Comparison of LJ Medium and BACTEC MGIT 960 Culture System for the Diagnosis of Tuberculosis
Pinki Kumari1, Jiwesh Kumar Thakur2, Prashant Kumar3, Rakesh Kumar4, Deval Parekh5
1 Assistant Professor, Department of Microbiology, IQ City Medical College and Multispecialty Hospital, Durgapur, West Bengal, India.
2 Associate Professor, Department of General Surgery, IQ City Medical College and Multispecialty Hospital, Durgapur, West Bengal, India.
3 Assistant Professor, Department of Respiratory Medicine, IQ City Medical College and Multispecialty Hospital, Durgapur, West Bengal, India.
4 Associate Professor, Department of Community Medicine, IQ City Medical College and Multispecialty Hospital, Durgapur, West Bengal, India.
5 Specialist Pathologist, Department of Pathology, Central Hospital, Kalla, Eastern Coalfield Limited, Asansol, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rakesh Kumar, Flat-F, 2nd Floor, MC 6, IQ City, Durgapur-713206, West Bengal, India.
E-mail: dr.rakeshkr082@gmail.com
Introduction
Sputum negative pulmonary Tuberculosis (TB) is a major public health problem. So, the emergence of new techniques for a more precise and rapid microbiological identification of Mycobacterium tuberculosis in clinical samples is of great importance to improve the management of TB.
Aim
To determine and compare the sensitivity and turnaround time for Mycobacterium tuberculosis detection by the BACTEC Mycobacteria Growth Indicator Tube (MGIT) 960 system, Lowenstein Jensen (LJ) medium and Ziehl-Neelsen (ZN) staining.
Materials and Methods
An Institution based, observational, cross-sectional study was conducted at Rajendra Institute of Medical Sciences (RIMS), Ranchi, Jharkhand, India, from July 2013-March 2016. Sputum, pericardial fluid, pleural fluid, peritoneal fluid, pus and endometrial tissue samples were collected from 80 patients of suspected TB cases. All were Acid-Fast stained by ZN staining method and cultured on solid culture LJ medium and on liquid medium (MGIT). Data was analysed using Statistical Package for the Social Sciences (SPSS) software, Version 20.0 (SPSS Inc, Chicago, IL, USA). Fisher’s-Exact test was used to show association of categorical variables. Non-parametric Mann-Whitney U test was used to show median difference of non-normally distributed continuous variables of two groups.
Results
Out of the 80 samples, 41 cases were positive by either of the all methods. The positive specimen for ZN staining, LJ media and MGIT were 21, 29 and 41 cases respectively. The mean Time To Detection (TTD) was shorter for MGIT system than LJ media. Both LJ medium and MGIT 960 detected all cases of sputum smear positive cases and in addition significantly higher number than ZN stain in sputum smear negative cases. MGIT 960 detected significantly higher number of cases of sputum negative cases than LJ Media. The mean TTD was also significantly shorter in case of smear positive cases than the smear negative cases by both the solid and liquid culture mediums.
Conclusion
The use of liquid media (MGIT) is more accurate and rapid method for the diagnosis of TB. The combination of more than one method is also highly recommended for rapid detection and early treatment of TB.
Extra pulmonary tuberculosis, Lowenstein-jensen medium, Mycobacteria growth indicator tube system, Pulmonary tuberculosis
Introduction
History of Tuberculosis dates back to 4000 years [1]. Since ancient times this disease is affecting mankind in different forms. TB is caused by Mycobacterium tuberculosis which most often affects the lungs. TB is curable and preventable [2]. TB is a global disease and in 2018, South-East Asian region reported 44% of the total new cases, largest in the world [2]. In 2018, 30 high burden countries reported 85% of the total new cases and out of these 2/3rd of total new cases were reported by eight countries which include China, Philippines, Indonesia, Nigeria, South Africa, Bangladesh, Pakistan and India [2]. People having Human Immunodeficiency Virus (HIV) infection are 15-22 times more likely to develop active TB. HIV and TB co-infection is a lethal combination because each infection fastens the progress of other’s infection [2]. TB cases who don’t respond to isoniazid and rifampicin are classified as Multidrug Resistant TB (MDR-TB), which poses additional health security threat and remains a public health crisis [2]. While smear microscopy is by far the most popular method to detect mycobacteria in clinical specimen, culture of the aetiological agent remains the accepted “gold standard” for diagnosing mycobacterial infections [3]. However, cultivation on solid media, such as that of LJ, is time-consuming, taking up to 6 to 8 weeks, and has a low sensitivity especially in the samples containing small number of organisms [4,5]. In recent times, non-radiometric liquid culture media such as that used in the MGIT system have been introduced and extensively evaluated [6]. MGIT 960 system is a non-invasive instrument which is fully automated, high capacity and non-radiometric. It is used to incubate and monitor 7 mL culture tubes [7]. The MGIT uses modified middlebook 7H9 media. The culture tubes also contain silicon embedded fluorescent growth indicator present at the bottom of each tubes [8]. This compound is quenched by the presence of dissolved oxygen in the broth. As the microorganisms grow in the media, oxygen gets exhausted which allow fluorescence to be detected automatically over time [8].
MGIT 960 system is an excellent diagnostic method for the TB and many researchers have published on this topic [3-6]. However, the research which compares between the conventional and MGIT 960 media are very limited in eastern part of the country especially in resource poor state like Jharkhand. This study was planned with an objective to compare the diagnostic sensitivity of ZN Stain, LJ culture medium and MGIT 960 culture medium at a tertiary level health care facility of Jharkhand, India.
Materials and Methods
An Institution based, observational, cross-sectional study was conducted at Rajendra Institute of Medical Sciences (RIMS) Ranchi, Jharkhand, India, from July 2013-March 2016. This study was ethically cleared by Institutional Ethics Committee (IEC) of RIMS (Memo No-10: IEC/IAEL/RIMS/Ranchi, Date-13.03.15). Specimens were collected after getting written informed consent from all the study participants. Non-probability, consecutive sampling method was used and all those who came during data collection period and consented to participate in study were included in study. Total 80 study participants consented and samples were collected from them.
Samples were collected from patients suspected to be suffering from TB who visited the “Department of Microbiology, RIMS” during data collection period. All the suspected cases of pulmonary TB (persistent cough for ≥2 weeks, unexplained low grade fever specially with evening rise of temperature, unexplained weight loss etc.,) as well as Extrapulmonary TB (Non-resolving lymph node swellings, pleural effusion, abdominal pain with low grade fever and weight loss, etc.,) were included in the study. All the samples were Acid-Fast stained by ZN method and cultured on solid medium (LJ) media and on liquid media (M960).
Specimen preparation and culture methods: All specimens were processed following conventional methods for mycobacterial isolation, digestion and decontamination by the N acetyl-L-cysteine-NaOH procedure [5].
Briefly, equal volume of the freshly prepared MycoPrep NALC-NaOH solution was added to the sputum specimen, mixed on vortex and left to stand at room temperature for 15 minutes. The mixture was completed to double its volume with sterile phosphate buffer (pH 6.8) and centrifuged at 3000 x g for 15 minute. The supernatant was separated and the sediment was used for Acid-Fast Bacilli (AFB) microscopy (ZN stain) and for cultures {(one solid medium (LJ) and one liquid medium MGIT (BACTEC MGIT 960, Becton Dickinson)}.
1) MGIT 960: MGIT consists of liquid broth medium which gives better and faster growth of mycobacteria. It contains 7 mL of modified Middlebrook 7H9 broth base. A growth supplement MGIT OADC (Oleic acid, Albumin, Dextrose and Catalase) which is essential for the growth of many mycobacteria is added to make the medium complete. The medium is sterilised by autoclaving. MGIT PANTA (Polymyxin B, Amphotericin B, Nalidixic acid, Trimethoprim, and Azlocillin) is added to suppress contamination [8]. Each tube is inoculated with 0.5 mL of the processed specimen and then the tubes were kept into the MGIT 960 instrument at 37°C and were monitored automatically after every one hour for increase in fluorescence for a maximum of six weeks. Any sample, which showed signal of growth, is taken out from the instrument. From the positive tube, a smear preparation is done for microscopic examination of AFB. A blood agar plate inoculated for sub-culture on LJ slant to detect any contamination for the BACTEC MGIT 960 culture media. No growth was observed in blood agar plate.
2) Solid media: For inoculation onto solid LJ slant, 0.1 mL of the suspension was used. Solid media was incubated at 37°C in a slant position for 24-48 hours, then in upright position for a further eight weeks and read daily for the 1st week then twice weekly. Colonies of Mycobacterium tuberculosis is identified by its rough, crumbly, waxy, buff colored appearance which develops after 2-3 weeks after inoculation. The colony with doubtful morphology was confirmed by ZN staining [9]. All positive, liquid and solid media are sub-cultured onto Columbia agar with 5% sheep blood to check for contaminants [5]. No growth was observed onto Columbia agar with 5% sheep blood in present study.
Statistical Analysis
All the data were codified and entered in MS Excel spread sheet. Data were analysed using SPSS software, Version 20.0 (SPSS Inc, Chicago, IL, USA). Fisher’s-Exact test was used to show association of categorical variables. Non-parametric Mann-Whitney U test was used to show median difference of non-normally distributed continuous variables of two groups. The p-value ≤0.05 was considered as statistically significant.
Results
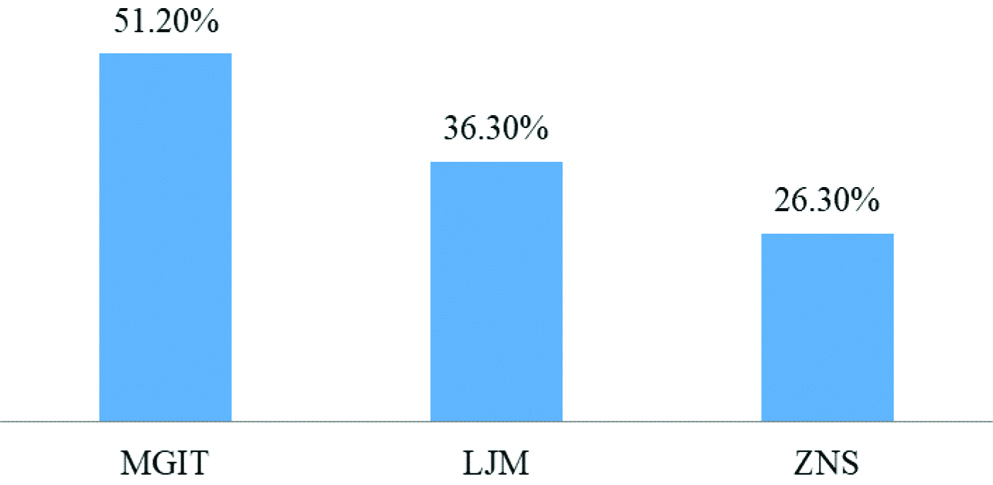
Mean age of the study population was 51.63±12.9 years. A 47.5% of study population belonged to age group of 41-60 years followed by 30.0% and 22.5% who belonged to age group of ≥61 years and 20-40 years, respectively. Total 80 samples were processed using ZN stain, LJ medium culture and MGIT 960 culture medium. An 80.0% of sample was sputum followed by pus (7.5%), peritoneal fluid (5.0%), pleural fluid (3.75%) and lymph node aspirates (3.75%). Two of the study population was HIV positive [Table/Fig-1]. The isolates were identified as Mycobacterium tuberculosis on the solid culture media by the rate of growth, pigment production and further Acid-Fast staining and from the M960 tubes by confirmation by the BD MGIT 960TbC ID test strips. Out of the 80 samples under study, total 41 samples (51.2%) were found to be positive by any of the three methods viz., ZN Stain, LJ Media or MGIT 960. All 41 were detected by MGIT 960 method followed by 29 and 21 by LJ media and ZN staining, respectively [Table/Fig-2]. Out of the 59 smear negative cases, culture on LJ media detected eight cases [Table/Fig-3] while M960 system detected 20 cases. All 21 sputum positive cases on ZN stain [Table/Fig-4] were detected by both LJ media as well as by MGIT 960 media [Table/Fig-5].
Clinico-social characteristics of study population, n=80.
| Clinico-social characteristics | n (%) |
|---|
| Age group (years) |
| 20-40 | 18 (22.5) |
| 41-60 | 38 (47.5) |
| ≥61 | 24 (30.0) |
| Gender |
| Male | 55 (68.8) |
| Female | 25 (31.2) |
| Types of sample |
| Sputum | 64 (80.0) |
| Pus | 6 (7.5) |
| Peritoneal fluid | 4 (5.0) |
| Pleural fluid | 3 (3.75) |
| Lymph node aspirate | 3 (3.75) |
| HIV status |
| HIV Negative | 78 (97.5) |
| HIV Positive | 2 (2.5) |
Simple bar diagram showing percentage of samples tested positive by different media, n=80.
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium; ZNS: Ziehl neelsen stain
Colonies of Mycobacterium tuberculosis (arrow) on L-J medium.

ZN staining of mesenteric lymph node aspirate from HIV positive patient showing Acid-Fast Bacilli (arrow).

Distribution of test results as per the different diagnostic test results (n=80).
| Diagnostic test | Total positive | Total negative | Sputum positive diagnosed by LJ media | Sputum negative diagnosed by LJ media | Sputum positive diagnosed by MGIT 960 | Sputum negative diagnosed by MGIT 960 | LJ medium positive diagnosed by MGIT 960 | LJ medium negative diagnosed by MGIT 960 |
|---|
| ZN stain | 21 | 59 | | | | | | |
| LJ medium | 29 | 51 | 21 | 8 | | | | |
| MGIT 960 | 41 | 39 | | | 21 | 20 | 29 | 12 |
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium; ZNS: Ziehl neelsen stain
While the sensitivity of MGIT 960 culture was 100.0%, the sensitivity of LJ medium and ZN stain was found to be 70.7% and 51.2%, respectively [Table/Fig-6]. LJ culture medium detected eight more case than ZN stain and MGIT 960 detected 20 more cases than ZN stain. Higher detection rate of TB infection by LJ Media and MGIT 960 Media than JN stain was found to be statistically significant by Fisher’s-Exact test [Table/Fig-7]. In addition to identifying all the LJ medium positive samples, MGIT 960 diagnosed 12 more cases which were found to be negative by LJ Medium. Higher detection rate of MGIT 960 than LJ medium was also found to be statistically significant [Table/Fig-8].
Sensitivity of ZN stain and LJ media in detecting Mycobacterium tuberculosis as compared to “Gold standard” MGIT 960 media (n=80).
| Test | n | True Positive (TP) | False Negative (FN) | True Negative | Sensitivity (TP/TP+FN) |
|---|
| ZN stain | 80 | 21 | 20 | 39 | 21/41×100=51.2% |
| LJ media | 80 | 29 | 12 | 39 | 29/41×100=70.7% |
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium; ZNS: Ziehl neelsen stain; TP: True positive; FN: False negative
Fisher’s-Exact test showing association between sputum positivity and different culture media (n=80).
| Culture media | Sputum | Total n (%) | p-value |
|---|
| Positive (%) | Negative (%) |
|---|
| LJ Media |
| Positive | 21 (72.4) | 8 (27.6) | 29 (100.0) | |
| Negative | 0 | 51 (100.0) | 51 (100.0) | <0.05 |
| MGIT 960 |
| Positive | 21 (51.2) | 20 (48.8) | 41 (100.0) | |
| Negative | 0 | 39 (100.0) | 39 (100.0) | <0.05 |
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium
Fisher’s-Exact test showing association between LJ media and MGIT 960 (n=80).
| Culture media | LJ medium | Total n (%) | p-value |
|---|
| Positive (%) | Negative (%) |
|---|
| MGIT 960 |
| Positive | 29 (70.7) | 12 (29.3) | 41 (100.0) | |
| Negative | 0 | 39 (100.0) | 39 (100.0) | <0.05 |
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium
The median TTD was 9.0 days {Inter Quartile Range (IQR)}: (8.0-10.0) and 33.0 days (IQR: 28.0-34.0) in MGIT 960 media and LJ media, respectively. Mean Rank of LJ Media was 14.79 and 49.65 in case of sputum smear positive and sputum smear negative samples, respectively. Similarly, mean rank of MGIT 960 was 25.17 and 45.96 in case of sputum smear positive and sputum smear negative samples respectively. Low mean rank in case of sputum smear positive cases as compared to sputum smear negative cases was statistically significant in both LJ media culture and MGIT 960 culture method [Table/Fig-9].
Mann-Whitney U test showing median Time To Detection (TTD) and mean rank of different culture media in sputum smear positive and negative samples (n=80).
| Test | Sputum smear | Number | Mean rank | Median (IQR) days | Mann-Whitney U | p-value |
|---|
| LJ media | Positive | 21 | 14.79 | | | |
| Negative | 59 | 49.65 | 33.0 (28.0-34.0) | 79.5 | <0.05 |
| MGIT 960 | Positive | 21 | 25.17 | | | |
| Negative | 59 | 45.96 | 9.0 (8.0-10.0) | 297.5 | <0.05 |
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium
Discussion
The present study demonstrated that M960 system provided better isolation rates of Mycobacterium tuberculosis (100%) from the clinical samples than the LJ media (70.7%) or the simple acid fast staining by the ZN Method (51.2%). Results of this study are in agreement with few other studies which also reported that the BACTEC MGIT 960 had higher recovery rate for Mycobacterium tuberculosis than solid media [7,10-13]. Bunger R et al., reported 91.6% recovery of Mycobacterium tuberculosis by MGIT 960 system as compared to only 58.3% by LJ medium [14]. However, a study by Siddiqui MAM et al., reported a low detection rate of 15.0% for both LJ Media and MGIT 960. This might be due to either improper sample collection or higher contamination rate [15]. In this study, all the ZN stained smear which were positive by direct microscopy were also positive by the growth on LJ media, and also out of the total positive cases of TB (41 cases), the LJ media showed growth in 28 cases implying the isolation rate or the sensitivity of LJ media to be 70.7%. An almost similar detection rate of Mycobacterium tuberculosis by LJ medium was reported by Almazini MAI et al., (72.6%) and Aziz NA et al., (76.1%) [16,17]. A bit higher detection rate of 81.8% by LJ medium was reported by Somoskovi A et al., [18]. The isolation rate was also higher in smear positive samples than the smear negative samples. These slight variations in the sensitivity of LJ medium to detect TB may be due to the method and quality of sample collection or due to the difference in clinical case presentation.
In present study, the Mycobacterium tuberculosis detection rate was significantly higher (100.0%) for MGIT 960 than LJ culture media (70.7%) and ZN staining method (51.2%). Many other research articles have reported almost similar and significant higher detection rate of Mycobacterium tuberculosis by MGIT 960 than LJ culture media and ZN staining method [7,10-13]. Higher detection rate with MGIT 960 medium may be because of the less contamination rate with the MGIT 960 system [19,20]. However, there are studies who reported a lower detection rate of Mycobacterium tuberculosis by MGIT 960 [21-23]. Somoskovi A et al., reported a detection rate of 96.4% by MGIT 960 [18]. Few other studies reported a detection rate of 75.3%-95.1% for MGIT 960 culture medium [22-23].
In this study, the median TTD was 9.0 days and 33.0 days in MGIT 960 media and LJ media respectively. Mean rank of both LJ media culture and MGIT 960 culture method were significantly lower in sputum smear positive cases. The median TTD by both LJ media and MGIT 960 media was significantly lower in sputum smear positive samples. In present study, median TTD was 9 days for MGIT 960 culture media which was shorter than Tortoli E et al., (19.6 days) Somoskovi A et al., (15.8 days) [10,18]. Lower median TTD in present study might be due to less contamination, precise sample collection and inclusion of more clinically relevant cases. Lower mean TTD for sputum smear positive samples than smear negative samples were also reported by Almazini MAI et al., Aziz NA et al., Somoskovi A et al., and Piersimoni C et al., [16-18,24]. MGIT 960 culture medium is a rapid and more sensitive diagnostic test for Mycobacterium tuberculosis than the traditional ZN stain and LJ culture medium.
Limitation(s)
Limitation of the study includes non-probability sampling technique and failure to compare the MGIT 960 with other liquid culture medium like BACTEC12B.
Conclusion(s)
The use of liquid media (MGIT-960) is more accurate and rapid method for the diagnosis of TB than the conventional solid culture method using LJ media. This early and appropriate diagnosis of TB can aid in the usage of appropriate drugs and prevent the emergence of MDR-TB and hence reduce the overall morbidity and mortality due to the disease.
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium; ZNS: Ziehl neelsen stain
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium; ZNS: Ziehl neelsen stain; TP: True positive; FN: False negative
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium
MGIT: Mycobacterial growth indicator tube; LJM: Löwenstein jensen medium
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 23, 2020
Manual Googling: Nov 03, 2020
iThenticate Software: Nov 21, 2020 (18%)
[1]. Zaman K, Tuberculosis: A global health problemJ Health Popul Nutr 2010 28(2):111-13.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2980871/pdf/jhpn0028-0111.pdf (last accessed on 10th October 2020)10.3329/jhpn.v28i2.487920411672 [Google Scholar] [CrossRef] [PubMed]
[2]. World Health Organization (WHO). WHO Information Fact Sheets/Tuberculosis/2020. Available at https://www.who.int/news-room/fact-sheets/detail/tuberculosis (Last accessed on July 2020) [Google Scholar]
[3]. Cheng VCC, Yew WW, Yuen KY, Molecular diagnostics in tuberculosisEur J Clin Microbiol Infect Dis 2005 24(11):711-20.10.1007/s10096-005-0039-116283213 [Google Scholar] [CrossRef] [PubMed]
[4]. Negi SS, Khan SF, Gupta S, Pasha ST, Khare S, Lal S, Comparison of the conventional diagnostic modalities, bactec culture and polymerase chain reaction test for diagnosis of tuberculosisIndian J Med Microbiol 2000 23(1):29-33.10.1016/S0255-0857(21)02708-0 [Google Scholar] [CrossRef]
[5]. Kent PT, Kubika GP. Public health mycobacteriology (1985): A guide for a level III laboratory. Centers for Disease Control, Atlanta, Georgia, 1985. https://ntrl.ntis.gov/NTRL/dashboard/searchResults/titleDetail/PB86216546.xhtml (Last accessed on 18th October 2020) [Google Scholar]
[6]. Salfinger M, Pfyffer GE, The new diagnostic mycobacteriology laboratoryEur J Clin Microbiol Infect Dis 1994 13(11):961-79.10.1007/BF021114987698123 [Google Scholar] [CrossRef] [PubMed]
[7]. Lu D, Heeren B, Dunne WM, Comparison of the automated Mycobacteria Growth Indicator Tube System (BACTEC960/MGIT) with Lowenstein-Jensen medium for recovery of mycobacteria from clinical specimensAm J Clin Pathol 2002 118(4):542-45.10.1309/65KN-2M7E-7MNN-X0TA12375641 [Google Scholar] [CrossRef] [PubMed]
[8]. Siddiqi SH, Gerdes SR. MGIT Procedure manual: Mycobacterial Growth Indicator Tube (MGIT) Culture and Drug Susceptibility Demonstration Project. Foundation for innovative new diagnostics, Geneva, Switzerland, 2006. https://www.finddx.org/wp-content/uploads/2016/02/mgit_manual_nov2006.pdf (last accessed on 18th October 2020) [Google Scholar]
[9]. Revised National TB Control Programme Training Manual for Mycobacterium tuberculosis Culture & Drug Susceptibility testing. Central TB division, Directorate General of Health Services, Ministry of Health and Family Welfare, New Delhi, India, 2009. https://tbcindia.gov.in/WriteReadData/l892s/6995271860Training%20manual%20M%20tuberculosis%20C%20DST.pdf (Last Accessed on 18th October 2020) [Google Scholar]
[10]. Tortoli E, Cichero P, Piersimoni C, Simonetti T, Gesu G, Nistta D, Use of BACTEC MGIT for recovery of mycobacteria from clinical specimens: Multicentric studyJ Clin Microbiol 1999 37(11):3578-82.10.1128/JCM.37.11.3578-3582.199910523555 [Google Scholar] [CrossRef] [PubMed]
[11]. Hanna BA, Ebrahimzadeh A, Elliott LB, Morgan MA, Novak SM, Rusch-Gerdes S, Multicentre evaluation of the BACTEC MGIT 960 system for recovery of mycobacteriaJ Clin Microbiol 1999 37(3):748-52.10.1128/JCM.37.3.748-752.19999986844 [Google Scholar] [CrossRef] [PubMed]
[12]. Hines N, Payeur JB, Hoffman LJ, Comparison of the recovery of Mycobacterium bovis isolates using the BACTEC 460 TB system and middle brook 7H10 and 7H11 solid mediaJ Vet Diagn Invest 2006 18(3):243-50.10.1177/10406387060180030216789711 [Google Scholar] [CrossRef] [PubMed]
[13]. Rishi S, Malhotra B, Pal N, A Comparative study for the detection of mycobacteria by BACTEC MGIT 960, Lowenstein Jensen media and direct AFB smear examinationInd J Med Microbiol 2007 25(4):383-86.10.1016/S0255-0857(21)02056-9 [Google Scholar] [CrossRef]
[14]. Bunger R, Singh VA, Avneet Mehta S, Pathania D, Evaluation of BACTEC Micro MGIT with Lowenstein Jensen media for detection of Mycobacteria in clinically suspected patients of extra pulmonary tuberculosis in a tertiary care hospital at Mullana (Ambala)J Med Microb Diagn 2013 2(3)10.4172/2161-0703.1000123 [Google Scholar] [CrossRef]
[15]. Siddiqui MAM, Anuradha PR, Nagamani K, Vishnu PH, Comparison of conventional diagnostic modalities, BACTEC culture with polymerase chain reaction for diagnosis of extra-pulmonary tuberculosisJ Med Allied Sci 2013 3(2):53-58. [Google Scholar]
[16]. Almazini MAI, Mankhi AA, Al-Kinani EAK, Study comparison of diagnostic methods for tuberculosis patients in IraqAdv Biores 2015 6(2):11-22.http://soeagra.com/abr/abrmarch2015/3.pdf (Last accessed on 22th October 2020) [Google Scholar]
[17]. Aziz NA, Ahmed H, Morsy MM, Sabet EA, Comparative evaluation of the BACTEC MGIT 960 (Mycobacteria Growth Indicator Tube) system with LJ solid medium for diagnosis of pulmonary tuberculosisEgyptian Journal of Medical Microbiology 2009 18(2):113-18. [Google Scholar]
[18]. Somoskovi A, Kodmon C, Lantos A, Bartfai Z, Tam L, Fuzy J, Comparison of recoveries of mycobacterium tuberculosis using the Automated BACTEC MGIT 960 system the BACTEC 460 TB system and Lowenstien-Jensen mediumJ of Clin Microbiol 2000 38(6):2395-97.10.1128/JCM.38.6.2395-2397.200010835013 [Google Scholar] [CrossRef] [PubMed]
[19]. Pfyffer GE, Welscher HM, Kissling P, Cieslak C, Casal MJ, Gutierrez J, Comparison of the mycobacteria growth indicator tube (MGIT) with radiometric and solid culture for recovery of acid-fast bacilliJ Clin Microbial 1997 35(2):364-68.10.1128/jcm.35.2.364-368.19979003597 [Google Scholar] [CrossRef] [PubMed]
[20]. Chihota VN, Grant AD, Fielding K, Ndibongo B, Zyl AV, Muirhead D, Liquid versus solid culture for tuberculosis: Performance and cost in a resource-constrained settingInt J Tuberc Lung Dis 2010 14(8):1024-31. [Google Scholar]
[21]. Bohy E, Raafat H, Aly F, El-Aziz MA, Comparison between Mycobacteria Growth Indicator Tube (MGIT), BACTEC 460 TB system and Lowenstein-Jensen medium for detection of mycobacterium tuberculosisEgyptian Journal of Bronchology 2009 3(2):102-08. [Google Scholar]
[22]. Huang TS, Chen CH, Lee SS, Huang WK, Liu Y, Comparison of BACTEC MGIT 960 and BACTEC 460 TB system for detection of mycobacteria in clinical specimensAnnals of Clinical and Laboratory Science 2001 31(3):279-83. [Google Scholar]
[23]. Badak FZ, Kiska DL, Setterquist S, Hartly C, O’Connell MA, Hopfer RL, Comparison of mycobacteria growth indicator tube with BACTEC460 for detection and recovery of mycobacteria from clinical specimensJ of Clin Microbiol 1996 34(9):2236-39.10.1128/jcm.34.9.2236-2239.19968862591 [Google Scholar] [CrossRef] [PubMed]
[24]. Piersimoni C, Scarparo C, Cichero P, Pezzo MD, Covelli I, Gesu G, Multicenter evaluation of the MB-Redox medium compared with radiometric Bactec system, Mycobacteria Growth Indicator Tube (MGIT), and Löwenstein-Jensen medium for detection and recovery of acid-fast bacilliDiagn Microbiol Infect Dis 1999 34:293-99.10.1016/S0732-8893(99)00029-2 [Google Scholar] [CrossRef]