlarging thyroid massEndocrinol Metab Int J 2014 1(1):04-06.10.15406/emij.2014.01.00002 [Google Scholar] [CrossRef]
[9]. Amar A, Singhal S, Chandra GS, Dua H, Primary thyroid lymphomaApollo Med 2019 16:58-60. [Google Scholar]
[10]. Kumar R, Khosla D, Kumar N, Ghoshal S, Bera A, Das A, Survival and failure outcomes in primary thyroid lymphomas: A single centre experience of combined modality approachJ Thyroid Res 2013 2013:26903410.1155/2013/26903424163775 [Google Scholar] [CrossRef] [PubMed]
[11]. Thieblemont C, Mayer A, Dumontet C, Barbier Y, Callet-Bauchu E, Felman P, Primary thyroid lymphoma is a heterogeneous diseaseJ Clin Endocrinol Metab 2002 87(1):105-11.10.1210/jcem.87.1.815611788631 [Google Scholar] [CrossRef] [PubMed]
[12]. Chen C, Yang Y, Jin L, Dong L, Zhang X, Xiang Y, Primary thyroid T-lymphoblastic lymphoma: A case report and review of the literatureInt J Clin Exp Pathol 2014 7(1):443-50. [Google Scholar]