For all age groups, a physically active lifestyle is important. There are many motives to engage in sports activities such as relaxation, socialisation, wellness, conservation and health enhancement [1]. Participation in sports provides possible benefits for people of all ages, such as improving psychosocial health, functional ability and reduces risk of coronary heart disease [2].
Injuries during sport tend to be unavoidable, and upto 30% to 40% of all incidents in children and adolescents occur during sports [3]. Dental injuries are the most common form of orofacial injury suffered during sports participation [4]. Contact sports are characterised as sports in which players engage physically with each other, attempting to prevent the opposing team or individuals from winning [5]. In India, collision and contact sports like football, basketball, skating, karate, boxing, judo, martial arts, gymnastics and volleyball are generally associated with dental and soft tissue injuries [6].
Dental injury among contact sport athletes usually includes the upper front teeth which can be chipped, broken, loosened or avulsed. This injury can be severe, affecting appearance, voice, and ability to eat [7]. Dental trauma in sports is different from other dental trauma, because it can be easily avoided and there is also the potential of significantly reducing the incidence rates by using mouthguards to protect both dental and periodontal structures [8,9]. Since the growing popularity of contact sports and motivation to participate at an early age, the dental professional’s role has become more important in the prevention of dental and orofacial injury. With this in mind, children, coaches, parents, and dental community members should be aware of how individuals involved in sports activities are at risk for dental trauma [10].
Dental practitioners have long promoted the use of mouthguards in sports activities [11]. Mouthguard is defined as a “resilient device or appliance placed inside the mouth to reduce oral injuries, particularly to teeth and surrounding structures. Despite national medical and dental associations urging the use of properly designed headgear and mouthguards to reduce head, facial and dental injury, this was not very common among children in India. Surveys of parents regarding the indications for mouthguard usage reveal a lack of complete understanding of the benefits of mouthguard use [12-15]. Many sports medicine professionals described inappropriate coaching as a cause of an injury [16]. Many young athletes are never taught the right methods or tactics to practice their sports because coaches actually do not have the right knowledge base to teach correct sporting techniques [17].
Despite the high incidence of trauma during sports, sports dentistry has been a neglected field throughout the world and in India too. A comprehensive literature review [7,9-11] revealed scant data on Indian coaches and children’s perception of knowledge, understanding and prevention of dental injuries. So, present study was undertaken to assess the understanding and knowledge of sport children and sports coaches in Vadodara, India regarding various aspects of sport-related orofacial injuries as they have a direct impact on the trainees.
Materials and Methods
This cross-sectional study was carried out from August 2019 to October 2019 at three sports complexes in Vadodara, Gujarat after approval by the Institution’s Research Ethics Committee (SVIEC/ON/DENT/SP/19111). Permission was taken from the Chief Executive Officer of various sports complex.
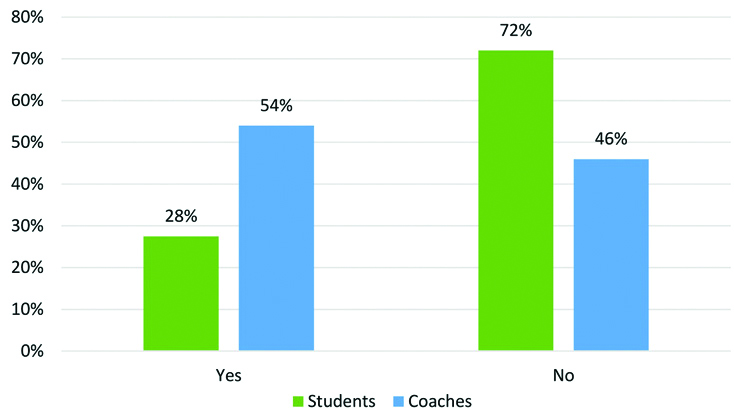
Sample size calculation: Formula used for the calculation of sample size was
Where N=Population size, 300 (considering children participated in various sports complexes);
e=Level of Precision (0.05) at 95% Confidence interval
Hence n=240.
Where N, is Population size and e is the level of precision
Where, N=300 (considering participation of children in various sports complexes) e=0.05 at 95% Confidence interval n=240
Same formula was applied for sample size calculation for coaches. Where, N=70 (considering coaches in various sports complexes) e is 0.05 at 95% Confidence interval n=50
Where, N=70 (considering coaches in various sports complexes);
e=(0.05) at 95% Confidence interval Hence, n=50
Therefore, final sample size was 240 for sports children and 50 for coaches.
The selection of participant children and coaches were based upon following criteria:
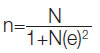
Inclusion criteria: The children aged between 6-18 years, who register to participate in different contact sports. In present study, all the coaches included were involved in training of contact sports. All the coaches were having experience of above five years. Contact sports included in the study were: contact/collision (football, martial arts, wrestling, boxing), limited contact/impact (basketball, cycling, gymnastics, skating, squash, volleyball, hockey), strenuous contact (tennis, weight lifting, swimming), moderately strenuous contact (badminton, table tennis).
Exclusion criteria: Children who were not registered in any sports complex or not playing contact sports. Children who were physically handicapped or mentally retarded children were excluded from the study.
A pilot study was conducted in which 20 closed ended questions for coaches and 18 closed ended questions for children were constructed using a multiple choice or Yes-No format, based on previous questionnaires on the topic [10,16]. Ten coaches, 10 sports children and 10 subject experts took part in the pilot study; and were excluded in the final research to test reliability; and concurrent and content validity. Ten subject experts were included in the pilot study to test if the questionnaire was accurate. Reliability was used to calculate whether variables given were stable or replicable, validity was measured whether the survey tool used in the analysis was accurate or not. Reliability obtained for the tool was 98.43%. Reliability of the tool was obtained using test-retest method. Concurrent validity of the tool was obtained by statistical calculations which was found to be more than 95% Confidence interval (t-value=1.00 and p-value=0.417). The content validity score for the entire questionnaire was calculated by the Lawshe’s (1975),
Content Validity Ratio (CVR) formula {CVR=(ne-N/2)/(N/2);
where CVR=content validity ratio, ne=number of SME panelists indicating “essential”, N=total number of SME panelists, and SME=subject matter expert} [18]. CVR for the questionnaire was 0.80, that is, 80.00% content validity. Questionnaire was modified as per the expert suggestions. The modified final version of the questionnaire was then used in the study.
The questionnaire for coaches contained 20 questions, including, what sport(s) they coached, the experience they had as a coach, the rate of oral trauma they had seen during sport activities, the reasons for the dental injuries, whether they advised any protective devices.
The children’s questionnaire included 18 closed ended questions, including type of sport involving children; time spent performing that sport, whether there were any injuries to the dental and soft tissues. If they knew that the avulsed tooth can be repositioned, and also the extraoral time during which the teeth can be repositioned. If they’re using mouthguard during sport.
Four questions were common from the two questionnaires, such as i) whether they understood that an avulsed tooth can be repositioned; ii) the extraoral time during which teeth can be repositioned; iii) which medium used to carry avulsed tooth; iv) whether they used mouthguards and reasons for not using mouthguards Consent form was obtained by each participant prior to questionnaire distribution. Questionnaires were distributed by principal investigator to coaches and sports children in-person, and were collected back after 15 minutes.
Statistical Analysis
The data collected were placed into a Microsoft Excel 2016TM and analysed using the SPSS system 23 (Statistical Package for the Social Sciences, version 23.0, SPSS Inc., Chicago, IL, USA) on a basis of percentage and proportion. For the questions that were commonly asked to coaches and sports children, Chi-square tests were applied and p≤0.05 was considered statistically significant.
Results
A total of 240 children from sports and 50 coaches from various Vadodara sports complexes were enrolled and same number of children and coaches were participated in the study. There were no drop outs and all the participants responded to questionnaire. Furthermore, this present study also compared important questions such as the use of mouthguards, carrying medium for avulsed tooth in both sport children and coaches.
Sports Children
Out of all the sports children, male children (62.3%) were more than female children (37.7%). Their age ranged from 6 to 18 years and mean age was 11.2 years.
Majority 105 (43.8%) sports children were in primary school, 81 (33.8%) were in secondary school level, and 54 (22.4%) were from higher secondary level. Children participated in various sports ranging from contact sports, limited contact sports, strenuous contact and moderately strenuous contact [Table/Fig-1].
Distribution of Sports Children into different type of sports.
The responses of various questions regarding orofacial injuries due to various types of sports and their prevention were obtained from sports children and were analysed [Table/Fig-2].
Perception and knowledge of sports children regarding orofacial injury.
| Sr No. | Questions | Answers/option | Response N (Total sports children=240) | Percentage (%) |
|---|
| 1. | Does your coach/sports club make you aware of sports related injuries or how to prevent it? | Yes | 190 | 79.2 |
| No | 50 | 20.8 |
| 2. | Have you ever injured your face while playing sports? | Yes | 100 | 41.7 |
| No | 140 | 58.3 |
| 3. | Did you have any soft tissue injuries in the following parts? | Face | 45 | 18.8 |
| Lip | 42 | 17.5 |
| Tongue | 8 | 3.3 |
| Nose | 36 | 15.0 |
| None of the body parts mentioned above | 109 | 45.4 |
| 4. | Did you have any hard tissue injuries in the following parts? | Teeth | 25 | 10.4 |
| Facial bone | 17 | 7.1 |
| Bone of legs | 40 | 16.7 |
| Bone of hands | 36 | 15 |
| None of the body parts mentioned above | 122 | 50.8 |
| 5. | Did you cut you lip/tongue/cheek while playing sports? | Yes | 55 | 22.9 |
| No | 185 | 77.1 |
| 6. | Did your chip/fracture your teeth while playing sports? | Yes | 21 | 8.8 |
| No | 219 | 91.3 |
| 7. | Did your teeth come out while playing sports? | Yes | 18 | 7.5 |
| No | 222 | 92.5 |
| 8. | Have you been to dentist after sports injury? | Yes | 54 | 22.5 |
| No | 186 | 77.5 |
| 9. | Did your coach advise you to use mouthguard to prevent dental injuries due to sports? | Yes | 83 | 34.6 |
| No | 157 | 65.4 |
| 10. | Are you aware that mouthguards can prevent dental injury? | Yes | 118 | 49.2 |
| No | 122 | 50.8 |
| 11. | Do you use mouthguards?* | Yes | 33 | 15.8 |
| No | 207 | 84.2 |
| 12. | If yes which type* | Prefabricated | 29 | 12.1 |
| Customised | 4 | 1.7 |
*Question number 11&12 were interconnected. Number of sports children answered yes and no were 33 and 207, respectively, so n=33 in question 12.
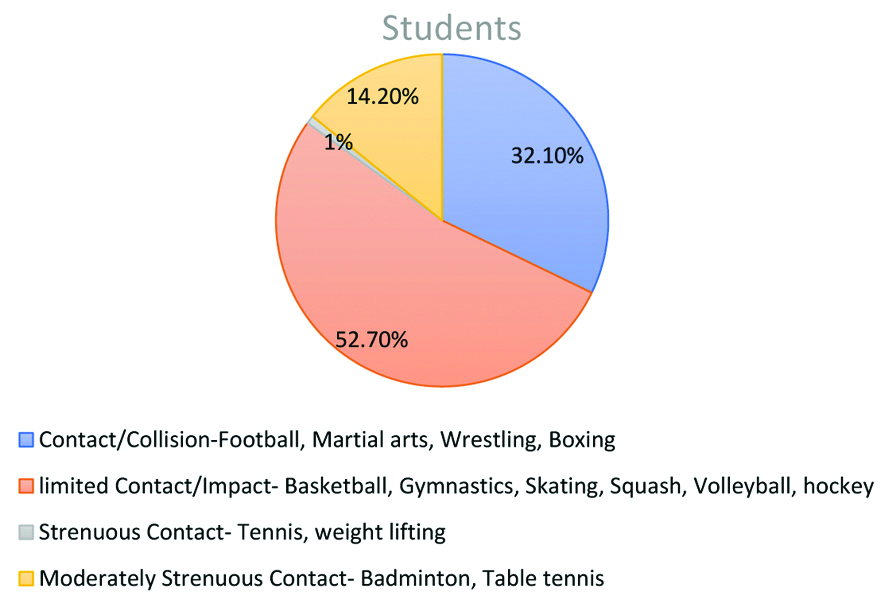
Various reasons for not using mouthguards by sports children were recorded [Table/Fig-3].
Reason for not using mouthguard during sports for sports children.
Coaches
A total of 50 coaches from various sports complexes participated in the study. Male coaches 42 (84%) were more than female coaches 8 (16%). Their age ranged from 31 to 54 years and mean age was 41.02 years. They had mean experience of 10.5 years.
Majority coaches that is 29 (58%) were giving coaching in limited contact sports that is basketball, skating, volleyball, hockey. The perception and knowledge of coaches regarding orofacial injury and prevention of that injury were analysed [Table/Fig-4].
Knowledge and perception of coaches regarding orofacial injuries.
| Sr No. | Questions | Answers/Option | Response n (Total sports children=240) | Percentage (%) |
|---|
| 1. | Are sports injury and their prevention a part of your syllabus during the degree/diploma in physical education? | Yes | 46 | 92.0 |
| No | 4 | 8.0 |
| 2. | Type of sports in which you give coaching | Contact/collision | 12 | 24.0 |
| Limited contact/impact | 29 | 58.0 |
| Strenuous contact | 0 | 0 |
| Moderately strenuous contact | 9 | 18.0 |
| 3. | Do sports activities supervised by you cause injuries to head, face or teeth (dental trauma)? | Yes | 41 | 82.0 |
| No | 9 | 18.0 |
| 4. | Have you interacted with medical or dental experts regarding safety measures in sports?† | Yes | 32 | 64.0 |
| No | 18 | 36.0 |
| 5. | If yes, then where did this interaction occur?† | Casually | 8 | 16.0 |
| At seminars | 1 | 2.0 |
| During Sports career | 23 | 46.0 |
| During the sports/physical education degree course | 0 | 0 |
| 6. | Are girls more concerned about sports injuries? | Yes | 30 | 60.0 |
| No | 20 | 40.0 |
| 7. | How often have students under your care sustained facial or dental injury (in the last year)? | None | 13 | 26.0 |
| 1-5 | 37 | 74.0 |
| 6 or more | 0 | 0 |
| 8. | What were the reasons for the sports injuries?* | Falls | 23 | 46.0 |
| Collison | 3 | 6.0 |
| Hit by a ball/Hockey/Hard object | 16 | 32.0 |
| Fight between players | 18 | 36.0 |
| Any other | 8 | 16.0 |
| 9. | Could you describe the injuries?* | Bruise | 13 | 26.0 |
| Cut lip, cheek, tongue | 35 | 70.0 |
| Broken tooth, avulsed tooth | 5 | 10.0 |
| Fracture of facial bones | 0 | 0 |
| Loss of consciousness/concussion | 6 | 12.0 |
| 10. | Do you advice use of mouthguard to sports person?‡ | Yes | 31 | 86.0 |
| No | 19 | 14.0 |
| 11. | If no, what is the reason for not advising mouthguard?‡ | Not aware about facilities available in city | 7 | 14.0 |
| It is uncomfortable | 10 | 30.0 |
| According to me it is not important | 2 | 4.0 |
| 12. | If yes, then which type of mouthguard will you prefer?‡ | Pre-fabricated | 22 | 44.0 |
| Customised | 9 | 18.0 |
| 13. | How often were the injuries related to non-use of a mouthguard? | Always | 4 | 8.0 |
| Sometimes | 31 | 62.0 |
| Never | 15 | 30.0 |
| 14. | Do you feel the use of protective devices will? | Reduce efficiency while playing sports | 25 | 50.0 |
| Enhance efficiency while playing sports | 25 | 50.0 |
| 15. | Did the sports injury ever prevent a student from continuing the sport? | Yes | 34 | 68.0 |
| No | 9 | 18.0 |
| Any other | 7 | 14.0 |
| 16. | Do parents of sports persons express their concerns regarding sports-related injuries to you? | Yes | 47 | 94.0 |
| No | 3 | 6.0 |
| 17. | Are the concerns of these parents, in your opinion | Appropriate | 50 | 100 |
| Inappropriate | 0 | 0 |
*coaches could choose more than 1 options. †Question number 4 and 5 were interconnected. Number of coaches answered yes and no were 32 and 18 respectively, so n=32 in question 5.
‡Question number 10, 11 and 12 were interconnected. Number of coaches answered yes and no were 31 and 19, respectively, so n=19 in question 11 and n=31 in question 12
Coaches and Sports Children
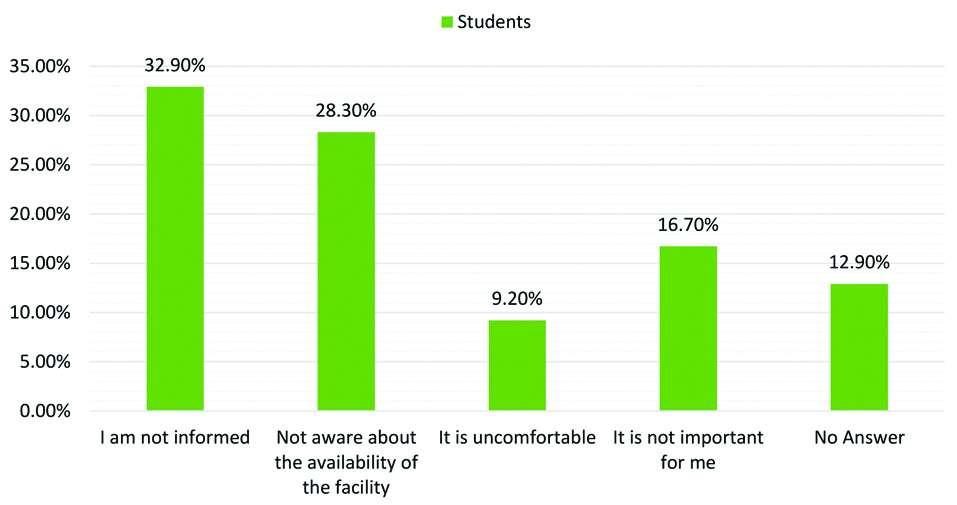
A 28% sports children and 54% coaches knew that it was possible to re-implant the teeth (p<0.05) [Table/Fig-5].
Responses of sports children and coaches regarding replantation of avulsed tooth in oral cavity.
*Chi-square test (p≤0.05) is statistically significant
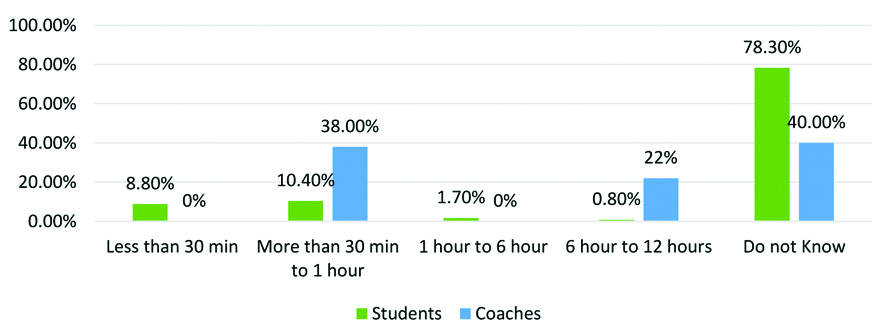
Most suitable time period for re-implantation of avulsed tooth in oral cavity is 30 minutes. Only 8.8% children and none of the coaches knew most suitable time span in which tooth should be re-implanted in oral cavity (p=0.03) [Table/Fig-6]. There was significant difference between responses of coaches and sports children that clearly suggested lack of knowledge in coaches about exact time period to re-implant avulsed teeth.
Responses of sports children and coaches regarding time period within which Avulsed tooth should be re-implanted into oral cavity.
*Chi-square test (p-value 0.03)
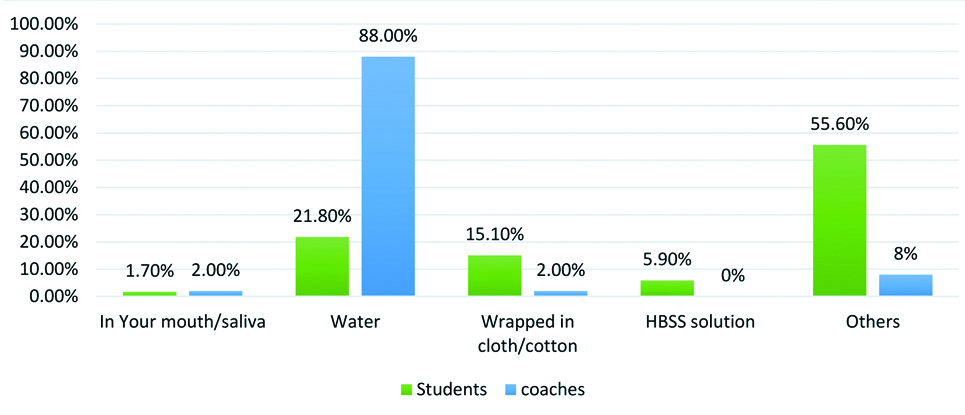
Various medium can be used for carrying an avulsed tooth. A 5.9% sports children knew correct response that HBSS solution was the best for carrying avulsed tooth while none of the coaches knew about HBSS solution (p=0.08) [Table/Fig-7].
Knowledge of sports children and coaches regarding medium for carrying the avulsed tooth in case of orofacial injury.
*Chi-square test (p-value 0.08) is statistically significant
Discussion
The present research was based on the understanding and awareness of dental injuries in the sports children and coaches. In this study, both sports children and coaches were enrolled to test their understanding and comprehension of trauma-related dental injuries so that investigators can find out what are the various reasons for the trauma. Gap in transmitting the information from coaches to children was also assessed as if, coaches are well qualified and gave proper instruction to sports children then why sports children do not follow the instructions. All this information provided useful inputs for making/modifying a guideline to prevent sports children from having the trauma.
Knowledge of sports children: Injury was also regarded as a natural consequence of participation in organised sports. However, several accidents, particularly those arising from a lack of adequate, well-supervised training and involvement, may be preventable. The present study shows that 41.7% of sports children have suffered one or more forms of orofacial injury during sport activities. This result is higher than studies performed by Tulunoglu I, Ozbek M and Persic R et al., where 22.3 and 20.4% of participants registered oral injury, respectively [19,20].
The most frequent sports injury reported was laceration on lip, tongue and cheek (22.9%), followed by chipping/fracture of teeth 8.8%. Hard tissue injuries namely fracture of legs and facial bone reported were 16.7% and 7.1%, respectively. Kay EJ et al., in his study suggested that, these injuries incurred in children when they fall on their face or they are hit by hard objects from sports equipments and collision between players [21].
Knowledge of coaches: A 74% of the coaches choose the frequency of orofacial injuries in range of 1-5 in present study by their students in last 1 year. A 62% of coaches believed that these injuries were sometimes related to non-use of mouthguards while 30% of coaches believed that it was never related to non-use of mouthguard and 8% of coaches believed that it was always related to non-use of mouthguards [Table/Fig-4]. Similar study done by Lehl G found the frequency of orofacial injury between 1-5 [16]. Frequency of injury due to non-use of protective devices found out by various authors were; Lehl G 82%, Garon MW et al., 63%, Mc Nutt T et al., 75% and Berg R et al., 48% [16,22-24]. In the present study, majority of the injuries occurred due to falls (46%) followed by fight between players (36%) and hit by an object (32%). The most common type of injury were cut lip, cheek, tongue (70%) followed by bruising (26%), loss of consciousness/concussion (12%) and broken or avulsed tooth (10%) [Table/Fig-4]. In a similar study, Blinkhorn found that falls and collision were the main cause of injury [25]. Research done by Berg R et al., found that the most common injury was a cut lip, tongue or cheek (82.4%) and proposed that this form of injury would be a cause of considerable concern, as it may indicate a tooth object impact in which serious harm to the tooth was prevented [24].
Current research revealed that 62% of coaches reported injuries were sometimes related to non-use of protective devices. In other studies, 63-75% such injuries occurred when a mouthguard was not used [22,23]. It is a promising finding that 64% of the coaches had interacted with medical or dental experts regarding injury prevention and 50% of the coaches found that protective devices enhance the efficiency of the players.
Knowledge of coaches and sports children regarding common questions: In the present study, 66 out of 240 (27.5%) sports children and 50 out of 27 (54%) coaches were aware that it was possible to re-implant the avulsed tooth. Studies carried out by Ersin N et al., found that 34.7 percent of individuals were aware of teeth re-implantation [26]. In the present study 78.3 % sports children had no knowledge regarding period of time during which avulsed tooth should be re-implanted and 21.8% sports children believed that water was best suitable medium for transporting avulsed tooth. Similar research performed by Donaldson M and Kinirons MJ found that 31.6% of individuals had no knowledge of the period of time during which avulsed teeth should be re-implanted and only 8.3% understood that avulsed teeth could be transported in liquid medium (milk, water, saliva) [27].
Regarding the usage and awareness of mouthguard, 15.8% of the athletes were utilising it. However, 49.2% of those athletes knew that a mouthguard can prevent orofacial injuries. This result is corroborating with the studies done by Goswami M et al., where 20.9% of athletes utilise mouthguard and 71.3% knew that mouthguard can prevent orofacial injuries [10].
Present study suggested that there is a lack of knowledge of re-implantation of the tooth, period span of re-implantation of the tooth and storage medium of carriage of the tooth in coaches so, that it is difficult to educate the sports children for the same, and in the same way sports children were aware that mouthguard can prevent dental injuries but, very few of them wear. Most of them indicated that they have not been told or that they were not aware about the availability of mouthguards or source from where it can be procured.
Based on the present study investigators put forth some recommendation. Recommendations were divided into three subcategories, recommendations for sports authorities, recommendations for sports coaches and recommendations for sports children.
Recommendations for sports authorities: 1) General physical and emotional health screening should be conducted for children prior to admission in contact sports; 2) Authorities should take history of tetanus toxoid vaccination; 3) Authorities should have record of blood groups of all children. 4) All the coaches should be trained for Basic Life Support (BLS). All the safety measures should be there in every section of sports complexes; 5) Sports authorities should have collaboration with the dentist. First aid kit should be available in each section of sports complex; 6) The sports complex authority should provide a list of shops from which parents can buy the protective kit and dentist information from whom they can fabricate the mouthguards.
Recommendations for sports coaches: 1) Coaches should have certified training with BLS course certificate; 2) Coaches should be trained and have thorough knowledge regarding first aid kit. Trauma management should be included in the curriculum of coaches; 3) If children are not coming with protective devices recommended by coach they should not be allowed to play at that day; 4) Coaches should give clear instructions to the sports children and provide brochure which contains instructions for safety measures.
Recommendation for sports children: 1) Should be aware about rules while playing contact sports; 2) Should follow proper instruction given by coach. 3) Should wear protective devices while playing contact sports. 4) Sports children should have an ID card including their name, blood group and contact number of parents.
Limitation(s)
Less sample size and no closed ended questions have been used in questionnaires.
Conclusion(s)
Many participants were aware of the importance of mouthguards in injury prevention but most did not use mouthguards due to lack of support from coaches. Awareness of the medium for carrying avulsed teeth was obviously missing. It appears that the use of protective devices among coaches is increasingly recognised, but its use was still dependent on the type of game. The dentist not only give coaches adequate information about protective equipment, but also advise patients, especially children, adolescents and young adults, on participation in sports so that adequate protection can be taken.
After time gap of three-month, re-assessment of knowledge and awareness about mouthguard should be done. Motivate and educate the children as well as coaches by making education material. We could increase awareness in the parents about mouthguard by involving them into the study. Take home message from this study is to educate and aware coaches, parents and sports children regarding the orofacial injury and their prevention. Most of the traumatic injury can be prevent by using protective devices. Awareness can also be increased in parents about mouthguards by involving them in future studies.