Nd:YAG Capsulotomy Induced Pupillary Block Glaucoma- A Rare Case Report
K Stephen Sudhakar1, G Premnath2, KR Vignitha3, Minnu Lekshmi4, DP Shinisha5
1 Professor and Head, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
2 Associate Professor, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
3 Postgraduate, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
4 Postgraduate, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
5 Assistant Professor, Department of Ophthalmology, Chettinad Academy of Research and Education, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: G Premnath, Associate Professor, Department of Ophthalmology, Chettinad Academy of Research and Education, Kelambakkam, Chennai-603103, Tamil Nadu, India.
E-mail: drpremn18@yahoo.co.in
A 70-year-old female reported with complaints of defective vision in both eyes. Ophthalmological examination of both eyes revealed well-centred Posterior Chamber Intraocular Lens (PCIOL), thin membranous Posterior Capsular Opacification (PCO) with no signs of inflammation, myopic fundus and normal Intraocular Pressure (IOP). She had history of uneventful cataract surgery in both eyes four years back and was on treatment for diabetes mellitus and chronic obstructive pulmonary disease. PCO was managed with Nd: YAG capsulotomy in both eyes. After ten hours, patient reported back with severe headache, right-sided periorbital pain and profound diminution of vision. Examination revealed corneal oedema, shallow Anterior Chamber (AC) and raised IOP in her right eye. Patient was admitted and treated with parenteral and local IOP lowering agents and cycloplegic agents. Once the IOP was lowered and cornea cleared, slit lamp examination revealed vitreous blocking the pupil resulting in secondary angle closure which was confirmed by Anterior Segment Optical Coherence Tomography (AS-OCT). Nd:YAG LASER peripheral iridotomy was done to relieve the pupillary block. This is presented as a rare case of pupillary block following Nd:YAG capsulotomy in the presence of well-centred PCIOL.
Intraocular pressure, Posterior chamber intraocular lens, Pupillary block
Case Report
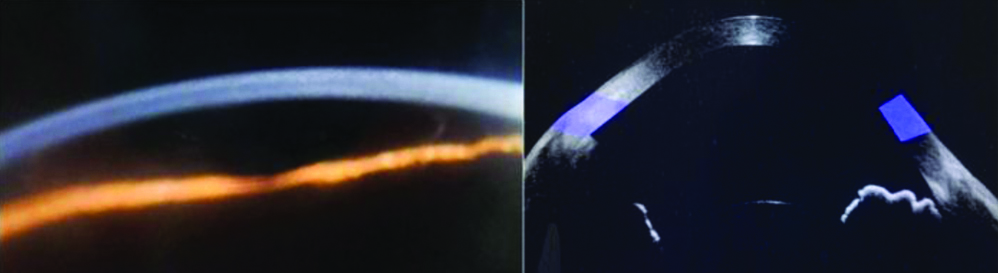
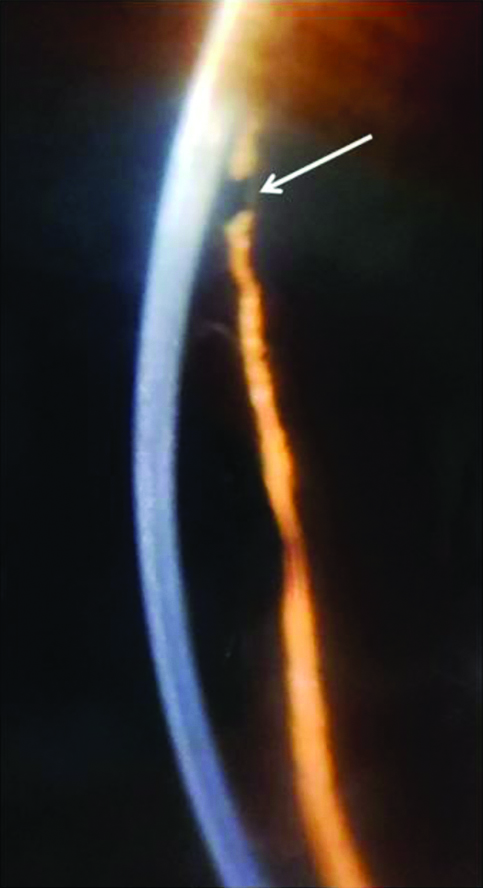
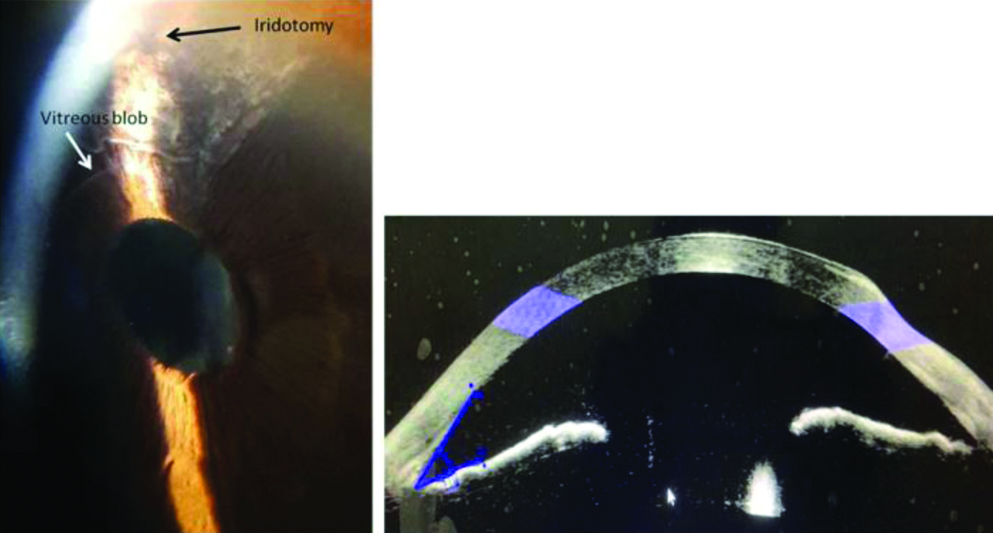
A 70-year-old female patient reported at ophthalmology clinic with complaint of defective vision in both eyes. She had history of uneventful cataract surgery four years back elsewhere and was on treatment for diabetes mellitus and chronic obstructive pulmonary disease. On examination, her Best Corrected Visual Acuity (BCVA) was 6/12 in both eyes. Anterior segment revealed quiet eyes, pseudophakia with thin membranous PCO and posterior segment revealed myopic fundus in both eyes. IOP was normal in both eyes. As the PCO was visually significant, Nd: YAG capsulotomy was done in both eyes after obtaining the informed consent. Four shots with 2.3 milliojoules (mJ) energy were used to create a 4.5 mm sized central posterior capsular opening. Energy was titrated starting from 0.5 mJ. IOP measured after the successful procedure was found to be within normal limits. Ten hours post procedure, patient complained of severe headache and pain around her right eye with decreased vision. Vision in right had reduced to hand movements and left eye improved to 6/9. Examination of right eye revealed corneal oedema, shallow AC and IOP of 58 mm Hg and left eye revealed clear cornea, deep AC and normal IOP. Patient was diagnosed to have either acute angle closure or malignant glaucoma and was treated with intravenous injection of 20% mannitol at 1 mg/kg dose, oral acetazolamide 250 mg four times a day and topical IOP lowering agents and cycloplegic agents. Once the IOP lowered and cornea cleared, slit lamp examination revealed vitreous blocking the pupil resulting in secondary angle closure which was confirmed by AS-OCT [Table/Fig-1]. Nd:YAG LASER peripheral iridotomy was done which promptly relieved the angle closure [Table/Fig-2]. Post-iridotomy, the patient recovered well. At four weeks follow-up the BCVA in the right eye was 6/9 with deep AC and 15 mm Hg IOP. AS OCT confirmed deep AC and no vitreous touch to the corneal endothelium [Table/Fig-3].
Pupillary block with angle closure ten hours post capsulotomy-Iris bombe and shallow AC.
Pupillary block relieved Post-iridotomy. White arrow shows patent iridotomy hole.
Four weeks Post-iridotomy, deep AC and vitreous in AC AS OCT- Deep AC and no vitreous touch.
Discussion
Nd:YAG LASER is known to disrupt the anterior vitreous face during capsulotomy [1]. Anterior vitreous face is damaged in around 20% of cases which had undergone capsulotomy [2]. But a well-placed PCIOL would prevent the vitreous prolapse. Though there were instances where vitreous had prolapsed into AC in eyes without implants and in eyes with AC intraocular lens or subluxated lenses the occurrence of pupillary block in cases with well-centred PCIOL is rare [3-6]. In the present case, in spite of presence of a well-centred PCIOL, vitreous prolapsed into the AC and blocked the pupil resulting in secondary angle closure which is a rare complication. The occurrence could be due to degenerated vitreous of a myopic eye.
Probably, the first case of pupillary block following capsulotomy with PCIOL was reported more than 35 years back and the second case reported in 2004 resulted in corneal decompensation which required corneal transplant [7,8]. In the present case, the clinical signs were picked up promptly and the treatment was directed towards the aetiology. Timely management averted further complications.
To the best of our knowledge there are only three cases reported worldwide and none reported in this part of the world (PubMed search). This case shows the importance of anticipating pupillary block after Nd:YAG capsulotomy even in a case with well-centred PCIOL though it is a rare occurrence [7-9].
Conclusion(s)
Pupillary block glaucoma after Nd:YAG capsulotomy in a case of PCIOL is very rare owing to the barrier effects of PCIOL and integrity of anterior vitreous face. Nevertheless, the rare complication must be anticipated in such cases to avert more serious complication.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 14, 2020
Manual Googling: May 19, 2020
iThenticate Software: Oct 27, 2020 (10%)
[1]. Özyol P, Özyol E, Evaluation of barriers between anterior and posterior compartments during Nd:YAG capsulotomy in diabetic patientsClin Ophthalmol 2014 8:483-84.10.2147/OPTH.S6121624627623 [Google Scholar] [CrossRef] [PubMed]
[2]. Ozyol E, Ozyol P, Doğanay Erdoğan B, Onen M, The role of anterior hyaloid face integrity on retinal complications during Nd: YAG laser capsulotomyGraefes Arch Clin Exp Ophthalmol 2014 252(1):71-75.10.1007/s00417-013-2526-x24257893 [Google Scholar] [CrossRef] [PubMed]
[3]. Terry AC, Stark WJ, Maumenee AE, Fagadau W, Neodymium-YAG laser for posterior capsulotomyAm J Ophthalmol 1983 96(6):716-20.10.1016/S0002-9394(14)71912-9 [Google Scholar] [CrossRef]
[4]. Goudie C, Tatham A, Advanced glaucoma following Nd:YAG capsulotomy: A case reportBMC Ophthalmol 2018 18(Suppl 1):22910.1186/s12886-018-0852-930255795 [Google Scholar] [CrossRef] [PubMed]
[5]. Gstalder RJ, Pupillary block with anterior chamber lens following Nd:YAG laser capsulotomyOphthalmic Surg 1986 17(4):249-50.10.3928/1542-8877-19860401-123714195 [Google Scholar] [CrossRef] [PubMed]
[6]. Kersey JP, McMullan TF, Broadway DC, Pupil block glaucoma after neodymium: YAG capsulotomy in a patient with a partially subluxated posterior chamber intraocular lensJ Cataract Refract Surg 2005 31(7):1452-53.10.1016/j.jcrs.2004.11.05816105624 [Google Scholar] [CrossRef] [PubMed]
[7]. Ruderman JM, Mitchell PG, Kraff M, Pupillary block following Nd:YAG laser capsulotomyOphthalmic Surg 1983 14(5):418-19.10.3928/1542-8877-19830501-076877743 [Google Scholar] [CrossRef] [PubMed]
[8]. Mihora LD, Bowers PJ Jr, Blank NM, Acute angle-closure glaucoma caused by vitreous prolapse after neodymium: YAG posterior capsulotomyJ Cataract Refract Surg 2004 30(11):2445-47.10.1016/j.jcrs.2004.04.05915519106 [Google Scholar] [CrossRef] [PubMed]
[9]. Li EY, Wu WK, Jhanji V, Pupillary block glaucoma secondary to vitreous prolapse after Nd:YAG capsulotomyClin Exp Optom 2011 94:383-84.10.1111/j.1444-0938.2010.00577.x21599749 [Google Scholar] [CrossRef] [PubMed]