Case Report
A 26-year-old male patient presented with the chief complaint of intermittent pain over three months with respect to lower right posterior teeth region. The pain was dull, moderate and intermittent in nature which aggravated on intake of hot food and beverages, and was relieved on its own. It was not associated with any diurnal or postural variations. Dental history revealed that the patient had undergone root canal treatment with respect to mandibular second premolar six months ago. Medical history was non contributory.
On clinical examination, right mandibular second premolar was found to be tender on percussion. Heat and cold tests were negative, while there was a delayed response with electric pulp test. No evidence of swelling or sinus tract was associated with the same.
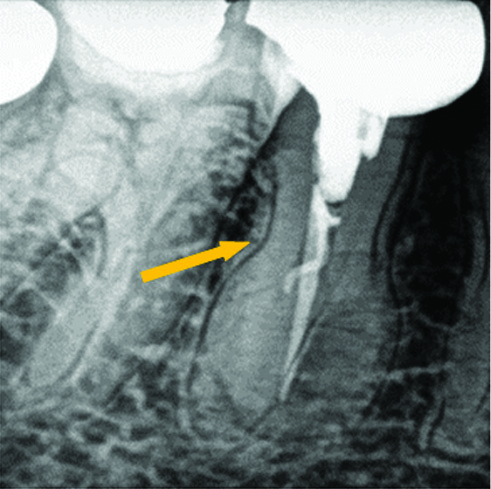
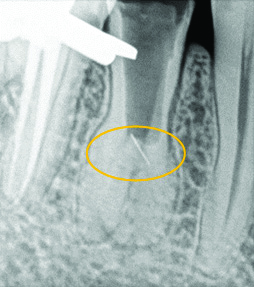
Preoperative periapical radiograph (with the x-ray beam projected perpendicular to the tooth in bucco-lingual direction) revealed incomplete endodontic treatment w.r.t. 45. Slight widening of the periodontal ligament space and thickening of the lamina dura were noticed. In addition, an unusual root anatomy was evident on the radiograph. The mid-root diameter was large and unusual which suggested the presence of extra roots [Table/Fig-1].
Preoperative radiograph revealing incomplete endodontic treatment and an unusual increased mid-root diameter w.r.t. 45.
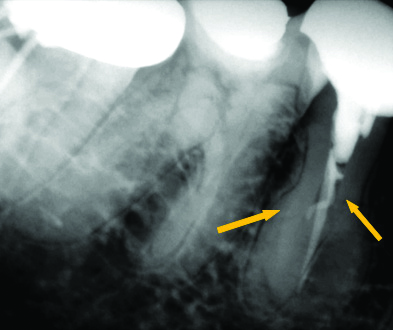
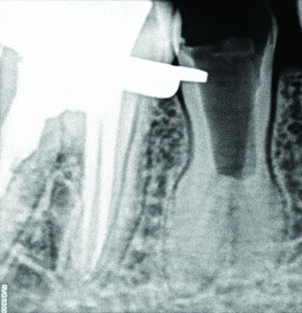
Hence, a second angulated radiograph at a horizontal angle of 20° from the distal aspect of the tooth was taken. Thin radiolucent lines were evident on either side of the main canal, which led to the diagnosis of extra roots and canals [Table/Fig-2].
Angulated radiograph revealing radiolucent lines present mesial and distal to the main canal suggestive of additional canals.
Due to financial constraints the patient was reluctant for a Cone Beam Computed Tomography (CBCT) scan.
Based on clinical and radiographic evidences, a diagnosis of symptomatic apical periodontitis associated with previously treated tooth was established.
Patient was informed about the treatment and after obtaining informed consent; non-surgical endodontic retreatment was initiated with respect to 45.
After administering of local anaesthesia (2% lidocaine with 1:80,000 adrenaline) the prosthetic coverage (full metal crown) was removed using tungsten carbide bur (Neo Burr Max2®). Rubber dam was applied and access was gained to the pulp chamber using EndoAccess bur (Size no. 2) (Mani, Inc., Japan).
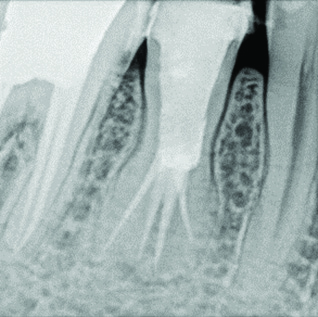
On removal of the previously placed composite as post-obturation restoration, the obturated canal was cleared of the gutta-percha using gutta-percha solvent (RC Solve®, Prime Dental Products, India) and No. 25 H-file (Dentsply Maillefer, Switzerland) [Table/Fig-3]. The chamber was thoroughly irrigated using saline solution following the complete removal of the gutta-percha.
Removal of previously placed gutta-percha from the canals.
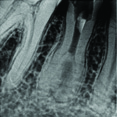
To gain sufficient access to canals, the conventional access opening was modified to have more width mesio-distally. Radiographically, the mid-root diameter appeared to be more than the crown diameter [Table/Fig-3].
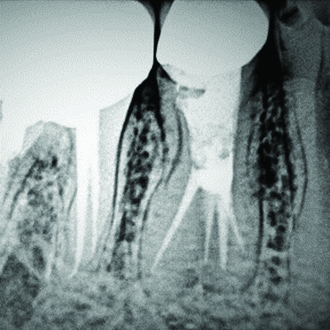
Working length determination radiograph, with the four K-files in four separate root canals (Mesio-buccal, Disto-buccal, Mesio-lingual and Disto-lingual).
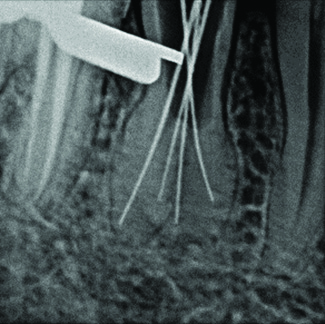
Tactile examination of the walls of major canals was implemented with a small pre-curved No. 10 K-file (Mani, Inc., Japan) which was slowly glided along each wall of the major canals, probing for a catch. A slight catch was appreciated along the buccal and lingual walls which gave an indication about the presence of additional canal orifices. Four separate orifices were located: two buccally, and two lingually. Patency was ascertained with a small size No. 10 K-file (Mani, Inc., Japan). The working length was determined by using an apex locator (Root ZX®, J. Morita Corporation, Japan) and confirmed radiographically [Table/Fig-4]. A working length of 14 mm was established for mesio-buccal and disto-buccal canals and 13.5 mm for the mesio-lingual and disto-lingual canals. While cleaning the mesiobuccal canal, 4.5 mm of #15-K file (Mani, Inc., Japan) was separated at the orifice level [Table/Fig-5]. The separated file was successfully retrieved using H-file (Dentsply Maillefer, Switzerland) [Table/Fig-6].
Instrument separation (#15 K-file, 4.5 mm) in mesio-buccal canal.
Retrieval of the separated instrument using H-file.
After the retrieval, canals were cleaned and shaped sequentially by crown down technique with No. 10 C+ files (Dentsply Maillefer, Switzerland) and till 25/.04 rotary ProTaper files (Dentsply, Maillefer, Switzerland), irrigated with the alternate use of 5.25% sodium hypochlorite (Prime Dental Products, India) and 17% liquid EDTA (SmearClearTM, SybronEndo, USA) and a final rinse of normal saline. Canals were dried with paper points (Medicept, United kingdom) and calcium hydroxide was placed as the intracanal medicament. Cotton was placed in pulp chamber and CavitTM (ESPE, Seefeld, Germany) was used to seal the access cavity. The patient was recalled after eight days. At the second appointment, the patient was asymptomatic. Calcium hydroxide was flushed out using normal saline. Master cone selection was done and the canals were obturated with 4% No.25 gutta-percha cones (Dentsply Maillefer, Switzerland) and AH Plus sealer (Dentsply Maillefer, Switzerland) [Table/Fig-7], by cold lateral compaction technique, using Buchanan hand pluggers (SybronEndo®, USA). The access cavity was sealed using resin composite (3M ESPE®, USA). The patient was recalled after seven days. The patient was found to be asymptomatic and hence, full coverage Porcelain Fused to-Metal (PFM) crown prosthesis was placed on the tooth [Table/Fig-8].
Immediate postobturation radiograph showing four distinct obturated root canals w.r.t. 45, and access cavity sealed with composite resin.
Porcelain Fused to-Metal (PFM) crown w.r.t. 45.

A one-year follow-up radiograph revealed satisfactory healing [Table/Fig-9] and the tooth was asymptomatic.
Follow-up radiograph radiograph one-year postoperatively w.r.t. 45.
Discussion
The root canal system in mandibular premolars comprises of complex anatomical features where the presence of extra canals is an endodontic challenge [1]. In order to accomplish this, the clinician should have adequate and accurate knowledge of the normal root canal anatomy and common variations [2]. Hoen MM and Pink PE found that missed canals were the major cause of endodontic retreatment in 42% of cases studied [3]. Mandibular premolars exhibit an aberrant root canal anatomy [4]. Literature has reported the presence of more than two roots and root canals of mandibular second premolars in varying percentages [Table/Fig-10] [5-9].
Literature review depicting aberrant canal anatomy of mandibular second premolar [5-9].
| Author | Year | Canal configuration |
|---|
| Wong M [5] | 1991 | Four canals |
| Holtzman L [6] | 1998 | Four canals |
| Al-Fouzan KS [7] | 2001 | Four canals |
| Farmakis ET [8] | 2008 | Four roots and four root canals |
| Sinanoglu A et al., [9] | 2015 | Four canals |
Owing to the fact that so many variations exist, it becomes imperative that when a patient presents with persistent pain or sensitivity to hot and cold even after root canal treatment, the clinician must begin to suspect the presence of any missed canals [10].
Al-Attas H and Al-Nazhan S had reported a similar case of mandibular second premolar with three root canals, where endodontic retreatment was carried out due to the missed third canal. They diagnosed the presence of an extra root canal midway between the buccal and lingual canals on access cavity modification [11].
Paul B and Dubey K reported a case of mandibular second premolar exhibiting an aberrant canal anatomy. The author diagnosed an unusual pattern of the root on radiographic examination, followed by a modification of the conventional access cavity leading to the detection of three root canals [12].
Al-Shawwa S et al., reported the occurrence of Type IX canal configuration in mandibular second premolar. The main canal trifurcated into three separate root canals at the middle third, and later merged in the C-shaped canal [13].
A study at the University of Washington showed failure rate of 11.45% and 4.54% of all types of mandibular first and second premolars [14]. Careful use of endodontic instruments, contemporary methods of determining extra roots and root canals and high end diagnostic aids should be employed in dealing with such complex situations [10].
A large number of classification systems and their modifications pertaining to numerous root canal configurations are available in the literature [15,16].
In the present case, mandibular second premolar had Sert and Bayirli’s canal Classification Type XX (4-4) i.e., four canals start from the pulp chamber and continue throughout the canal to exit as four canals [16]. The additional third and fourth canals were undetected which ultimately led to the endodontic treatment failure. The clinicians could suspect the presence of third and fourth canals clinically when the pulp chamber alignment is lacking in its classic bucco-lingual relationship, or if there is a significant difference from the normal configuration and has a triangular appearance, or if there is presence of an additional cusp, or its size is remarkably large in mesiodistal plane [7].
If the tooth appears to have one large canal in the cervical third of the root which disappears or constricts as it travels in an apical direction (Fast break), multiple canals should be suspected [17].
Other diagnostic aids which help in the detection of extra roots and root canals include two or more periapical radiographs taken at different horizontal angulations (40 degrees), attention to the colour changes on the pulpal floor and wall during inspection and following the dentinal maps, tactile examination of all the walls of the major canal with a small, pre curved K-file tip, instruments such as Micropeners and DG16 endodontic explorer, troughing of anatomic grooves with ultrasonic tips to facilitate canal location, staining the chamber floor with dyes such as 1% methylene blue and transillumination, performing “Champagne Bubble Test” by flooding sodium hypochlorite in access cavity and root canal bleeding points [7,17,18].
Radiographs are two-dimensional representations of a three-dimensional object. They furnish a gross information to the clinician about the presence of aberrant canal anatomy in the tooth. Hence, recently various 3-D scans as Spiral Computed Tomography, CBCT, micro-computed tomography (μCT) have been employed to not only establish a confirmatory diagnosis of the morphological aberrations, but also ascertain the exact root and root canal anatomy [10].
The presence of missed and incompletely obturated root canals in this case could have probably led to the persistence of clinical symptoms and subsequent failure of endodontic therapy.
Conclusion(s)
The anatomy of the mandibular second premolar can be complex. The success of the present case can be attributed to the proper diagnosis, thorough chemo-mechanical debridement and complete obturation of all the four root canals.
[1]. Sonarkar S, Purba R, Badole G, Makade C, Unusual root canal morphology of mandibular second premolar: A case series and reviewJ Dent Res Rev 2017 4(4):107-13.10.4103/jdrr.jdrr_64_17 [Google Scholar] [CrossRef]
[2]. Macri E, Zmener O, Five canals in a mandibular second premolarJ Endod 2000 26(5):304-05.10.1097/00004770-200005000-0001611199743 [Google Scholar] [CrossRef] [PubMed]
[3]. Hoen MM, Pink FE, Contemporary endodontic retreatments: An analysis based on clinical treatment findingsJ Endod 2002 28(12):834-36.10.1097/00004770-200212000-0001012489654 [Google Scholar] [CrossRef] [PubMed]
[4]. Nallapati S, Three canal mandibular first and second premolars: A treatment approachJ Endod 2005 31(6):474-76.10.1097/01.don.0000157986.69173.a615917692 [Google Scholar] [CrossRef] [PubMed]
[5]. Wong M, Four root canals in a mandibular second premolarJ Endod 1991 17(3):125-26.10.1016/S0099-2399(06)81744-9 [Google Scholar] [CrossRef]
[6]. Holtzman L, Root canal treatment of mandibular second premolar with four root canals: A case reportInt Endod J 1998 31(5):364-66.10.1046/j.1365-2591.1998.00166.x9823141 [Google Scholar] [CrossRef] [PubMed]
[7]. Al-Fouzan KS, The microscopic diagnosis and treatment of a mandibular second premolar with four canalsInt Endod J 2001 34(5):406-10.10.1046/j.1365-2591.2001.00408.x11482725 [Google Scholar] [CrossRef] [PubMed]
[8]. Farmakis ET, Four-rooted mandibular second premolarAust Endod J 2008 34(3):126-28.10.1111/j.1747-4477.2007.00092.x19032648 [Google Scholar] [CrossRef] [PubMed]
[9]. Sinanoglu A, Helvacioglu-Yigit D, Mutlu I, Use of cone-beam computed tomography and three-dimensional modeling for assessment of anomalous pulp canal configuration: A case reportRestor Dent Endod 2015 40(2):161-65.10.5395/rde.2015.40.2.16125984479 [Google Scholar] [CrossRef] [PubMed]
[10]. Sachdeva GS, Ballal S, Gopikrishna V, Kandaswamy D, Endodontic management of a mandibular second premolar with four roots and four root canals with the aid of spiral computed tomography: A case reportJ Endod 2008 34(1):104-07.10.1016/j.joen.2007.10.00418155506 [Google Scholar] [CrossRef] [PubMed]
[11]. Al-Attas H, Al-Nazhan S, Mandibular second premolar with three root canals: Report of a caseSaudi Dent J 2003 15(3):145-47. [Google Scholar]
[12]. Paul B, Dubey K, Endodontic management of mandibular second premolar with three canalsClujul Med 2018 91(2):234-37.10.15386/cjmed-87529785164 [Google Scholar] [CrossRef] [PubMed]
[13]. Al-Shawwa S, Al Khairallah Y, Alenazy M, Al Dayel O, Endodontic management of mandibular second premolar with Type IX canal configuration using cone beam computed tomographySaudi Endod J 2019 9(2):144-47. [Google Scholar]
[14]. Ghiasi J, Javidi M, Farhangnia A, Shayan E, Mandibular second premolar with four canalsJournal of Dental Materials and Techniques 2015 4(3):133-36. [Google Scholar]
[15]. Vertucci FJ, Root canal anatomy of the human permanent teethOral Surg, Oral Med, Oral Pathol 1984 58:589-99.10.1016/0030-4220(84)90085-9 [Google Scholar] [CrossRef]
[16]. Sert S, Bayirli GS, Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish populationJ Endod 2004 30:391-98.10.1097/00004770-200406000-0000415167464 [Google Scholar] [CrossRef] [PubMed]
[17]. Akyuz SN, Erdemir A, Mandibular second premolar with four rootsEur J Gen Dent 2012 1(1):54-57.10.4103/2278-9626.101361 [Google Scholar] [CrossRef]
[18]. Mittal S, Kumar T, Mittal S, Sharma J, Mandibular premolars with aberrant canal morphology: An endodontic challengeJ Conserv Dent 2014 17(5):491-94.10.4103/0972-0707.13985125298656 [Google Scholar] [CrossRef] [PubMed]