Reliability of the Flexible Ruler in Measuring Lumbar Lordosis among Children
Reshma1, Mohamed Sherif Sirajudeen2, Thangadurai Chinnakalai3, Mohammad Suhail4, Nasser M Al-Hussinan5, Padmakumar Somasekharan Pillai6
1 Assistant Professor, Kanachur College of Physiotherapy, Mangalore, Karnataka, India.
2 Assistant Professor, Department of Physical Therapy and Health Rehabilitation, College of Applied Medical Sciences, Majmaah University, Majmaah, Saudi Arabia.
3 Associate Professor, Yenepoya Physiotherapy College, Yenepoya (Deemed to be University), Mangalore, Karnataka, India.
4 Dean, Kanachur College of Physiotherapy, Mangalore, Karnataka, India.
5 Head, Department of Physiotherapy and Rehabilitation, Hawtah Sudair Hospital, Riyadh, Saudi Arabia.
6 Principal, Yenepoya Physiotherapy College, Yenepoya (Deemed to be University), Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Reshma, Assistant Professor, Kanachur College of Physiotherapy, Deralakatte, Mangalore, Karnataka, India.
E-mail: reshphysio786@gmail.com
Introduction
Postural alignment is commonly assessed, and the abnormal postures are associated with musculoskeletal disorders. There are different methods for screening spinal column anomalies. The flexible ruler provides a safe, portable, inexpensive and non-invasive way to measure the spinal curvature in clinical and larger population.
Aim
To determine the intra-rater and inter-rater reliability of flexible ruler in measuring lumbar lordosis among children.
Materials and Methods
In this cross-sectional study 81 school children that fulfilled the criteria were recruited with age ranging from 9 to 15 years. Youdas method in standing position was adopted. By using flexible ruler, measurement was taken and without altering the shape of the lumbar curve it was traced in a graph sheet. By using straight ruler, line L and H were drawn by following deep point method. Lumbar lordosis angle was calculated by using the formula, θ=4Arctan 2H/L. Intra-rater reliability: Four measurements were taken by evaluator 1 with a gap of one minute between first two measurements and 3 minutes rest then other two measurements were taken with a gap of one minute between each. The average of first two and the last two measurements were considered as measurements 1 and 2. Inter rater reliability: Two measurements were taken by evaluator 2 by adapting the same procedure. The averages of two measurements were considered as measurement for evaluator 2. This value was correlated with the value of measurement 1 of evaluator 1. The data was analysed using Intra Class Correlation coefficient (ICC) test.
Results
The results showed high intra-rater reliability (ICC-0.991; p<0.001) for lumbar lordosis angle by flexible ruler and poor inter-rater reliability (ICC-0.241; p=0.11) for lumbar lordosis angle by flexible ruler.
Conclusion
The flexible ruler has shown only intra-rater reliability and additional studies are required to prove inter-rater reliability in measuring lumbar lordosis among children.
Lumbar region, Paediatrics, Range of motion, Spine
Introduction
The human spine acts as a multi-segmental, flexible curved rod which consists of 24 pre-sacral vertebrae that forms lordotic and kyphotic curves in the sagittal plane [1]. The vertebral column of the newborn at birth comprises of single long curve which is convex posteriorly [2]. The curves which retain the original posterior convexity throughout the life are primary curves (thoracic and sacral curves) called Kyphotic curve, the curves which show a reversal of posterior convexity are the secondary curves (lumbar and cervical curves) called Lordotic curve. The secondary spinal curves develop due to the weight bearing position [1-3]. Curve develops as the infant begins to walk and hold his/her trunk upright until growth stops somewhere between the age of 12 and 17 years [4]. Lumbar region has the lordotic curve which takes the repetitive load by providing “flex” or damping function. The main function of lumbar spine is stability with adequate mobility for daily activities. Mobility of the spine is affected by the age and gender. Muscles and ligaments play an important role in stabilising lumbar spine [1]. Postural alignment is commonly assessed, and the abnormal postures are associated with musculoskeletal disorders [5-8]. The lumbar region has the greater influence on the position of the pelvis. The pelvis should be in neutral position i.e., in transverse plane, Anterior Superior Iliac Spine (ASIS) are in level with Posterior Superior Iliac Spine (PSIS) and the ASIS is in the same vertical plane as the symphysis pubis. When the pelvis is in the neutral position, there is desired lumbar curvature or lordosis. If the pelvis is tilted anteriorly, it results in increased lumbar lordosis [9].
There are different methods for screening spinal column anomalies such as Kyphyometer [10], Inclinometer [11], Flexible ruler [12], Spinal mouse [13], Spinal pantograph [14] and Image processing methods [13]. X-ray radiography is a golden standard invasive method in lumbar lordosis measurement but is expensive, harmful and time consuming [15]. The flexible ruler provides a safe, portable, inexpensive and non-invasive way to measure the spinal curvature in clinical and larger population [12]. There are two methods when using flexible ruler to measure lumbar lordosis -deep point and midpoint of arch [16]. Seidi F et al., reported the construct validity of the flexible ruler method to measure lumbar lordosis by comparing with X-ray method (gold standard). The findings of the study by Seidi F et al., demonstrated good intra-tester (ICC=0.89) and inter-tester reliability (ICC=0.82) for flexible ruler method to measure lumbar lordosis [15]. In contrast, findings of Filho JCTS et al., showed poor inter-examiner reliability of the flexible ruler (ICC=0.31) [17]. The reliability based on ICC values: 0.90-0.99, high reliability; 0.80-0.89, good reliability; 0.70-0.79, fair reliability; and 0.69 and below, poor reliability [18].
Though the flexible ruler is not commonly used in India, it is widely used in clinical settings in some other countries, but few studies supporting the use of flexible ruler in measuring lumbar lordosis in children and no studies done in India related to reliability of flexible ruler in children [15,16]. So, the main purpose of the study was to check the Inter and Intra-rater reliability of flexible ruler on measuring lumbar lordosis angle in children.
Materials and Methods
This cross-sectional study was conducted at Dandatheertha Higher Primary School, Uliyargoli, Kaup, Udupi District, Karnataka, India in June 2014. The Yenepoya (Deemed to be University) Ethics Committee, Yenepoya (Deemed to be University), India, provided the ethical approval for this study (Approval. No. YUEC06/13/01/2014). A letter describing the purpose of the study and seeking the cooperation was sent to the Principal of the School. Each child’s parents/guardians were provided information about the study, after which they signed a written informed consent to permit their child to participate in the research. Moreover, assent was also obtained from the participating children before their enrolment in this study. The required sample was determined as 81 based on 80% power, 5% alpha error, sample reliability-0.9 and population reliability-0.82 for side-sided test [9].
Inclusion criteria: Children of both gender and the age ranging from 9 to 15 years were included in the study.
Exclusion criteria: Children with history of back pain, recent surgeries, trauma, spinal deformities, overweight {Body Mass Index (BMI) 25-29.9 kg/m2} and obese (BMI >30 kg/m2) were excluded [19,20].
Measurements of the lumbar lordosis were taken by two physical therapists with 5 and 2 years of clinical experience, respectively and were not among the authors of the study. The entire study was explained to the testers. Both testers independently practiced taking measurement at least for five times, before the study. The testers were involved only in taking measurements. The subjects were asked to stand in a relaxed position with the lower back and upper buttocks exposed. The subjects were told to stand in bare foot with body weight evenly distributed on the markings done by adhesive tape on the floor with the distance of 15 cm between feet. The subjects were made to stand with their arms at the sides and fix his/her eyes on the opposite wall [Table/Fig-1].
Markings on floor with distance of 15 cm.

The measurement was taken for lumbar lordosis by the flexible ruler (Saintograph measuring flexible curve: 40 cm, Model number 4-232M) was similar to the Youdas method [21], spinous process of (12th thoracic vertebra) T12 was the beginning point and (second sacral vertebra) S2 was the end point. The spinous process of T12 was palpated by identifying the inferior margins of last rib T12 bilaterally and then simultaneously palpating these rib margins while moving superiorly and medially with the distal tips of each thumb until they disappeared deep into the soft tissue. A removable marking was done using a skin marker at the center of spinous process of T12. Next, the tester palpated the S2 spinous process, which was assumed to be midway between the inferior aspects of the PSISs. A marking was done over the center of spinous process of S2 [Table/Fig-2].

The flexible ruler was then placed over the contour of the lumbar spinous process of the back and the readings on the flexible ruler that intersected with the markings done on spinous processes were noted [Table/Fig-3] [21].
Procedure of lumbar lordosis measurement using flexible ruler by tester.

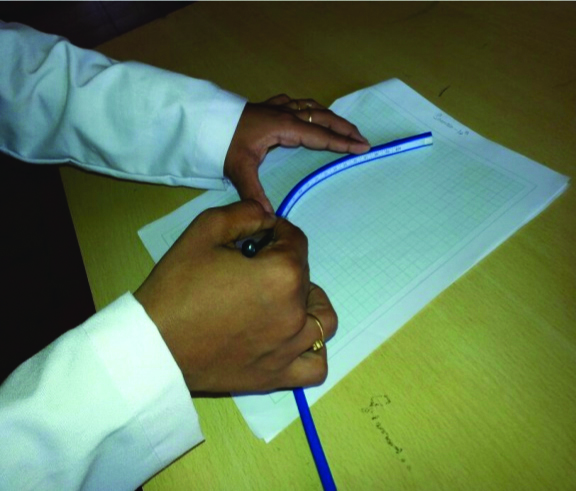
The measurements were recorded by the tester after carefully removing the flexible ruler without changing the curve. Then, the outline of the curve was traced from the readings noted for T12 to S2 spinous processes using a pencil along the flexible ruler onto the graph sheet [Table/Fig-4].
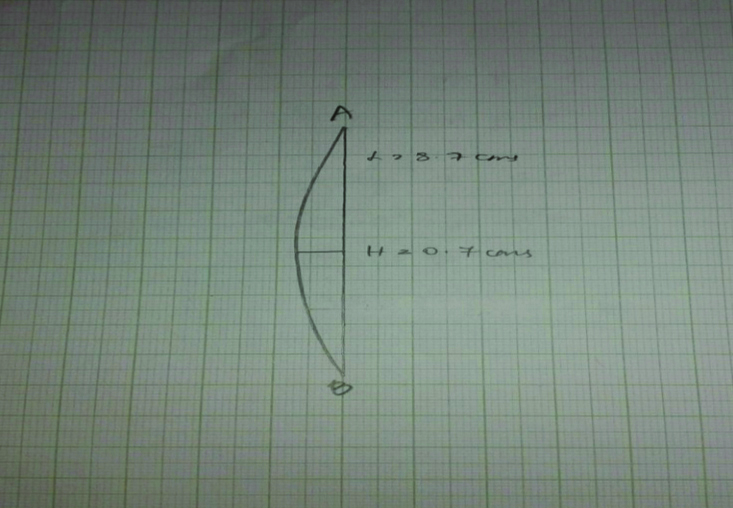
The vertical line (L) was drawn to connect the location of spinous processes T12 and S2 landmarks and were labelled as A and B respectively. The deepest point of the curve was identified by recording the steep of the curve and a perpendicular line (H) from the point to the line L was drawn. The length of the lines L and H were measured in cm [15,21] [Table/Fig-5].
Schematic for trignometric method.
Intra-Tester Reliability
After the procedure mentioned above, markings were removed using spirit and the subjects were given one-minute rest. The subjects were then asked to stand with their feet in same position as the first, and then the second measurement was taken by following the same procedure and the average of two measurements was taken. After this, the same procedure was repeated again by tester 1 for 2 times, after 3 minutes rest the average of these two measurements was taken. The two averages calculated were used for statistical analysis. Only one tester was present in the examination room at a time [22].
Inter-Tester Reliability
After measurements were taken by tester 1, each subject was given one-to three-minute rest. Then, each subject was measured by the tester 2 for 2 times with a gap of one minute, using the same procedure as the tester 1. The average of two measurements was taken. Both the testers were blinded about their measurement. In inter-rater reliability, the first average measurements of tester 1was compared with the measurement of the tester 2 [22].
Then using the formula, θ=4Arctan 2H/L, the index of lumbar lordosis was calculated for each subject [15,16,22,23].
θ=Index of lordosis (degrees);
L is the straight line from T12 to S2 vertebrae;
H is the distance between the deepest point of the lumbar curve and L.
In this study, the measurements of tester 1 were used to determine the intra-rater reliability and the inter-rater reliability, whereas, the measurements of tester 2 were used to determine inter-rater reliability only.
Statistical Analysis
Data collected was analysed using Statistical Package for the Social Sciences (SPSS) version 22. The mean and standard deviation of lumbar lordosis angle was calculated. ICC coefficient was used to analyse the reliability of flexible ruler. Level of significance was set up at p<0.05.
Results
The age and gender distribution of the subjects are presented in [Table/Fig-6]. The age varied from 9 to 15 years; mean age found to be 12.7 years with standard deviation of 1.97 years.
Age and gender distribution.
| Gender | Number | Age (years) |
|---|
| Mean | SD |
|---|
| Male | 41 | 12.85 | 1.66 |
| Female | 40 | 12.62 | 1.95 |
| Over all | 81 | 12.7 | 1.97 |
[Table/Fig-7] shows the Intra-rater reliability of flexible ruler. The ICC coefficient test showed ICC=0.991 with p-value <0.001, which reflects that there is a significant correlation between the measurements. This result showed that there is a high intra-rater reliability of flexible ruler used to measure the lumbar lordosis.
Intra-rater reliability of flexible ruler [18].
| Evaluator 1 | Mean (In degrees) | SD (In degrees) | Intra Class Correlation (ICC) | p-value |
|---|
| Measurement 1 | 37.66 | 6.67 | 0.991* | <0.001 |
| Measurement 2 | 37.34 | 6.55 |
Statistical tests used-lntraclass correlation coefficient; *(ICC values: 0.90-0.99, high reliability; 0.80-0.89, good reliability; 0.70-0.79, fair reliability; and 0.69 and below, poor reliability); p<0.05 is considered as statistically significant
[Table/Fig-8] shows the Inter-rater reliability of flexible ruler. The ICC coefficient test showed the value of ICC=0.241 with p=0.110, which reflect that there is no significant correlation between the measurements of two evaluators. This result shows that there is a poor inter-rater reliability of flexible ruler in measuring lumbar lordosis angle.
Inter-rater reliability of flexible ruler [18].
| Evaluator | Mean (In degrees) | SD (In degrees) | Intra Class Correlation (ICC) | p-value |
|---|
| Evaluator 1 | 37.66 | 6.67 | 0.241* | 0.110 |
| Evaluator 2 | 37.3 | 7.09 |
Statistical tests used- lntraclass correlation coefficient; *(ICC values: 0. 90-0.99, high reliability; 0.80-0.89, good reliability; 0.70-0.79, fair reliability; and 0.69 and below, poor reliability); p<0.05 is considered as statistically significant
Discussion
In this study flexible ruler was used to measure the lumbar lordosis angle in children and found higher degree of reliability when repeated by the same tester after a short period of time with an ICC=0.991(p<0.001) for intra-rater reliability. Walker ML et al., also reported high intra-rater reliability of flexible ruler (ICC- 0.90) among 31 young healthy physical therapy students [24]. Youdas JW et al., obtained an ICC of 0.87 for intra-rater reliability as good for measuring lumbar lordosis using flexible ruler on 10 healthy volunteers [21]. Seidi F et al., found high and good intra-rater reliability for lumbar lordosis angle by using flexing ruler with the ICC test values of 0.92 (p=0.01) and 0.89 (p=0.01) for first and second rater, respectively [15]. Inter-rater reliability of flexible ruler in measuring lumbar lordosis in this study was poor with an ICC value of 0.241(p=0.110). The same results were found in a study by Lovell FW et al., who also reported a poor inter-rater reliability (ICC=0.45) for measurement of lumbar lordosis using flexible ruler in 80 volunteers with and without Low Back Pain (LBP) [22]. Filho JCTS et al., studied the lumbar lordosis with flexible ruler in 37 physical therapy students and ICC between two evaluators was 0.37 indicating poor inter-rater reliability [17]. The high intra-rater reliability for flexible ruler reported in this study may be attributed to the manual location of anatomical landmarks (T12 and S2) by the same tester. The poor inter-rater reliability may be due to the discrepancy in manual location of anatomical landmarks by two different testers and also by changes in the posture of the subject due to changes in the posture of the subject due to fatigue from undergoing repeated measurements. According to Lovell FW et al., each millimeter of change in H value can also cause a change of 10° in the angle of flexi curve [22]. In this study, the measurements of tester 1 were used to determine the intra-rater reliability and the inter-rater reliability, whereas, the measurements of tester 2 were used to determine inter-rater reliability only. Hence, we could not determine the better rater among these two of them.
Limitation(s)
The limitation of the study is that there was no stabiliser used to control the forward sway when measuring the lumbar lordosis angle. The force exerted by the examiner in molding the flexible ruler on the spinous process was not controlled which could also change the curve.
Conclusion(s)
The measurement of lumbar lordosis using flexible ruler has shown high intra-rater reliability when measurements were taken by same therapist over a short period of time. Inter-rater reliability of flexible ruler in measuring lumbar lordosis in this study was poor. It is concluded that the flexible ruler has shown only intra-rater reliability and additional studies are required to prove inter-rater reliability of the flexible ruler in measuring lumbar lordosis.
Statistical tests used-lntraclass correlation coefficient; *(ICC values: 0.90-0.99, high reliability; 0.80-0.89, good reliability; 0.70-0.79, fair reliability; and 0.69 and below, poor reliability); p<0.05 is considered as statistically significant
Statistical tests used- lntraclass correlation coefficient; *(ICC values: 0. 90-0.99, high reliability; 0.80-0.89, good reliability; 0.70-0.79, fair reliability; and 0.69 and below, poor reliability); p<0.05 is considered as statistically significant
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 15, 2020
Manual Googling: Sep 30, 2020
iThenticate Software: Oct 26, 2020 (21%)
[1]. Oatis CA, Kinesiology The Mechanics and Pathomechanics of Human Movement 2004 1st editionLippincott Williams and Wilkins:540:560-561.:575:851 [Google Scholar]
[2]. Levangie PK, Norkin CC, Joint Structure and Function 2011 5th edition:140.502 [Google Scholar]
[3]. Hall SJ, Basic Biomechanics 1995 2nd edition:260-262. [Google Scholar]
[4]. Levangie PK, Norkin CC, Joint Structure and Function 2011 3rd edition:115 [Google Scholar]
[5]. Sirajudeen MS, Alaidarous M, Waly M, Alqahtani M, Work-related musculoskeletal disorders among faculty members of college of Applied Medical Sciences, Majmaah University, Saudi Arabia: A cross-sectional studyInternational Journal of Health Sciences 2018 12(4):18-25.PMID: 30022899; PMCID: PMC6040859 [Google Scholar]
[6]. Sirajudeen MS, Muthusamy H, Alqahtani M, Waly M, Jilani AK, Computer-related health problems among university students in Majmaah region, Saudi ArabiaBiomedical Research 2018 29(11):2405-15.10.4066/biomedicalresearch.61-18-418 [Google Scholar] [CrossRef]
[7]. Sirajudeen MS, Pillai PS, Vali GMY, Assessment of knowledge of ergonomics among information technology professionals in IndiaInternational Journal of Health and Rehabilitation Sciences 2013 2(4):192-97.10.5455/ijhrs.0000000170 [Google Scholar] [CrossRef]
[8]. Sirajudeen MS, Siddik SS, Knowledge of computer ergonomics among computer science engineering and information technology students in Karnataka, IndiaAsian Journal of Pharmaceutical Research and Health Care 2017 9(2):64-70.10.18311/ajprhc/2017/1102328770704 [Google Scholar] [CrossRef] [PubMed]
[9]. Lippert LS, Clinical Kinesiology for Physical Therapist Assistants 2002 3rd edition:401-403. [Google Scholar]
[10]. Greendale GA, Nili NS, Huang MH, Seeger L, Karlamangla AS, The reliability and validity of three non-radiological measures of thoracic kyphosis and their relations to the standing radiological Cobb angleOsteoporosis international 2011 22(6):1897-905.10.1007/s00198-010-1422-z20938766 [Google Scholar] [CrossRef] [PubMed]
[11]. Kolber MJ, Pizzini M, Robinson A, Yanez D, Hanney WJ, The reliability and the concurrent validity of measurement used to quantify lumbar spine mobility: An analysis of an iphone application and gravity based inclinometerThe International Journal of Sports Physical Therapy 2013 8(2):129-37. [Google Scholar]
[12]. Tizabi AAT, Mahdavinejad R, Azizi A, Jafarnejadgero T, Sanjari M, Correlation between height, weight, BMI with standing thoracic and lumbar curvature in growth agesWorld Journal of Sport Sciences 2012 7(1):54-56. [Google Scholar]
[13]. Yousefi M, Ilbeigi S, Mehrshad N, Afzalpour ME, Naghibi SE, Comparing the validity of non-invasive methods in measuring thoracic kyphosis and lumbar lordosisZahedan J Res Med Sci 2012 14(4):37-42. [Google Scholar]
[14]. Willner S, Spinal pantograph: A non-invasive technique for describing kyphosis and lordosis in the thoraco-lumbar spineActa Orthop Scand 1981 52:525-29.10.3109/174536781089921427331788 [Google Scholar] [CrossRef] [PubMed]
[15]. Seidi F, Rajabi R, Ebrahim TI, Tavanai AR, Moussavi SJ, The Iranian flexible ruler reliability and validity in lumbar lordosis measurementsWorld Journal of Sport Sciences 2009 2(2):95-99. [Google Scholar]
[16]. Rajabi R, Seidi F, Mohamadi F, Which method is accurate when using the flexible ruler to measure the lumbar curvature angle? Deep pin or Mid-point of arch?World Applied Sciences Journal 2008 4(6):849-52. [Google Scholar]
[17]. Filho JCTS, Abras ACV, Carvalho MT, Souza MGF, Souza AT, Costa LOP, Analysis of the interexaminer reliability of two clinical tests to measure the flexion range of motion of lumbar spineACTA FISIATR 2007 14(4):214-18. [Google Scholar]
[18]. Myers CR, Blesh TE, Measurement in Physical Education 1962 New YorkThe Ronald Press Company [Google Scholar]
[19]. Who EC, Appropriate body-mass index for Asian populations and its implications for policy and intervention strategiesLancet (London, England) 2004 363(9403):15710.1016/S0140-6736(03)15268-3 [Google Scholar] [CrossRef]
[20]. Centers for Disease Control and Prevention. Division of Nutrition, Physical Activity and Obesity, National Center for Chronic Disease Prevention and Health Promotion. (Available from: http://www.cdc.gov/obesity/childhood/defining.html) [Google Scholar]
[21]. Youdas JW, Suman VJ, Garrett TR, Reliability of measurements of lumbar spine sagittal mobility obtained with the flexible curveJournal of Orthopaedic & Sports Physical Therapy 1995 21(1):13-20.10.2519/jospt.1995.21.1.137889027 [Google Scholar] [CrossRef] [PubMed]
[22]. Lovell FW, Rothstein JM, Personius WJ, Reliability of clinical measurements of lumbar lordosis taken with a flexible rulePhysical Therapy 1989 69(2):96-102.10.1093/ptj/69.2.962521531 [Google Scholar] [CrossRef] [PubMed]
[23]. Youdas JW, Garrett TR, Harmsen S, Suman VJ, Carey JR, Lumbar lordosis and pelvic inclination of asymptomatic adultsPhysical Therapy 1996 76(10):1066-81.10.1093/ptj/76.10.10668863760 [Google Scholar] [CrossRef] [PubMed]
[24]. Walker ML, Rothstein JM, Finucane SD, Lamb RL, Relationship between lumbar lordosis, pelvic tilt & abdominal muscle performancePhysical Therapy 1987 67:512-16.10.1093/ptj/67.4.5122951745 [Google Scholar] [CrossRef] [PubMed]