Full-coverage crown construction is one of the most common procedures performed by general dental practitioners [1]. Nonetheless, this procedure is very challenging due to the increased number of patients that remain dentate but require advanced rehabilitation for the current dentition including construction and fabrication of full-coverage crowns . [2]. This treatment requires fundamental preclinical and clinical training that forms an integral part of the curriculum for UG. Thus, there is a need for dentists to develop and enhance the core skills of crown preparation and fabrication during training in order to provide this treatment in dental practice [3].
UG dental students are one of the main care providers for full-coverage crowns in the university dental setting. They develop the skills for clinical procedures on crown preparation in clinical skills laboratory with the aid and guidance of clinical tutors [4,5]. The students then further develop and practice the skills learnt on patients in a clinical environment by providing a comprehensive range of full-coverage crowns for the patients under their clinical care. At this stage, UG students are expected to be able to provide the care equivalent to that of practising general dentist with the aid and guidance provided by clinical teaching staff with consistent clinical competence [4,5].
Currently, the teaching staff lacks comprehensive objective data that is able to encapsulate the ability of students to translate the operative skills learnt in a simulated environment to the patient-care clinic [6]. It would be useful to have an appreciation of the student’s ability to provide these treatments, as compared to a gold standard preparation guideline as proposed by the current prosthodontic literature and textbooks. Currently, the common practice and method adopted by dental schools is to implement criteria and grading based on core and fundamental guidelines, literature and key prosthodontics reference books [7-9].
The study was conducted as there is a paucity of data and evidence on the assessment and evaluation of tooth preparation by UG dental students in clinical training. The aim of this study was to evaluate full-coverage crown preparations performed by UG dental students in the university clinical teaching programme by assessing the working casts which contained one or more full-coverage crown preparations based on specific criteria and grading system.
Materials and Methods
A cross-sectional clinical audit was performed on the quality of full-coverage crown preparations by fifth year UG dental students of Universiti Sains Islam, Malaysia (USIM). The inclusion criteria were the final working casts prepared by the fifth year UG students in which the full-coverage crown was then fitted and issued to patients from April to July 2018 during which all the fifth year UG students would have completed the preclinical course and clinical competency assessment in full-coverage crown preparation.
Single unit crowns in working casts with all types of teeth with the exception of the third molar teeth are included in this study. The data was derived primarily by assessing the final working casts that were used for the fabrication of full-coverage crowns with the use of different materials available such as PFM, all ceramic (lithium disilicate and zirconia) and full-metal. The exclusion criteria were the final working casts with the third molar crown preparations, partial coverage crown preparations, fixed bridge prosthesis and crown preparations performed by UG students other than fifth year UG dental students.
All the impressions were recorded with heavy and light body polyvinylsiloxane (Aquasil Ultra, Dentsply Sirona, Charlotte, North Carolina, USA) and custom tray fabricated from light-cured acrylic resin (Kemdent LC Trays, Kemdent®, Swindon, Wiltshire, United Kingdom). The impressions were recorded by the students who conducted the crown preparations. The impression was sent to the laboratory, disinfected and poured in Type IV die stone. The dies were then trimmed and sectioned by the laboratory staff. The construction of each specific types of crowns were according to the laboratory production protocols. The students collected the final working casts and the crowns were fitted to the patients.
The final working casts were collected within April to July 2018 by the authors with a total 40 units of working casts consisted of 45 full-coverage crowns from 31 patients included for quality assessment in this study.
Assessment Tools
An audit proforma checklist adopted from the standard criteria of tooth preparation for full-coverage crowns was constructed for this clinical audit [7,9]. The main criteria for quality assessment of a crown preparation included occlusal reduction, buccal/labial reduction, lingual/palatal reduction, proximal reduction, cervical margins, as well as an overall assessment (smooth preparation with no sharp line angles) of the complete tooth preparation. An example of the criteria and grading assessment form for zirconia crown preparation is given in [Table/Fig-1]. Each criterion of assessment was categorically divided according to the following grades of: I) Not attained; II) Adequate; and III) Well-achieved based on the evaluated final working cast. Adequate (II) and Well-Achieved (III) criteria were considered as acceptable in this study. The adequacy of crown preparation was finally assessed according to clinical standards [Table/Fig-2].
Example of the criteria and grading assessment form for the preparation of a zirconia crown for an anterior tooth [7,9].
| Criteria | Not attained | Adequate | Well-achieved | Remarks |
|---|
| Labial/Buccal reduction planes | | | | |
| a. 2 planes reductionb. Reduction of 1.5 mm with no undercut present | | | | |
| Palatal/Lingual reduction planes | | | | |
| a. 2 planes reductionb. Reduction of 1.0 mm with no undercut present | | | | |
| Occlusal reduction | | | | |
| a. At least 1.5 mm on incisal reduction.b. Range of 1.5-2.0 mm | | | | |
| Cervical margin | | | | |
| a. Shoulder reduction 1.0 mm.b. Clear and continuous margin | | | | |
| Proximal reduction | | | | |
| a. No undercut and no excessive axial convergence (within 5° to 20°)b. Not touch/damage adjacent teeth | | | | |
| Overall assessment | | | | |
| a. Smooth with no sharp line angles | | | | |
Criteria and standards of the clinical audit [7,9].
| Criteria | Standards |
|---|
| Adequate preparation for a full-coverage crown should be demonstrated on the final working casts | Working casts is able to demonstrate an adequate preparation/finishing line for full-crown according to current prosthodontic literature and textbook |
| a) Adequate lingual/palatal reduction planes |
| b) Adequate buccal/labial reduction planes |
| c) Adequate occlusal reduction |
| d) Adequate preparation of cervical margin |
| e) Adequate proximal reduction |
| f) Adequate smooth preparation with no sharp line angles |
The assessment tools which were used as criteria for clinical guidelines for full-crown preparation were advocated by the prosthodontics teaching members during teaching and learning sessions [7,9].
Other relevant patient details including age, gender, reasons of crown fabrication and tooth vitality response to thermal and electrical tests were also taken into account for further analysis.
Data Collection
The final working casts were assessed by performing visual examination under proper illumination and magnification by dental loupes (2.5X, EyeMag Smart Loupe, Carl Zeiss) at the Preclinical Prosthodontics Simulation Laboratory, Faculty of Dentistry, USIM. The assessment was conducted with the aid of a standardised parallelometry using a mechanical Dental Surveying Unit (Bego Paraflex, Bego USA Inc., USA) to verify the tooth preparations on the working casts [Table/Fig-3]. The tooth preparation quality was assessed with careful collective considerations by examination of the final working casts by using William’s periodontal probe, diagnostic casts, silicone index fabricated prior to crown preparations, opposing and adjacent teeth, previous record on patient’s notes and instructions at the laboratory cards by the students [Table/Fig-4,5 and 6].
Assessment of working cast using mechanical dental surveying unit set at 0 degree to verify the tooth preparations on working casts.

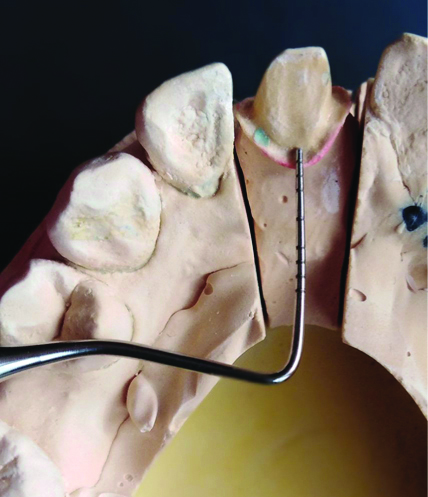
Example of the assessment of the cervical margin using William’s periodontal probe showed 1.0 mm of preparation with uniformity in cervical margin preparations.
Example of occlusal reduction measurements utilising the William’s periodontal probe and silicone putty index.

Picture of analog calliper utilisation in measuring the consistencies of crown preparations in the final working cast.

Prior to the study, an ethical approval was obtained from the University Research Ethical Committee {USIM/FPg-MEC/2016/No.(46)} in accordance with the Declaration of Helsinki. Two experienced and independent prosthodontists were enrolled for the cast assessment and the inter-examiner calibration showed a substantial agreement with a Cohen’s kappa score of 0.78 (κ=0.78).
Statistical Analysis
The data analysis was performed using Microsoft Excel 2013 with the descriptive data measured in frequency and percentage for categorical variables and mean and standard deviation for continuous data.
Results
A total of 31 patients fitted with 45 units of full-coverage crowns from 40 working casts in this audit ranged between ages of 17 to 63 with a mean age of 40.5 (SD±14.16). Majority of them were females (58.1%) and were given PFM crowns (51.1%). A great majority (84.4%) of the teeth treated with crown were nonvital [Table/Fig-7].
Demographic data and type of crowns constructed by final year Undergraduate (UG) dental students.
| Characteristics | n | Percentage (%) |
|---|
| Gender |
| Male | 13 | 41.9 |
| Female | 18 | 58.1 |
| Vitality |
| Nonvital | 38 | 84.4 |
| Vital | 7 | 15.6 |
| Type of crown material |
| PFM | 23 | 51.1 |
| Zirconia and lithium disilicate | 18 | 40.0 |
| Full-metal | 4 | 8.9 |
| Reasons for crown fabrication |
| Root Canal Treatment (RCT) | 25 | 55.5 |
| RCT with Post and Core | 13 | 28.9 |
| Others | 7 | 15.6 |
The final outcome according to the standards used in this clinical audit was as in [Table/Fig-8]. Overall, the students achieved a satisfactory standard on the compliance rate for crown preparation. They achieved the highest percentage that is 97.7% for the criterion on smooth preparation with no sharp line angles. Meanwhile, the lowest percentage of standard of 51% was for the adequacy in proximal reduction. The study also found that all working casts were 100% free of distortion and bubbles along the finishing lines, preparation lines and walls.
Results according to the standards of the study (n=45). Well-achieved and adequate criteria were included as acceptable standards in this study.
| Criteria | Standards | Not attained | Acceptable |
|---|
| Adequate | Well-achieved |
|---|
| n (%) | n (%) | n (%) |
|---|
| Adequate preparation for a full-crown should be demonstrated on the final working cast | Working casts is able to demonstrate an adequate preparation/finishing line for full-crown according to current prosthodontic literature and textbook | 13 (28.8) | 0 (0.0) | 32 (71.1) |
| Lingual/palatal reduction planes | 13 (28.8) | 28 (63.6) | 4 (8.88) |
| Buccal/labial reduction planes | 13 (28.8) | 26 (57.7) | 6 (13.3) |
| Occlusal reduction | 12 (26.6) | 29 (64.4) | 4 (8.88) |
| Preparation of cervical margin | 18 (40.0) | 23 (51.1) | 4 (8.88) |
| Proximal reduction | 22 (48.8) | 20 (44.4) | 3 (6.6) |
| Smooth preparation with no sharp line angles | 1 (2.2) | 44 (97.7) | 0 (0.0) |
Discussion
A proper and detailed preparation of the tooth prior to the fabrication of a full-coverage crown with the aim to achieve a clinically successful prosthesis should be done according to the standard prosthodontic literature and textbooks [7,9]. The crown preparation should follow the principles of tooth preparation which include adequate retention and resistance, structural durability, preservation of tooth structure, preservation of periodontium and marginal integrity [7,9]. Apart from that, satisfactory aesthetic value is another main component that needs to be considered during the fabrication of a full-coverage crown to ensure longevity of the crown, in addition to a predictable prognosis of the restoration, as well as the satisfaction quotient of the patient concerned. These combined components have been used for the prosthodontic academic programmes worldwide [10,11].
In this study, the analysis performed in the teaching institute showed that the majority of the full-coverage crown constructed by fifth year UG dental students were on nonvital teeth (84.4%) in which 28.9% (n=13) were root filled teeth and restored with post and core prior to the fabrication of the crown. There was a strong emphasis on prosthodontic pedagogy practiced in this teaching institution that the root filled teeth required cuspal coverage restoration to ensure the longevity and survival of the teeth in a long run. A study by Aquilino SA et al., showed that the root filled teeth that were not crowned after completion of obturation stage were lost at 6.0 times higher than the root filled teeth that were crowned after completion of RCT [12]. Another study by Stavropoulou AF and Koidis PT showed that the 10 years survival rate of crowned root filled teeth (81%) were higher than the root filled teeth that were restored by direct restoration (63%) [13].
The study involved an analysis on a range of final working casts of full-coverage crowns using different materials including full-metal, zirconia, lithium disilicate and PFM crown. In this study, the criteria that scored the highest were smooth preparations with no sharp line angles in 97.7% (n=44) crowns. This finding was similar to a study by El-Mubarak N et al., in which it was shown that all the full-crown preparation on the working casts were generally smooth with no sharp angles [14]. This criterion is paramount to ensure that future prosthesis are more resistant to stress during functional dynamic mastication movements [7,9]. The criterion that scored the lowest in this study was the proximal reduction whereby according to the audit proforma guidelines used, the acceptable angle of convergence ranges between 5° to 20°. It was suggested that the ideal total convergence angle was between 10° to 20° by Goodacre CJ et al., and considered acceptable in the ranged between 4° to 14° by other literature [7,9]. In the current study 23 crowns (51%) showed acceptable proximal reduction. This finding was in agreement with the other studies that showed the dental students tended to finish tooth preparations with higher convergence angle. Measurements for total convergence angle by the dental students in other studies include Al-Omari WM and Al-Wahadni AM (22.4° to 25.3°), Enechi TC (25°) and Rafeek RN et al., (31.6° for anterior teeth) are higher than the recommendation by the classic prosthodontic literature and textbook [15-17]. The higher and excessive total convergence angle might potentially reduce the retention and resistance form of the future prosthesis and the other conventional methods to increase the retention and resistance form like the construction of retention grooves were required [7,9]. The inconsistencies of the proximal reduction between students might be contributed by operator factor such as lack of clinical experience or anatomical factors such as convexity of the buccal and lingual walls of the molar teeth and prominent cingulum on anterior teeth especially on canines [14].
The preparation of a good and definite finish line is important, as it will determine the structural durability and margin integrity of the prosthesis. It is also very closely related to the periodontium maintenance and biological width preservation of the tooth, as it maintains the quality of the restoration, while prolonging the longevity of the prosthesis [9,18]. In this study, demonstration of an adequate preparation and finishing line was 71.1% (n=32) samples fulfilling the criteria. It can be challenging for the operator especially UG dental students to provide an acceptable finish lines due to minimal clinical experience, difficulty of accessing the preparation especially at the interproximal area, the possibility of the teeth being cut or stripped off accidentally and errors in visual estimation [8,14].
The challenging dilemma in the preclinical and clinical prosthodontic training was to train dental students to visualise and advocate the preparation features as demonstrated by the faculty members. It depends on the overall subjective amount of preparation without an exact objective value in quantifying the absolute numerical values required for the preparation [19]. In recent years, the current technology adopted in preclinical dental training with the extensive use of Computer Aided Technology/Manufacturing (CAD-CAM) includes the introductory usage of intraoral scanner and specialised software. This technique had been advocated in preclinical trainings and published in multiple reports from dental schools throughout the world. It will allow a more accurate and precise definition of the preparation features compared to subjective visualisation by the operators. This will indirectly improve the psychomotor of the dental students in appreciating the clinical exercise given [19-21].
There were also reports on the preclinical training done using virtual reality simulation [22,23]. This was based on the haptic feedback in which the UG dental students were trained to develop and improve the overall dental operative procedure. This training provided a natural force feedback that allowed the dental students to appreciate the simulated clinical procedure as it mimics a real clinical situation [24]. It was designed to improve the proprioception and manipulation of the sensory skills of the dental students in preclinical trainings. It also provides an entirely different format and environment compared to the conventional preclinical trainings that were based solely on clinical operative procedures. The feedback is given by the faculty members with the additional input from the virtual simulation machine data using the haptic technology [23,25]. The opinion on the implementation of the digital approach towards clinical training seemed encouraging. A study suggested that the implementation of a digital assessment software will allow the dental students to independently assessed the objective data while also being helpful for faculty members to bridge the gap between different cohort of students with multiple achievements [27].
This current study will provide current academic staff with data on student’s performance in crown preparation at the clinical stage.
Limitation(s)
There were a few limitations to this study such as the grading and the evaluation of the tooth preparation were solely based on the final working casts without proper aid or knowledge on the previous original working impressions. Besides that, poor archiving of the documents required such as final working casts and laboratory receipts reduced the number of samples for this study since the study only accepted proper documentation including the availability of those mentioned.
Conclusion(s)
Majority of the crowns prepared by UG dental students had an acceptable preparation with the exception of proximal reduction and cervical margin preparation that can be further improved and emphasised upon during the teaching and learning sessions. Moreover, the evaluation can be improved through the implementation of digital techniques measurement while evaluating each specific criterion.