Thyroid nodules are seen in about 12.2% of population in India and incidence of thyroid carcinoma is around 8.7 per 100,000 people per year [1,2]. Many different techniques are used for diagnosis of thyroid lesions, including radionuclide scanning, high-resolution ultrasonography and FNAC [3]. FNAC is an increasingly common procedure in the diagnosis of neoplastic lesions. In spite of all its documented advantages, sometimes FNAC may not be able to bring forth an accurate diagnosis and the risk of false negative diagnoses is inherent. This could be attributed to inadequate spreading, presence of artifacts and dense tissue remains [4]. Also, FNAC is a predominantly operator-dependent technique. Inconclusive diagnosis on FNAC may be attributed to procedural errors in drawing samples, haemorrhagic or a pauci-cellular aspirates and incorrectly sampled lesions especially in case of small swellings [5]. Further in case of highly vascular organs like thyroid, it often yields hemorrhagic aspirate which reduces its diagnostic efficacy. Cell blocks have been extensively promoted as an adjunct to FNAC in evaluating neck lesions as they aid in providing architectural details which supplements FNAC as suggested by Akalin A et al., [6].
Cell block technique combines the advantages of FNAC in being fast and safe and providing a precise diagnostic architecture similar to a histological diagnosis. It may be superior in diagnosing neoplasms, as many a times diagnosis met by the cytologic criteria and histologic criteria do not correlate and hence, to avoid any pitfalls by using either of them alone, cell block and smears can be used together to reach a diagnosis [7]. Qiu et al., also advocated the use of cell block, especially for processing hemorrhagic thyroid aspirates [8].
Conventional FNAC for cystic thyroid nodules has a high rate of non-diagnostic and false negative results as it yields a large amount of fluid that cannot be processed. Cell block may resolve this problem, as a large amount of the fluid aspirated is centrifuged and cell block prepared from it [9]. Moreover, 10% formal-alcohol used for fixation causes proteins to be cross-linked and a gel is formed, which does not get dissolved in any material used for processing, thus, minimising the cell loss [10]. Cell block also better delineates the few follicular cells that may appear within a large number of degenerated cells. Thus, it helps in easily ruling out malignancy and in preventing a misdiagnosis.
According to previous studies using variable methodologies, sensitivity, specificity and diagnostic accuracy of FNAC and Cell Block ranges from 65 to 100% [10,11]. The current study aims to assess the diagnostic efficacy of FNAC and cell block in thyroid lesions and compare it with final histopathological diagnosis (after excision) in case of malignancies and clinico-radiological follow-up in case of benign lesions.
Materials and Methods
The present observational study was conducted over a period of one year from 1st November, 2016 to 31st October, 2017 after obtaining approval from the Institutional Ethics Committee of a Tertiary Care Teaching Hospital in Northern India. All patients referred to cytology section of Department of Pathology for FNAC thyroid were included in the sample, ensuring confidentiality. Cases yielding inadequate material for cell block, patients not ready to give consent for the FNAC thyroid and patients with bleeding disorders or on anticoagulation therapy were excluded. Written consent was sought and FNAC was done. Aspirated material was subjected to direct smears as well as cell block study and subsequent microscopic examination of the same was done.
FNAC was performed under aseptic precautions using 25-27 G needle attached to 20 mL syringe with a Cameco syringe holder.
A) Direct Smear on Glass Slide
After procuring the specimen onto the surface of previously labelled clean glass slides, tongue-shaped smears were prepared on the middle third of the slide. Usually four slides were prepared, two slides were instantly inserted in coplin jar for wet fixation- Papanicolaou (PAP) staining. Other two were air-dried for May Grunwald Giemsa (MGG) staining. This could vary depending on the amount of material aspirated.
B) Preparation of Cell Block [
10]
After preparing smears, needles and syringes used for attaining fine needle aspirates were bathed in 10 mL of 50% ethanol in a specimen container. Left over clots or tissue remnants left in the hub of needles were removed cautiously with the help of another needle and rinsed in 50% ethanol followed by centrifugation of this material in a 10-mL disposable centrifuge tube at 4,000 rpm for six minutes to produce one pellet in most cases. The supernatant fluid thus obtained, was emptied and the residue fixed (for 45 minutes) in freshly prepared Nathan Alcohol Formalin Substitute (NAFS) consisting of nine parts of 100% ethanol and one part of 40% formaldehyde. The fixed cell pellets were then, recentrifuged at 4,000 rpm for six minutes. After centrifugation, these pellets either detach themselves or can be removed easily with a single use Pasteur pipette. The cell pellets were enveloped in filter paper, positioned in a cassette, and kept in 80% ethanol pending processing in the automatic tissue processor using a 13-hours processing schedule as follows: 80% ethanol with one change (2.5 hours); 95% ethanol (one hour); 100% ethanol, four times (one hour each); 1:1 ethanol/xylene (one hour); xylene, three times (one hour each). The cell blocks were embedded in paraffin and sectioned at 3 μm thickness. The cytomorphology of FNA smears was compared with histopathology of cell blocks in all cases.
Specimens with insufficient cellularity i.e. less than five to six groups of follicular epithelial cells with ten or more cells per group on conventional smears and cell block negative for follicular cell were considered as “Suspicious” according to the adequacy assessment protocol taken from Goellner et al., [12]. To ensure quality control in this study, 10% of slides were examined by an independent consultant pathologist who was blinded to the previous results.
Study specimens were categorised into neoplastic, non-neoplastic and non-diagnostic/suspicious of malignancy. Following the FNAC/Cell Block, all the patients with diagnosis of neoplasm were subjected to surgery. The thyroid specimens which were excised during surgical procedures were processed in automated tissue processing units and sent for histopathological examination. The report of FNAC and Cell Block was then compared with final HPE report after excision. For neoplastic lesions, the final histologic diagnosis after excision and for benign lesions, assessment by clinical/radiological follow-up were considered the gold standard.
Statistical Analysis
The results were tabulated as proportions and the sensitivity, specificity, diagnostic accuracy, Positive Predictive Value (PPV) and Negative Predictive Value (NPV) were calculated for both FNAC and Cell Block techniques using MedCalc Statistical Software version 19.3.
Results
A total of 100 patients were enrolled in the study. Mean age of the patients was 42.75±15.75 years with a range of 12-75 years. Females constituted 88% of the sample with male to female ratio of 1:7.3. Among 100 cases, diffuse thyroid swelling was present in 65%, solitary nodule in 32% cases, of which right side thyroid swelling was present in 21% and left side in 11% cases and multinodular swelling was seen in 3% patients. 45%patients reported duration of thyroid swelling ranging from 1 to 12 months while the mean duration of thyroid swelling was 4.43 years with a range of three days to forty years. Blood mixed aspirate was present in 55% patients, followed by colloid aspirate in 42%, and brown colour fluid, straw colour fluid, yellowish fluid aspirated in 1% patients each.
[Table/Fig-1] revealed that 88% lesions were benign, 8% were malignant and 4% non-diagnostic/suspicious of malignancy on conventional smears in comparison to cell block which showed 90% as benign, 8% as malignant and 2% suspicious lesions. However, combination of the cell block and direct smears improved a gain in diagnosis, as four cases showing merely haemorrhagic material on conventional direct smears were diagnosed on cell block as one case of colloid goitre, one case of chronic lymphocytic thyroiditis and two cases of adenomatous goitre. Also, two cases showing haemorrhagic material on cell block were diagnosed as chronic lymphocytic thyroiditis on direct smears [Table/Fig-2]. Colloid goitre was the most common non-neoplastic lesion observed in both direct smear and cell block technique [Table/Fig-3,4] while papillary carcinoma was the commonest type of the neoplasm observed with both the techniques [Table/Fig-5,6].
Categorisation of patients according to direct smears and cell block diagnoses.
| Category | Diagnosis | Direct smears | Cell block | Final diagnosis (HPE/Clinical-radiological follow-up) |
|---|
| Non-Neoplastic (NN) | Colloid goitre | 52 | 53 | 53 |
| Adenomatoid goitre | 6 | 8 | 8 |
| Multinodular goitre | 3 | 3 | 3 |
| Colloid cyst | 4 | 4 | 4 |
| Acute thyroiditis | 1 | 1 | 1 |
| Chronic lymphocytic thyroiditis | 16 | 15 | 17 |
| Hashimoto’s thyroiditis | 6 | 6 | 6 |
| Neoplastic (N) | Papillary carcinoma | 4 | 4 | 4 |
| Follicular neoplasm | 1 | 1 | 1 |
| Hurthle cell neoplasm | 1 | 1 | 1 |
| Medullary carcinoma | 1 | 1 | 1 |
| Undifferentiated carcinoma | 1 | 1 | 1 |
| Non-Diagnostic (ND)/Suspicious of malignancy | 4 | 2 | 0 |
| Total | 100 | 100 | 100 |
HPE: Histopathological examination
Cytohistological correlation of direct smears and cell blocks.
| Diagnosis | Direct smears | Remarks | Cell block | Remarks |
|---|
| Colloid goitre | 52 | TN | 53 | TN |
| Adenomatoid goitre | 6 | TN | 8 | TN |
| Multinodular goitre | 3 | TN | 3 | TN |
| Colloid cyst | 4 | TN | 4 | TN |
| Acute thyroiditis | 1 | TN | 1 | TN |
| Chronic lymphocytic thyroiditis | 16 | TN | 15 | TN |
| Hashimoto’s thyroiditis | 6 | TN | 6 | TN |
| Papillary carcinoma | 4 | TP | 4 | TP |
| Follicular neoplasm | 1 | TP | 1 | TP |
| Hurthle cell neoplasm | 1 | TP | 1 | TP |
| Medullary carcinoma | 1 | TP | 1 | TP |
| Undifferentiated carcinoma | 1 | TP | 1 | TP |
| Non-Diagnostic (ND)/Suspicious of Malignancy | 2 Adenomatous goitre | FP | 2 Chronic lymphocytic thyroiditis | FP |
| 1 Colloid goitre | FP |
| 1 Chronic lymphocytic thyroiditis | FP |
| Total | 100 | | 100 | |
TN: True negative; TP: True positive; FP: False positive
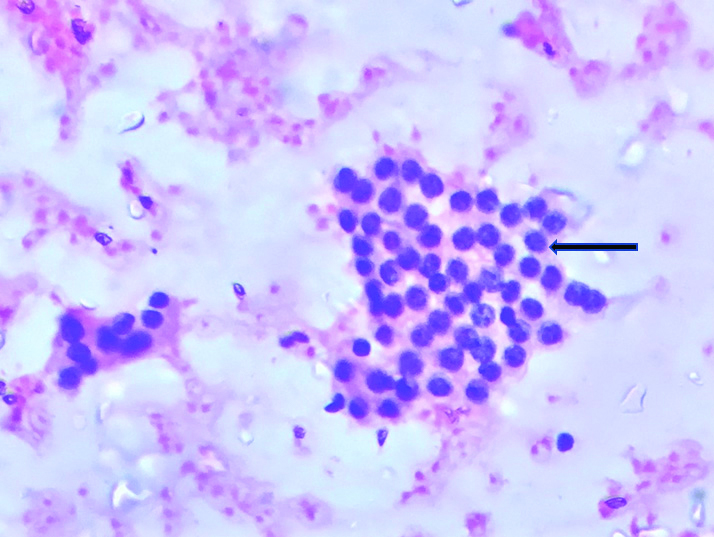
Colliod Goitre: Follicular cells arranged in monolayered sheet in background of colloid and hemorrhage. (CONVENTIONAL SMEAR,PAP 100x).
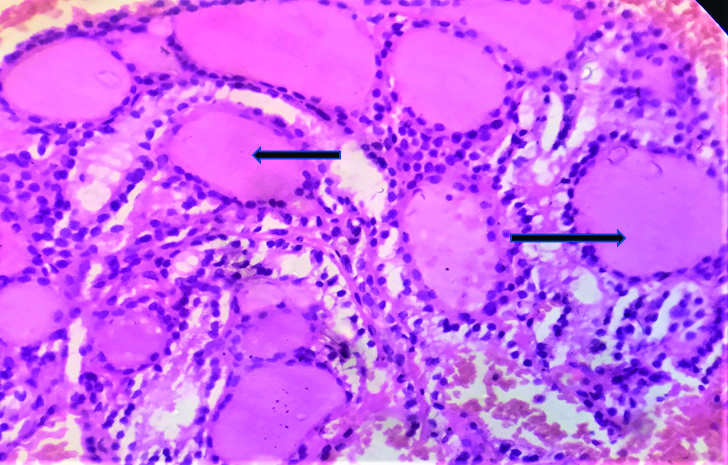
Colliod Goitre: Variable sized thyroid follicles filled with colloid (CELL BLOCK H&E 100X).
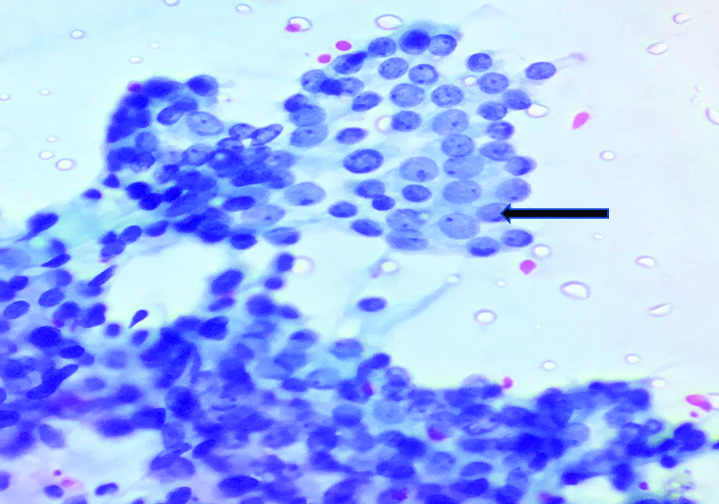
Papillary Carcinoma: Oval cell with moderate amount of often dense granular cytoplasm, well-defined cell border and powdery chromatin. (CONVENTIONAL SMEAR, PAP 400X).
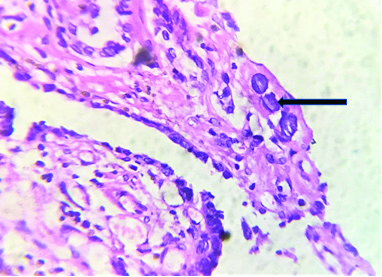
Papillary Carcinoma: Concentric laminated dark blue structure (CELL BLOCK, H&E 400x). (Psammoma bodies)
The sensitivity, specificity, Positive Predictive Value (PPV), Negative Predictive Value (NPV) and accuracy for FNAC was found to be 100%, 95.65%, 66.67%, 100.00% and 96.00% respectively, whereas for cell blocks these statistics were 100%, 97.83%, 80%, 100% and 98% respectively [Table/Fig-7,8].
Summary Results for FNAC and Cell Block Technique.
| Results | FNAC | Cell block |
|---|
| Cancer present | Cancer absent | Cancer present | Cancer absent |
|---|
| Test positive | 8 (TP) | 4 (FP) | 8 (TP) | 2 (FP) |
| Test negative | 0 (FN) | 88 (TN) | 0 (FN) | 90 (TN) |
| Total | 8 | 92 | 8 | 92 |
TN: True negative; TP: True positive; FP: False positive; FN: False negative
Summary Statistics for FNAC and Cell Block Technique.
| Statistics | FNAC | Cell block |
|---|
| Value | 95% CI | Value | 95% CI |
|---|
| Sensitivity | 100.00% | 63.06% to 100.00% | 100.00% | 63.06% to 100.00% |
| Specificity | 95.65% | 89.24% to 98.80% | 97.83% | 92.37% to 99.74% |
| Positive likelihood ratio | 23 | 8.82% to 59.98% | 46 | 11.68% to 181.17% |
| Negative likelihood ratio | 0 | - | 0 | - |
| Disease prevalence | 8.00% | 3.52% to 15.16% | 8.00% | 3.52% to 15.16% |
| Positive predictive value | 66.67% | 43.41% to 83.91% | 80.00% | 50.39% to 94.03% |
| Negative predictive value | 100.00% | - | 100.00% | - |
| Accuracy | 96.00% | 90.07% to 98.90% | 98.00% | 92.96% to 99.76% |
Discussion
The mean age of the patients in the present study was 42.75 years. These findings are in agreement with studies by Hegazy RA et al., Afroze et al., Madakshira MG et al., Islam M S et al., and Venkatachalapathy et al., where 40, 40.2,38.7, 37.7 and 35.4 years, respectively, was found to be the mean age group when thyroid lesions were studied [9,13-16]. In the present study, females (88%) outnumbered males with a male to female ratio of 1:7.3. This finding was in agreement with another study that reported the male to female ratio of 1: 6.5 [17]. Female preponderance was also seen in other studies that reported female proportion of 71.76% and 69% respectively [13,16].
The findings of the present study are in concord with study done by Ahmed Z et al. They observed that FNAC diagnosed 83.33% as non-neoplastic, of which colloid goitre constituted 74.44% cases, adenomatoid goitre 5.56% cases, thyroid cyst 2.22% cases and Hashimoto’s thyroiditis 1.11% cases. The neoplastic diagnosis was made in 14.44% cases. They were diagnosed as- follicular neoplasm, papillary carcinoma and anaplastic carcinoma. The proportion of non-diagnostic cases were 2.22%. By cell block technique, the non-neoplastic cases were 64.44% and comprised of colloid goitre, adenomatous goitre, multinodular goitre, thyroid cyst and Hashimoto’s thyroiditis. The neoplastic cases were: follicular adenoma in 11.11% cases, follicular neoplasm in 5.56% cases, papillary carcinoma in 4.44%, medullary carcinoma and anaplastic carcinoma in 1.11% cases each [18].
During the FNAC procedure, aspirated material could clot in the needle hub which was difficult to flush onto the slide for conventional smears. This clotted material in the hub was removed and used for cellblock preparation. This could explain why four samples which were non-diagnostic on conventional smear were satisfactory on modified cell block.
In comparison to four smears that showed haemorrhagic material on conventional direct smears, cell block smears showed only two smears with haemorrhagic material. These finding are in accord to Qui L et al., who concluded that Cell Block alone was superior to direct smears for hemorrhagic thyroid aspirates [8].
The present study showed that the combination of the cell block with direct smears improved a 4% gain in diagnosis, as four cases showing merely haemorrhagic material on conventional direct smears were diagnosed on cell block giving us 100% diagnosis. These results were in concord with a study done by Rajib RC et al., who found that by adding cell block technique, 12.5% inadequate direct smears could yield a diagnosis, increasing the percentage of adequate cases to 95.7%. De lima MA et al., also suggested similar findings [19,20].
In case of FNAC, results were comparable with published data as demonstrated in [Table/Fig-9]. The determinant factor for such a wide range of difference may be due to differences in number of cases, the included diagnostic categories, and how the cytopathologists classify ‘suspicious’, Follicular Lesion of Undetermined Significance (FLUS), as well as false positive and negative samples. Some authors include follicular lesion in the neoplastic group, whereas others exclude them from the calculations [21]. However, in case of cell blocks, different authors have reported sensitivities ranging from 60%-89.4% [10]. In another study from Brazil, the sensitivity and specificity for cell block was 100% and 90%, respectively, and the accuracy, PPV and NPV were 94%, 88 %and 100%, respectively, which is in tune with the findings of the present study [22]. In line with the findings of the present study, diagnostic accuracy of cell block alone was reported to be 100% by Basnet S et al., who also observed that when smear and cell block were used simultaneously, the diagnostic accuracy of tumours approached 100% which is in concordance with present findings [7].
Accuracy, sensitivity, specificity, false positives and false negatives of FNAC in various studies.
| Parameter | Islam et al., [15] | Venkatachalapathy TS et al., [16] | Sikder MAH et al., [23] | Sengupta et al., [24] | Syed O, Auti A [25] | E.A. Sinna, N. Ezzat [11] | Kulkarni P [26] | Sharma R et al., [27] |
|---|
| Sensitivity % | 76.68 | 74 | 94.7 | 90 | 77.78 | 92.8 | 100 | 84 |
| Specificity % | 97.26 | 100 | 94 | 100 | 100 | 94.2 | 94.2 | 100 |
| Accuracy % | 94.44 | - | 94.2 | 98.3 | 98.1 | 93.6 | 95 | 90 |
| FP (n) | 2 | 0 | 5 | 0 | 0 | 18 | 2 | 0 |
| FN (n) | 5 | 42 | 2 | 2 | 2 | 16 | 0 | 4 |
FP: False positive; FN: False negative
Thus, the results of present study are akin to the published literature and establish that FNAC and cell blocks are sensitive, specific, and accurate as preliminary diagnostic tests for assessment of patients with thyroid masses. Their concomitant use can reduce the number of patients with benign thyroid nodules undergoing unnecessary surgery and can aid in avoiding delays in planning of surgery in malignant cases. This study clearly shows the added advantages of performing cell block in thyroid FNAC aspirations.
Limitation(s)
No dedicated passes were done for modified cell block preparation, thus, limiting the effectiveness of the method.
Conclusion(s)
Cell block improved the diagnostic accuracy of FNAC when used as an adjunct leading to 100% diagnostic yield. However, benign FNAC findings should be viewed with discretion as false negative results can occur mainly due to inter-observer and intra-observer variability, especially in indeterminate cases. These patients should be followed-up clinically and radiologically for any advancement of disease symptomology that may warrant repeat FNAC and/or surgery.
HPE: Histopathological examination
TN: True negative; TP: True positive; FP: False positive
TN: True negative; TP: True positive; FP: False positive; FN: False negative
FP: False positive; FN: False negative