The epidemic of DM is prevalent and India will soon become the global capital of this metabolic derangement, causing multiple morbid complications and increased mortality [1]. DM is acknowledged to be one of the most common risk factors for developing Chronic Kidney Disease (CKD) and the economic burden of this chronic disease is overwhelming especially in lower socio economic societies such as India [2]. The risk for developing T2DM increases with age, sedentary lifestyle, obesity-promoting environment, energy imbalance that may impact multiple aspects of physical and psychological aspects of health during the progression of the disease. Renal complications of the disease are especially notable and it is estimated that 20% to 40% of T2DM eventually end up with kidney failure [3].
Diabetic kidney disease is a micro-vascular complication of DM and it has been suggested that it is initiated by a dysregulated metabolic milieu that includes hyperglycaemia, hyperlipidemia, and insulin resistance. It has been further hypothesised that this is a manifestation of altered glomerular permselectivity caused by a disruption of fenestrated glomerular endothelium and its glycocalyx [4]. Health hazards due to this will pose a big challenge in the next century and thus, priority needs to be given to its prevention through alternative and complementary adjuvant methods of therapy [5]. Because of the potential threat to Quality of Life (QoL) and the chronic nature of diabetes, many people turn to complementary therapies seeking help to control the disease [6]. Studies in diabetic patients have reported that yoga practice leads to a significant improvement in the anti-oxidant status and reduced oxidative stress levels, and Body Mass Index (BMI) [7].
Yoga has shown promising results as an adjuvant therapy in prevention, management and rehabilitation of psychosomatic and stress disorders including DM [8]. Gordon L et al., concluded that yoga had preventive and protective effects in end-stage renal patients through a reduction in oxidative stress [9]. Pandey RK et al., concluded that yoga is effective and safe as positive changes in renal function and QoL have been reported in CKD patients [10]. It was suggested that yoga helps in preventing as well as managing complications that may arise due to T2DM [11]. Madanmohan et al., concluded that yoga was beneficial as a complementary therapy along with standard medical care in peri and post-menopausal diabetic patients [12]. Mechanisms suggested for yoga and its beneficial effects include an optimal state of autonomic balance improving cardio-respiratory efficiency with reduction in overall consequences of stress on the body and mind [13].
Keeping the above in mind, the present single blinded RCT was planned to study the effect of 4 months of a thrice-weekly adjuvant yoga therapy on the renal profile of patients with DM. This work is part of a larger study based on the effects of adjuvant yoga therapy in diabetic patients. A part of the study dealing with improvements in lung function has already been published [14].
Materials and Methods
This randomised controlled trial of four months (November 2016 to February 2017), was undertaken as an interdisciplinary collaborative work between the Centre for Yoga Therapy Education and Research (CYTER) of Sri Balaji Vidyapeeth, and the Department of Endocrinology of Mahatma Gandhi Medical College and Research Institute (MGMC&RI), Puducherry. Approval was obtained from Institutional Research Council of MGMC and RI (MGMCRI/ IRC/2017/0177), and Institutional Human Ethics Committee, Sri Balaji Vidyapeeth (PG Dissertation/2017/05/76). The study was also registered with CTRI (CTRI/2017/11/010479).
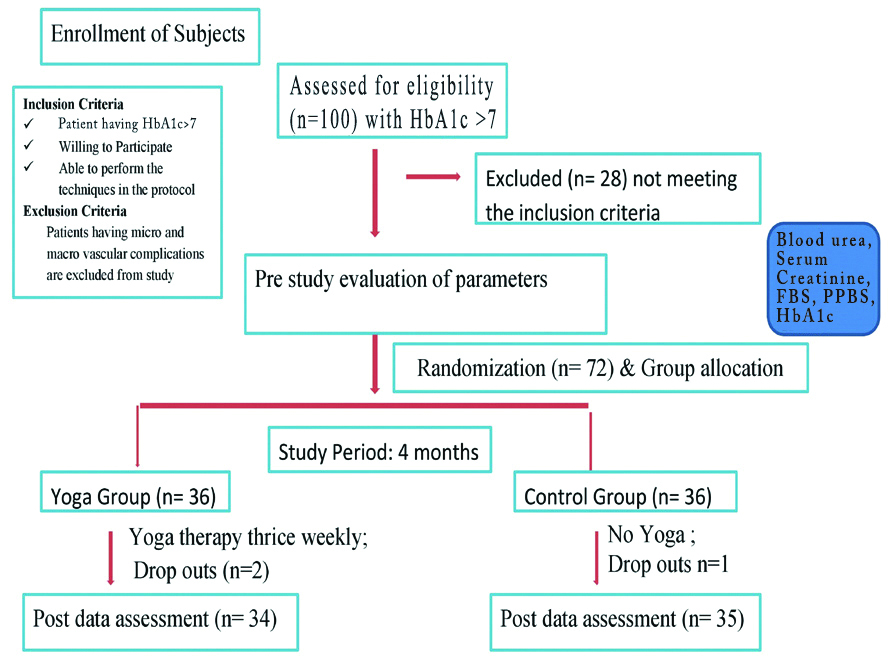
Inclusion criteria: After obtaining informed consent, diabetic patients with HbA1c more than 7%, without any renal diseases, who were willing to participate in the yoga therapy program and able to perform the techniques of the protocol were recruited for the study.
Exclusion criteria: Those who had clinical evidence of complications such as nephropathy, neuropathy and retinopathy were excluded from the study.
Simple random sampling method was followed and 100 consecutive diabetic patients who attended the diabetic clinic of MGMCRI were screened and assessed for eligibility as per the inclusion criteria [Table/Fig-1]. Recruited subjects were then allocated to two groups by random selection and block allocation (blocks of 4).
Statistics and Sample Size app (Version 1.0) [15] was used for sample size calculation. The formula used was:
Where, P1=0.5 or 50%; P2=0.7 or 70% (Assumed 20% increase from baseline); α=0.05; power=80% and r=1. Calculated sample size was 60, but considering a 20% drop out rate, the final sample size obtained was 72 and the selected patients who satisfied inclusion criteria were then randomised to yoga group (36 patients) who received an hour of yoga training at CYTER thrice weekly (Monday, Wednesday and Friday) for 4 months along with standard medical management.
Patients were followed-up rigorously by weekly telephonic conversations. Control group (36 patients) received only standard medical management (Standard medical care was provided through the Endocrinology Outpatient Department (OPD) and medications included oral hypoglycaemic drugs (sulphonylureas/biguanides/glitazones) or insulin used for glycaemic control) and were advised about the importance of diabetic diet apart from their routine activities. Yoga group subjects received Yoga training with similar dietary advice along with the medical management and were motivated for home practice. They were advised to maintain a diary to evaluate compliance. Despite the best efforts, two patients dropped out due to personal reasons in yoga group and 34 patients (22 male and 12 female) with mean age 51.85±7.60 years completed the experimental wing of the four month study. One patient dropped out in control group and hence, 35 patients (25 male and 10 female) with mean age 49.6±5.88 years completed the other wing.
Yoga therapy sessions were conducted at CYTER [Table/Fig-2] by trained and qualified yoga therapists. Components of yoga therapy protocol included yogic counseling, preparatory practices, brahma mudra, chandra nadi, and bhramari pranayamas, shavasana relaxation, and a series of 15 asanas, mudras, and pranayamas collectively known as Hathenas in the Gitananda (Rishiculture Ashtanga) Yoga tradition [Table/Fig-2] [16].
Yoga practices (given thrice a week for 4 months) and their duration [17].
| Yoga practices | Duration (min) |
|---|
| Hathenas (15 specialised techniques to enhance prana flow into all sections of the lung consciously) | 30 |
| Chandranadi pranayama (exclusive left nostril breathing with mindfulness) | 5 |
| Brahma mudra (movements of the head to four directions: Namely right, left, up and down with the breathing and usage of akara, ukara, ekara, and makara nada) | 5 |
| Bhramari pranayama (bumble bee sound made on the exhalation while using shanmukhi mudra to create introspectional awareness of the five senses) | 5 |
| Shavasana (supine relaxation of all body parts in sequence from toes to head coupled with slow and conscious deep breathing) | 15 |
| Total | 60 min |
The parameters such as Fasting Blood Sugar (FBS), Postprandial Blood Sugar (PPBS), HbA1c, blood urea and serum creatinine were recorded for all the subjects before and after 4-month study period to assess effects of yoga therapy. After obtaining informed consent from the subjects, 3 mL of blood was collected in fasting state, for serum preparation. An additional 3 mL was collected into Ethylene Diamine Tetra-acetic Acid vacutainers for the preparation of plasma. All the biochemical parameters were estimated using International Federation of Clinical Chemistry (IFCC) approved methods [17].
Serum urea was measured by Glutamate Dehydrogenase method and serum creatinine was estimated by JAFFE KINETIC method in Hitachi 902 auto-analyser [18-20] at the Central Laboratory of MGMCRI. Collection and analysis of all blood samples was done by qualified technicians and they had no knowledge of the subjects and their allocation into the respective groups.
Statistical Analysis
Data were assessed using GraphPad InStat version 3.06 for Windows 95, (GraphPad Software, San Diego California USA, www.graphpad.com). Data passed normality testing by Kolmogorov-Smirnov (KS) test and hence, intra-group comparisons of pre and poststudy data was done using Student’s paired t-test while intergroup comparisons between groups was done using Student’s unpaired t-test. The p-values less than 0.05 were considered to indicate significant differences between the means. Values are given as mean±SD. *p<0.05, **p<0.01, ***p<0.001 by Student’s paired t-test for intra group comparisons and actual p-values given for intergroup comparison by Student’s unpaired t-test. Delta percentage refers to the percentage changes in values from pre to post.
Results
The results are given in [Table/Fig-3]. The initial baseline values in both the groups were comparable, except FBS. Intragroup comparisons showed significant decrease (p<0.001) in FBS, PPBS, HbA1c, blood urea and serum creatinine in patients receiving adjuvant yoga therapy. FBS, HbA1c and PPBS increased significantly (p<0.001and p<0.01, respectively) in the controls. There was no change in blood urea in the control group while there was a significant increase (p<0.01) in their serum creatinine levels. Delta percentage values showed highly significant reduction in blood urea and serum creatinine in group receiving adjuvant yoga therapy.
Comparison of FBS, PPBS, HbA1c, blood urea and serum creatinine in Yoga and control groups before and after four months of study period.
| Parameters | Yoga (n=34) | Control (n=35) | p-value |
|---|
| Pre | Post | Delta % | Pre | Post | Delta % | Pre | Post | Delta % |
|---|
| FBS mg/dl | 214.44±48.66 | 176.14±36.40*** | -0.17±0.09 | 192.12±32.75 | 197.65±33.01*** | 0.03±0.03 | 0.028 | 0.016 | <0.001 |
| PPBS mg/dL | 306.32±62.92 | 223.88±53.40*** | -0.26±0.15 | 300.05±62.49 | 305.82±63.45** | 0.02±0.04 | 0.680 | <0.001 | <0.001 |
| HbA1c % | 8.45±0.61 | 7.35±0.400*** | -0.13±0.04 | 8.13±0.71 | 8.26±0.73*** | 0.02±0.03 | 0.052 | <0.001 | <0.001 |
| Blood Urea (mg/dL) | 33.22±5.63 | 30.91±5.23*** | -0.06±0.05 | 32.63±3.34 | 33.23±3.49 | 0.02±0.06 | 0.740 | 0.034 | <0.001 |
| Serum Creatinine (mg/dL) | 1.02±0.24 | 0.82±0.19*** | -0.14±0.14 | 1.07±0.27 | 1.14±0.32** | 0.07±0.14 | 0.480 | <0.001 | <0.001 |
FBS: Fasting blood sugar; PPBS: Postprandial blood sugar; *p<0.05, **p<0.01, ***p<0.001
Intergroup comparisons showed statistical significance in FBS, PPBS, and HbA1c (p-values were 0.016, <0.001 and <0.001, respectively) as well as in blood urea and serum creatinine (p-values were 0.034, <0.001, respectively). The delta percentage values between the yoga and control groups showed significant changes in all the parameters (<0.001).
Discussion
Incidence of T2DM has been on a steep rise principally because of the sedentary and stressful lifestyle that we are exposed to now-a-days. Long term diabetes, which is the most common endocrine and metabolic condition, leads to malfunctioning of various organ systems. Emerging evidence shows that yoga as an adjuvant therapy can have significant beneficial effects in diabetic patients.
Yoga has been studied and proven effective for controlling both the symptoms and the complications associated with T2DM. It has been reported that many complications due to diabetes may be alleviated through yoga, while simultaneously enhancing their QoL. The present study revealed highly significant reductions in all glycaemic parameters (FBS, PPBS, HbA1c) in patients receiving adjuvant yoga therapy. Such healthy reductions may be attributed to yogic techniques done by the subjects such as Asanas and Pranayama which can potentially improve insulin sensitivity in muscles and tissues as well as enhance peripheral glucose uptake and utilisation. This finding is in agreement with earlier studies that have shown such reductions over different periods of time [11-13]. Several hypothesis for such biological mechanisms have been put forward as it is non-invasive and promotes relaxation in patients with minimal side-effects [10]. Such conscious relaxation is not facilitated in the control subjects and hence, the healthy changes due to the psycho-physical mechanisms are absent [21].
Diabetic nephropathy is one of the most common and difficult to manage complications of uncontrolled diabetes [22]. Hence, the present study was planned to analyse the effect of adjuvant yoga therapy on kidney function in diabetic patients. The analysis of data [Table/Fig-3] showed that there was a statistically significant difference in glycaemic indices as well as kidney function tests in yoga group as compared to control group after 4 months of yoga training. Physical fitness in patients with renal problems is so reduced that it directly affects the ability and capacity to perform activities in everyday life and occupational tasks. Evidence shows significant beneficial effects of regular exercise on physical fitness, walking capacity, cardiovascular dimensions (e.g., blood pressure and heart rate), health-related QoL and some nutritional parameters in adults with kidney diseases [23]. Yoga is a cost-effective and relatively safe, nonpharmacological method of treating blood dyslipidemia and has shown to reduce lipid levels in diabetics and obese individuals, thereby reducing the load on the kidneys, which is found beneficial especially in patients with renal disorders [24,25].
Hatha yoga has been reported to be beneficial in renal patients, as oxidative stress reduced in the population after yoga therapy in a previous study by Gordon L et al., [9]. They showed that blood urea and serum creatinine decreased significantly in yoga group along with conservative management, whereas it increased in control group who were receiving conservative management alone. Pandey RK et al., concluded that adjuvant yoga therapy is safe and that it can enhance the renal function as well as QoL in patients of CKD [10]. According to Sengupta P, yoga may prevent as well as help in management of chronic illnesses such as diabetes by reducing stress and anxiety, improving autonomic balance as well as by promoting physical health and the higher neural center functioning. A meditative state of mind is induced in practitioners of yoga, that in turn increases self awareness and such an internalised focus produces changes in neuro-hormonal mechanisms that reduce sympathetic activity [26].
Elevated blood urea and serum creatinine levels are indicated markers of kidney dysfunction [27]. Yoga with well-defined and increasingly well understood concepts of health means to restore health and wellness. These therapeutic modalities are increasingly being accepted for treating most kinds of chronic disorders such as diabetes and other neurological or nephrological problems associated with it along with the standard medical management [28]. Decrease of serum creatinine levels was found in dialysis patients; resulting from a decrease in oxidative and psychological stress, sympathetic overdrive, and inflammatory markers due to yoga [10,29]. As other trials have reported on the role of yoga in reducing blood urea and serum creatinine levels, healthier blood pressure, perfusion pressure and renal artery blood flow are factors that need further exploration in this regard as it is expected that Yoga may be able to delay onset of nephropathy in such patients. Yoga-based rehabilitation program is a simple, safe and effective clinical treatment modality in patients with renal disease [10,26,30].
In the present study, blood urea and serum creatinine showed significant decrease in yoga group with contrary increases in control group. Inter group comparison showed statistically significant difference with improvements being positive in yoga group, which is in agreement with the findings of the other studies. [10,27,29,30]. This is a vital clinical result as it implies that regular yoga therapy, applied as adjuvant to medical management may retard progression of kidney damage in diabetic patients. Such benefits may be attributed to a better sense of relaxation that induces vasodilatation by reducing sympathetic adrenergic vascular tone.
Limitation(s)
The present study is limited by the smaller sample size and the fact that the protocol was not validated by external experts though it is being routinely used at CYTER. It was also limited to a single centre and only two renal parameters were taken for analysis. Further studies needs to be done in future, involving other renal parameters to validate these preliminary results. Though a personal diary was maintained by the participants and checked by investigator to evaluate compliance, home practice varied between 10 to 30 minutes and the number of days/week of home practice also varied. This interpersonal variability from patient to patient may also be considered as a limitation and kept in mind for future studies.
This study is a part of MPhil dissertation and due to the time frame of the course; it was done for 4 months as suggested by the respected board of members of IHEC. The experimental and control subjects were all under standard medications as advised and recommended by the qualified medical practitioners of the hospital where this study was conducted and those with HbA1c more than 7% and without any renal diseases have been recruited for the study.
Conclusion(s)
Yoga has a role as an adjuvant therapy along with modern medical management of renal profile in diabetic patients. Considerable changes in blood urea and serum creatinine may occur with prolonged practice and is useful as it may retard progression to nephropathy in such patients. Yoga as an adjuvant therapy, given along with standard medical care is a relatively safe and cost effective practice to promote holistic health and wellbeing. It is expected that the results of this RCT will provide impetus for further in-depth research to evaluate efficacy of yoga as a complimentary therapy in diabetic patients with special reference to kidney diseases.
FBS: Fasting blood sugar; PPBS: Postprandial blood sugar; *p<0.05, **p<0.01, ***p<0.001