Deep bite is a common malocclusion, frequently encountered in orthodontic practice. Aetiology of deep bite is multifactorial and based on the aetiology it can either be skeletal or dental. Factors like variations in skeletal growth of jaw bases in vertical and sagittal direction, alterations in lip postures and muscle tonicity, an altered tongue function and dento-alveolar growth can result in an increased overbite [1-4]. Iatrogenic deep bite is also produced when proclined anteriors are uprighted orthodontically. This attempt to correct labial inclination of incisors is biomechanically challenging as frequently during uprightening, crown lengthens vertically resulting and further deepening of the bite [5,6].
Various mechanics can be used to correct dental deep bite which involves extrusion of posteriors, intrusion of anteriors or a combination of both [7-9]. Extrusion of posteriors is stable usually in growing individuals where muscular and soft tissue adaptation successfully happens over a time. In nongrowing individuals, the extrusion tends to relapse owing to adaptability odds of facial muscles, soft tissues and newly adjusted occlusion [10]. Intrusion of anteriors is a preferable option when deep bite is a resultant of overerupted anteriors [11].
Conventional methods of intrusion include loop mechanics like K-SIR, utility arches, three-piece intrusion arches, and reverse curve of spee arch wires [12]. But all these auxiliaries/arch wires can produce undesirable effects in the anchor segment and can thereby affect the overall treatment outcome. The introduction of temporary anchorage devices has made many different and complicated orthodontics easy and predictable to perform. They have increased the number of treatment options and has contributed in attaining better results [13,14]. Kalra’s simultaneous intrusion and retraction loop is based on frictionless mechanics and can be used for retracting and simultaneously intruding anterior teeth. K-SIR was very commonly used before the advent of TADs and still used by many orthodontists [15,16].
This aim of the present study was to compare the rate of intrusion of maxillary anteriors between skeletal anchorage devices and K-SIR loop. The null hypothesis stated no statistically significant differences in the rate of intrusion between mini implant anchorage and K-SIR loop.
Materials and Methods
This was a prospective cohort study done at the Department of Orthodontics, Saveetha Dental College, Chennai. The study was conducted between June 2019 to February 2020. It was approved by the scientific review board of Saveetha Dental College and the number provided was SRB/SDC/MDS/003/004.
Inclusion criteria: (i) Patients having Angle’s Class I or Class II Division 1 malocclusion in age group of 16-30 years with full set of permanent dentition undergoing orthodontic treatment; (ii) Overbite and overjet of >4 mm (patients who were willing for orthodontics only were recruited for this study); (iii) excessive gingival display of more than 3 mm during smile (gummy smile) requiring intrusion of upper anterior teeth; (iv) Lower lip covering more than 4 mm of maxillary central incisors.
Exclusion criteria: (i) Any craniofacial disorders including cleft lip and palate; (ii) Local/systemic problems or trauma which affects the growth and development of facial structures or body; (iii) Skeletal Deep Bite, which required surgical intervention; (iv) Periodontally compromised and flared anteriors; (v) Patients with history of previous orthodontic treatment.
At a significance level of 0.05 and power of 95%, a sample size of six subjects per group was calculated based on a previous study [17]. A total of 12 patients were selected who fulfilled the inclusion criteria. The patients were randomly allocated in two groups of six each but no specific randomisation technique was followed. There were no drop-outs in both the groups. None of the participants reported with any discomfort or implant failure. Once initial levelling and aligning was completed, intrusion and retraction was planned simultaneously. Group A was treated using TAD, while Group B was treated with K-SIR loop.
All patients were treated using 0.022 MBT Pre-adjusted Edgewise Appliance (3M, UNITEK). After the initial alignment phase which lasted 3 to 6 months depending on the malocclusion, the anterior segment consisting of maxillary incisors and canine and posterior segment consisting of maxillary first molar, second premolar were consolidated with 0.010 inch stainless steel ligature, then intrusion and retraction was started. Patients were recalled after a four week/monthly interval for review check-up as it is the routinely followed interval for reviewing patients undergoing treatment with fixed appliances.
Group A
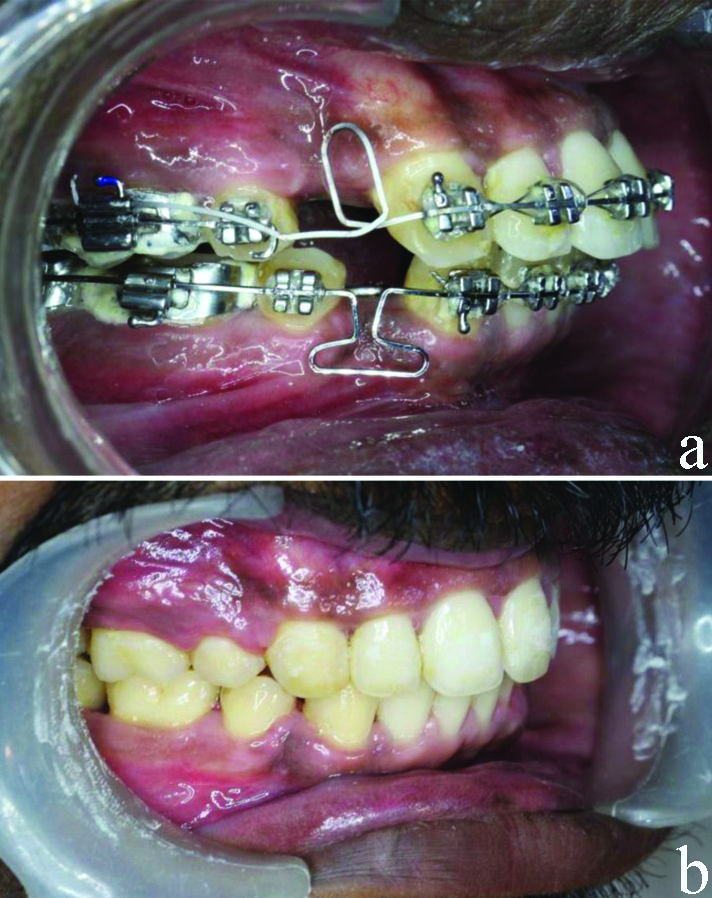
In Group A cases, for intrusion, two self-drilling microimplants (SK Surgical) diameter 1.3 mm and length 8 mm were placed between maxillary lateral incisors and central incisors bilaterally. A customised surgical guide was made with 0.016 “round Australian wire (AJ WILCOCK) to mark the exact position of placement of the implant clinically and on a radiograph. Selection of the site for microimplant was done so that it should not interfere with the intrusion and retraction process. Radioviscography (RVG) (CareStream Kodak) was taken post-insertion of microimplants to reconfirm the position and proximity to roots of incisors. In the anterior segment, the short e-chain (3M, UNITEK) was connected from wire to the implants for intrusion with a force of about 30 gms on each e-chain. The e-chain was changed every six weeks. Mini implants were loaded immediately after placement and both intrusion and retraction was started on 19×25 SS wire with retraction hooks between lateral incisor and canine. Retraction force was given using a Ni-Ti coil spring (12 mm, G&H) engaged from the molar hook to the soldered hooks on the archwire between the lateral and the canines. The Ni-Ti coil springs were later changed to 9 mm as the teeth retracted. A soldered transpalatal arch made with 19 guage SS wire was placed in all patients for anchorage control. A 30-40 gm of intrusive force per side was applied on the anterior teeth and the force was calibrated using Dontrix gauge (D-tech, India) [Table/Fig-1] [9].
(a) Beginning of Intrusion and retraction with two mini implants placed bilaterally in maxillary anterior segment for intrusion; (b) Post-treatment.

Group B
In Group B cases, intrusion and retraction was achieved using a K-SIR loop fabricated with 19×25 TMA wire (Ormco) with closed 7 mm*2 mm loop at extraction site-off centered near to the canine. Trans-palatal arch was used for anchorage control. The K-SIR loop was activated 4 mm by closing the loop and cinching it behind the first permanent molar for intrusion and retraction every three months once [Table/Fig-2] [18].
(a) K-SIR loop given in maxillary arch for simultaneous intrusion and retraction; (b) Post-treatment.
Digital lateral cephalograms were taken at following two time intervals:
(i) End of levelling and alignment (T1).
(ii) At the end of 6 months into intrusion and retraction (T2).
All lateral cephalograms were taken with the same radiography unit (PLANMECA PROMAX). The PLANMECA PROMAX is based on a unique digital technology called SCARA (Selectively Compliant Articulated Robot Arm) technology. The lateral cephalograms were recorded with the patient in the natural head position which was ascertained by the cephalostat.
Pre- and post-intrusion cephalograms were analysed using FACAD software (Version 3.11) for the assessment of upper incisor and maxillary molar positions. Two linear and one angular parameter were measured and recorded to assess the intrusion effects of incisors.
The linear parameters assessed were: (i) Vertical position of the maxillary incisors (C-PP)-Perpendicular distance from incisor centroid point to the palatal plane in mm; (ii) Vertical position of the maxillary first molar (U6-PP): Perpendicular distance from the mesiobuccal cusp tip of the molar (U6) to the palatal plane in mm.
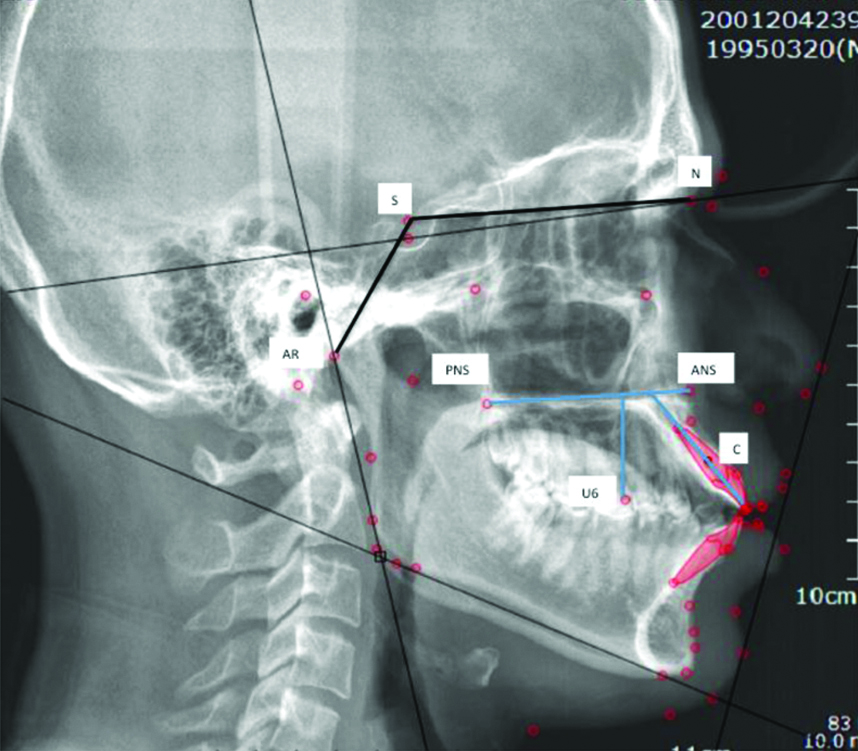
The angular parameter assessed were: (i) Change in the inclination of the maxillary incisors (U1-PP): Angle between the long axis of the maxillary incisor and the Sella Nasion (SN) plane in degrees [Table/Fig-3]. Rate of intrusion of incisors is obtained by dividing the mean amount of intrusion in mm (with mean treatment time, i.e., nearly six months in all the cases). All the measurements were made by the first author (PV) and after a week the second author (RKJ) repeated the same.
Landmarks used for analysis of cephalometric parameters: Linear parameters: (i) C-PP: Perpendicular distance from incisor centroid point to the palatal plane in mm. (ii) U6-P: Perpendicular distance from the mesiobuccal cusp tip of the molar (U6) to the palatal plane in mm.
Angular parameter: (i) U1-PP angle: Angle between the long axis of the maxillary incisor and the Sella Nasion (SN) plane in degrees
ANS: Anterior nasal spine; Ar: Articulare; C: Centroid point; N: Nasion; PNS: Posterior nasal spine; S: Sella turcica; U6- Mesiobuccal cusp tip of first permanent maxillary molar
Rate of Intrusion=Mean Intrusion/Mean Treatment Time for Intrusion. Mean Intrusion=C-PP (T1) - C-PP(T2) [17].
Statistical Analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS), Version 23; Chicago, USA). Independent t-test was used for intergroup comparison. Intragroup comparisons were performed by using paired t-tests. The p-value ≤0.05 considered to be statistically significant. Cohen’s Kappa Statistic test was used to evaluate the Inter-examiner reliability. The value for kappa was 0.613 indicating significant agreement between the two examiners.
Results
A statistically significant difference in rate on intrusion between the two groups was found. Rate of Intrusion was higher in Group A (TAD Group). The mean age of the patients included in the study was 29.5±2.1 years.
Rate of Intrusion of Maxillary Incisors
Intra-group comparison:
In Group A (TAD): A significant difference in C-PPT1 and C-PPT2 was found. C-PPT2 was significantly less than C-PPT1 (p=0.001; p<0.05).
In Group B (K-SIR): A significant difference in C-PPT1 and C-PPT2 was found. C-PPT2 was significantly less than C-PPT1 (p=0.001; p<0.05).
Intergroup comparison:
C-PPT1: No statistically significant difference was found between Group A and Group B. (p=0.103, p>0.05).
C-PPT2: No statistically significant difference was found between Group A and Group B. (p=0.11, p>0.05).
Amount and rate of intrusion: The mean amount of intrusion of incisors was calculated by difference in values of C-PPT1 and C-PPT2. Rate of intrusion was calculated by dividing the mean amount of intrusion by the total time required for intrusion i.e., six months.
For Group A (TAD group), the mean amount of intrusion was 2.3 mm, and the rate of intrusion was 0.38 mm/month. Group B (K-SIR Loop) had mean intrusion of 1.9 mm and the rate of intrusion was 0.31 mm/month. The amount and rate of intrusion was significantly higher in Group A [TAD (p=0.001, p<0.05] [Table/Fig-4].
Inter and Intragroup comparison for centroid Point-Perpendicular (PP) distance and rate of Intrusion in between the two groups.
| C-PP distance (in mm) | Group A (n=6) (Mean±SD) | Group B (n=6) (Mean±SD) | InterGroup comparison (p-value, independent t-test) |
|---|
| T1 (Pre-Intrusion) | 25.25±1.8 | 23.75±0.97 | 0.103 (NS) |
| T2 (Post-Intrusion) | 22.9±1.9 | 21.78±0.98 | 0.11 (NS) |
| Amount of intrusion (T1-T2) | 2.3±0.53 | 1.9±0.57 | 0.001 (S) |
| Rate of intrusion | 0.38 mm/month | 0.31 mm/month | 0.001 (S) |
| Intra-Group significance (p-value, paired t-test) | 0.001 (S) | 0.001 (S) | |
*S: Statistically significant
*NS: Not significant
Assessment of Maxillary First Molar Position
Intra-group Comparison:
In Group A (TAD): U6-PPT2 was significantly higher than U6-PPT1 (p=0.01; p<0.05).
In Group B (K-SIR): U6-PPT2 was significantly higher than U6-PPT1 (p=0.01; p<0.05).
Intergroup Comparison:
U6-PPT1- No significant difference was found between Group A and Group B at T1. (p=0.76, p>0.05).
U6-PPT2- No significant difference was found between Group A and Group B at T2. (p=0.61, p>0.05).
Amount of Molar Extrusion (U6-PPT2-U6-PPT1): Significantly higher amount extrusion of molar was seen in Group B (0.53 mm) as compared to Group A (0.43 mm). (p=0.001; p<0.05) [Table/Fig-5].
Inter and Intragroup comparisons for U6-PP distance and amount of molar extrusion within and between the two groups.
| U6-PP distance (in mm) | Group A (n=6) (Mean±SD) | Group B (n=6) (Mean±SD) | Intergroup Comparison (p-value, independent t-test) |
|---|
| T1 (Pre-Intrusion) | 23.98±1.6 | 22.8±0.97 | 0.76 (NS) |
| T2 (Post-Intrusion) | 24.43±1.8 | 23.33±0.98 | 0.61 (NS) |
| Amount of Extrusion (T2-T1) | 0.43±0.08 | 0.53±0.02 | 0.001 (S) |
| Intragroup significance (p-value, paired t-test) | 0.01 (S) | 0.01 (S) | |
*S: Statistically significant
*NS: Not significant
Assessment of Maxillary Incisor Inclination
Intra-group Comparison:
In Group A (TAD): A significant difference in U1-PPT1 and U1-PPT2 was found. Incisor angulation significantly decreased at T2 (p=0.05; p<0.05).
In Group B (K-SIR): No significant difference in U1-PPT1 and U1-PPT2 was found. (p=0.58; p>0.05).
Intra-group Comparison:
U1-PPT1: No significant difference was found between Group A and Group B at T1. (p=0.396, p>0.05).
U1-PPT2: No significant difference was found between Group A and Group B at T2. (p=0.4, p>0.05).
Amount of change in Incisor Angulation (U1-PPT1-U1-PPT2): Significantly higher amount change in incisor inclination was seen in Group A (reduction by 24.3 degrees from T1 to T2) as compared to Group B (reduction by 17.5 degrees from T1 to T2) (p=0.001; p<0.05) [Table/Fig-6].
Inter and Intra-group comparisons for U1-PP angulation within and between the two groups.
| U1-PP angulation (in degrees) | Group A (n=6) (Mean±SD) | Group B (n=6) (Mean±SD) | Intergroup comparison (p-value, independent t-test) |
|---|
| T1 (Pre-Intrusion) | 123.5±6.75 | 118.5±10.4 | 0.396 (NS) |
| T2 (Post-Intrusion) | 99.2±2.12 | 101±3.54 | 0.4 (NS) |
| Amount of change (T1-T2) | 24.3±8.4 | 17.5±7.5 | 0.001 (S) |
| Intra-Group significance (p-value, paired t-test) | 0.05 (S) | 0.58 (NS) | |
*S: Statistically significant
*NS: Not significant
Discussion
In deep bite cases, or in individuals with gummy smiles, intrusion of maxillary incisors is an integral part of the treatment [19-21]. In this prospective study, the aim was to compare the rate of intrusion and effects on the maxillary anteriors between K-SIR loop and TAD anchorage. In both groups simultaneously intrusion and retraction was done. Previously studies have been done to compare two intrusion systems, in which no retraction force was given while intrusive forces were given [22-24]. However, this tends to increase the total treatment time. This study assessed two systems where both intrusive and retractive forces were introduced together and rate of intrusion within such a force system was determined between two groups. Intrusive forces must be light and constant with low-load deflection mechanics [20]. The K-SIR loop was fabricated from TMA alloy to provide light, continuous force distribution. K-SIR loop remains active over a period of time with constant force. In the implant group, similar amounts of light intrusive forces were given with e-chain. Vertical control was maintained using the transpalatal arch. In the present study patients were evaluated for a period of six months after starting intrusion and retraction and not until complete retraction was done.
The results of the present study show a statistically higher rate of intrusion in the TAD group. Both the groups had a decreased Centroid- Perpendicular value post-intrusion (p-value=0.001). However, the post-intrusion values of distance between Centroid- Perpendicular was decreased significantly more in the TAD group suggesting more intrusion in that group.
The distance between the incisal edge to palatal plane is not constant when a proclined incisor is retracted thus incisal edge cannot be taken as a reliable reference point to measure true intrusion. The incisor centroid point, defined as a point on the longitudinal axis of the tooth that remains constant irrespective of change of inclination of the tooth. Therefore, the centroid point was taken as a reference point. It is the midpoint between the incisal edge and apex of the maxillary incisor [25].
In a previous study, similar results with mini implants compared to a connecticut intrusion arch were obtained. They reported a significantly higher rate of intrusion with mini implants [17]. However, in the study by Senisik NE and Türkkahraman H a similar amount of intrusion was obtained by CIA and mini implant [26] which is not in consensus with the present study. There is no reported literature comparing intrusive effects of K-SIR loop and mini implants. However, previous studies report promising results for mini implant aided intrusion [27,28]. Extrusion of first molars occurred significantly in both the groups in the present study and there was a significant difference in the amount of molar extrusion between the two groups. The molar extrusion was higher in Group B (K-SIR loop), this is because the K-SIR loop produces a clockwise moment on the molars resulting in extrusion and distalisation. Contrasting results were reported in a similar study where they demonstrated conservation of vertical anchorage of molars with mini implants [29]. Protrusion of the maxillary incisors might be an undesirable side effect of maxillary incisor intrusion. In the present study, however there was a decrease in proclination of incisors in both the groups significantly as intrusion and retraction were carried out together. The proclination was reduced significantly more in TAD group (Group A). This is in line with results by Deguchi T et al., and Upadhyay M et al., who achieved retrusion of the maxillary incisors during maxillary incisor intrusion [30,31]. A study by Jain RK reported a significantly higher amount of intrusion with mini implants without any undesirable effects [32]. Conversely, protrusion of the incisors during intrusion has been reported with intrusion arches as well as mini implants. This is due to the fact that only intrusive forces were applied in these studies [22,25].
Molar extrusion, molar rotation are one of the most important drawbacks of K-SIR arch and when used in a vertical or an average growth pattern. Anchorage control is very critical with K-SIR loop, and Mini implants are associated with mobility and failures. Hence, other methods of simultaneous intrusion and retraction can be used like sliding mechanics with reverse curve wires, three piece intrusion and retraction arch. Placement of high Trans Palatal Arch (TPA) or use of mini implants to augment anchorage control in patients with vertical growth patterns should be considered. Present study also reports significantly higher extrusion of molars with the K-SIR loop (Group B) than with mini implants.
Limitation(s)
Limitations of the study are a small sample size, short-term assessment, root resorption occurred if any was not assessed and randomisation of study samples was not done. Further studies are needed to affirm the finding of the current study as this is the first literature to report and compare the intrusive effects of K-SIR loop with implant aided intrusion and retraction.
Conclusion(s)
It can be concluded that both the modalities intruded maxillary anterior teeth but TADs were better than K-SIR in terms of: rate of intrusion, amount of intrusion and reduction of labial inclination. However, molar extrusion was more with the K-SIR loop than with TADs.