Endoscopic Removal of a Migrated Fragment of Wire used for Intermaxillary Fixation in Surgical Treatment of Mandibular Fracture
Toshinori Iwai1, Satomi Sugiyama2, Toshiyuki Koizumi3, Makoto Hirota4, Kenji Mitsudo5
1 Assistant Professor, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
2 Clinical Fellow, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
3 Assistant Professor, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
4 Associate Professor, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
5 Professor, Department of Oral and Maxillofacial Surgery/Orthodontics, Yokohama City University Hospital, Yokohama, Kanagawa, Japan.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Toshinori Iwai, 3-9 Fukuura Kanazawa-ku, Yokohama, Kanagawa, Japan.
E-mail: iwai104oams@yahoo.co.jp
Endoscope, Foreign body, Mandible
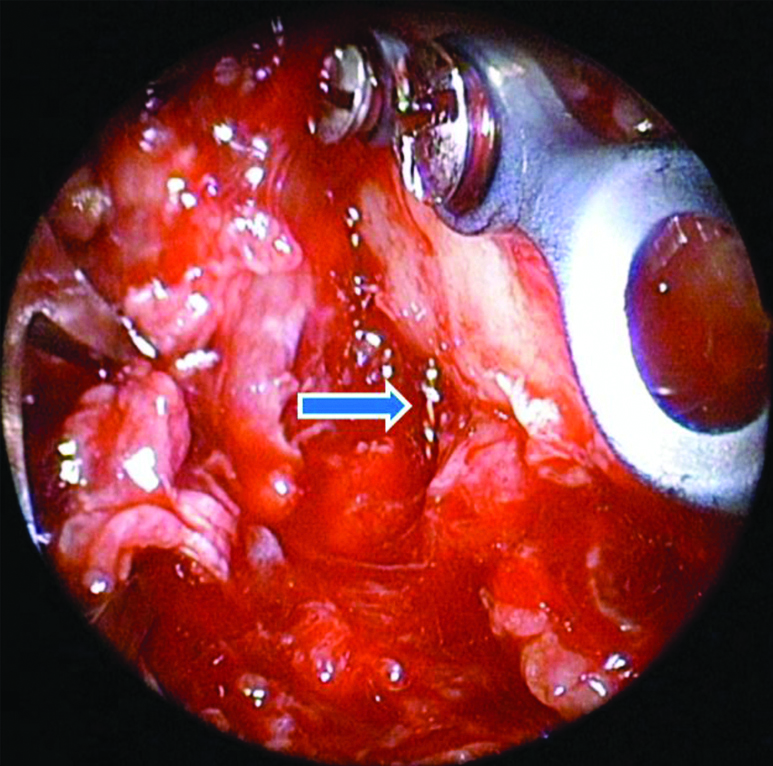
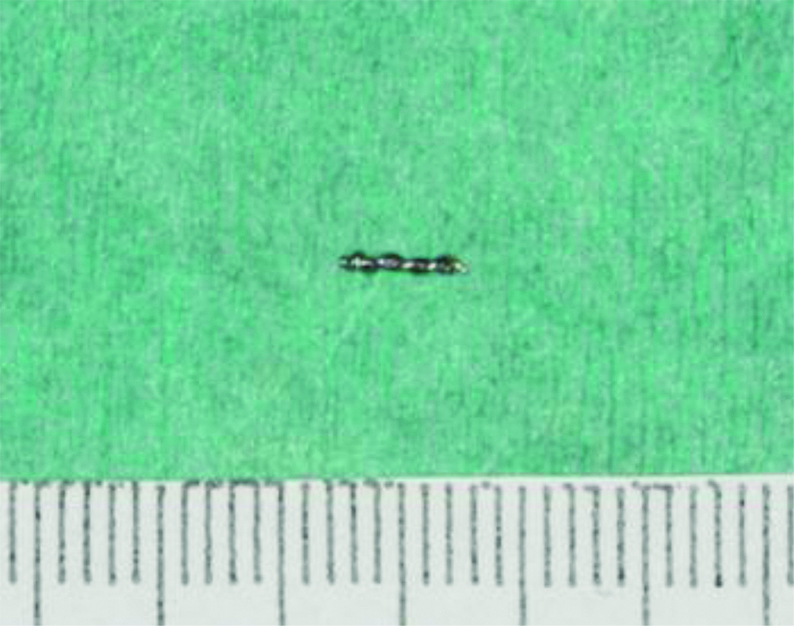
A 63-year-old woman fell and hit the right side of the mandible directly on the floor, and visited our department with right side of the lower jaw pain and intraoral bleeding as the chief complaint. She also had trismus. She had no present and past significant medical and dental histories. Intraoral examination showed malocclusion (imperfect positioning of the teeth when the jaws are closed) and intraoral bleeding from the fractured site. Panoramic radiograph showed fracture of the right posterior body of the mandible and the root fracture of the right second molar. Therefore, she underwent open reduction and internal fixation of the mandibular fracture under general anaesthesia. An intraoral incision was made along the ascending ramus and cervical gingiva of the mandibular right second molar and vertical gingival incision was made at the mesial aspect of the mandibular right second molar. The second molar was removed after the flap elevation, and six 2.0 mm diameter intermaxillary fixation screws (Dual-Top Auto Screw II®, Jeil Medical Corporation, Seoul, Korea) were used for intraoperative intermaxillary fixation. After the bone reduction and intermaxillary fixation with wires, two plates fixation was performed with 2.0 mm fixation system (Universal Mandible®, Stryker, Tuttlingen, Germany). The 0.3 mm diameter steel wires were cut and removed, and the wound was closed with resorbable suture (VICRYL®). Surgical time was 172 min. The next day, panoramic radiograph and computed tomography revealed a wire fragment below the right inferior border of the mandible [Table/Fig-1]. Therefore, she underwent removal of the wire fragment under general anaesthesia. Because the wire fragment was small (6 mm length), the removal was performed using a 30-degree, 4-mm-diameter endoscope with tissue retractor (Karl Storz, Tuttlingen, Germany) [Table/Fig-2]. An intraoral incision was made along the ascending ramus and cervical gingiva of the mandibular right second molar and vertical gingival incision was made at the mesial aspect of the mandibular right second molar. This incision was opened during second surgery by suture removal. The sutures were removed and intraoral wound was opened. After the retractor was inserted into the wound, the endoscope was inserted intraorally and blindly in the surgical space, and additional space-making was performed by the tissue retractor of the endoscope. The small wire fragment was identified on the lateral side of the right inferior border under endoscopic guidance [Table/Fig-3], and removed completely using a long mosquito forceps (FOUR MEDICS, Tokyo, Japan) without the use of 3D C-arm prepared [Table/Fig-4]. The wound was closed with resorbable suture (VICRYL®). Furthermore, refixation of plates was performed due to insufficient plate fixation in the initial surgery. Panoramic radiograph after second surgery showed no wire fragment [Table/Fig-5]. The patient was discharged 7 days after first surgery.
Panoramic radiograph and Computed Tomography (CT) show a wire fragment (arrow) below the right inferior border of the mandible. a) Panoramic radiograph; b) Axial CT image; c) Coronal CT image.

A 30-degree, 4-mm-diameter endoscope with tissue retractor.

Endoscopic view. Arrow indicates a wire fragment on the lateral side of the inferior border of the mandible.
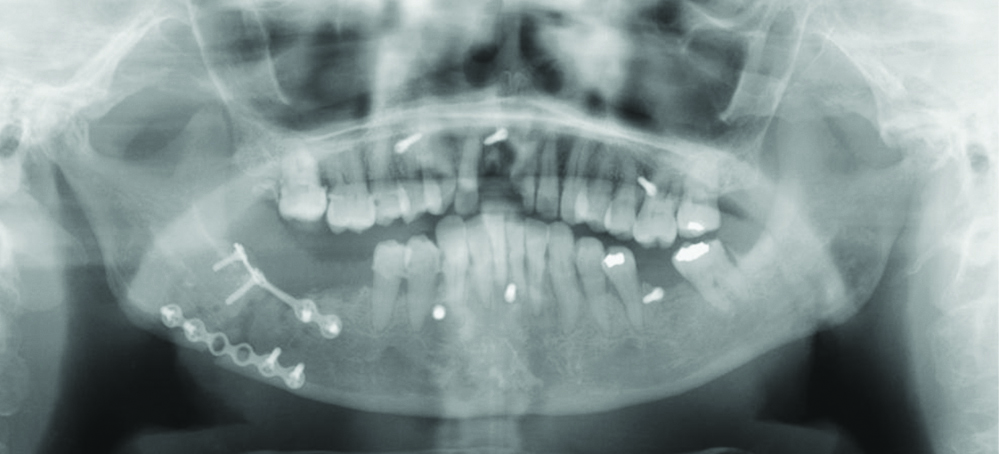
Postoperative panoramic radiograph showing absence of wire fragment.
Foreign bodies are sometimes migrated in the tissues in head and neck by trauma [1-3], but iatrogenic foreign bodies, such as broken needles or instruments, teeth, roots, and dental implants are also reported [4-8]. Foreign body removal is challenging for the complexity of the approach and the proximity to vital anatomical structures such as nerves and vessels [3], and blind exploration is often time-consuming and sometimes futile [4]. Therefore, preoperative localisation and intraoperative identification of foreign bodies are required.
Foreign bodies retained in the head and neck region may cause complications including infection such as sinusitis or meningitis, pain, fistula, metal relevant poisoning, or cancer [1].
Several methods have been used to detect and localise foreign bodies, such as radiograph, computed tomography, magnetic resonance imaging, ultrasonography [4], C-arm fluoroscopy [4-6], navigation system [1,2,4,7], endoscope [1-3,8]. Preoperative imaging methods cannot allow intraoperative identification of foreign bodies. Intraoperative ultrasonography cannot show foreign bodies migrated in deep tissues. Navigation systems help identify the location of foreign bodies three-dimensionally and intraoperatively, but the intraoperative displacement of foreign bodies migrated in the soft tissues makes the identification difficult. Although C-arm fluoroscopy has radiation exposure, it can provide real-time two-dimensional image. Especially, 3D C-arm allows not only planar images but also 3D images as CT. Because endoscope can provide good illumination, clear and magnified visualisation of the surgical field, it is used for removal of foreign body in deep regions, such as condylar process [3] and maxillary sinus [8]. Although the intraoral approach without a visible scar and facial nerve injury has restricted surgical field and difficult access, even small foreign bodies can be identified under endoscopic guidance. In the present case, a small wire fragment retained on the lateral side of the right inferior border, could be successfully removed under magnified view of the endoscope, without the use of 3D C-arm.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? NA
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 23, 2020
Manual Googling: Sep 05, 2020
iThenticate Software: Oct 15, 2020 (8%)
[1]. Liu Z, Lin Y, Zhang L, Yang C, Shen SG, Wang X, Endoscopic-assisted navigation-guided removal of long-standing metallic foreign body near to the sphenoidJ Craniofac Surg 2015 26(2):e122-24.10.1097/SCS.000000000000134525710741 [Google Scholar] [CrossRef] [PubMed]
[2]. Xing L, Duan Y, Zhu F, Shen M, Jia T, Liu L, Computed tomography navigation combined with endoscope guidance for the removal of projectiles in the maxillofacial area: A study of 24 patientsInt J Oral Maxillofac Surg 2015 44(3):322-28.10.1016/j.ijom.2014.12.01825601155 [Google Scholar] [CrossRef] [PubMed]
[3]. Suarez-Cunqueiro MM, Schon R, Gellrich NC, Schmelzeisen R, Endoscopic assistance in the removal of a foreign body in the condylar processJ Craniofac Surg 2004 15(1):98-101.10.1097/00001665-200401000-0002714704573 [Google Scholar] [CrossRef] [PubMed]
[4]. Holmes PJ, Miller JR, Gutta R, Louis PJ, Intraoperative imaging techniques: A guide to retrieval of foreign bodiesOral Surg Oral Med Oral Pathol Oral Radiol Endod 2005 100(5):614-18.10.1016/j.tripleo.2005.02.07216243249 [Google Scholar] [CrossRef] [PubMed]
[5]. Pandyan D, Nandakumar N, Qayyumi BN, Kumar S, C-arm fluoroscopy: A reliable modality for retrieval of foreign bodies in the maxillofacial regionJ Contemp Dent Pract 2013 14(6):1193-96.10.5005/jp-journals-10024-147524858775 [Google Scholar] [CrossRef] [PubMed]
[6]. Park SS, Yang HJ, Lee UL, Kwon MS, Kim MJ, Lee JH, The clinical application of the dental mini C-arm for the removal of broken instruments in soft and hard tissue in the oral and maxillofacial areaJ Craniomaxillofac Surg 2012 40(7):572-78.10.1016/j.jcms.2011.10.01322078499 [Google Scholar] [CrossRef] [PubMed]
[7]. Li P, Li Z, Tian W, Tang W, A strategy for removal of foreign body in mandible with navigation systemInt J Oral Maxillofac Surg 2015 44(7):885-88.10.1016/j.ijom.2015.01.02125744644 [Google Scholar] [CrossRef] [PubMed]
[8]. Gao QM, Yang C, Zheng LY, Hu YK, Removal of long-term broken roots displaced into the maxillary sinus by endoscopic assistantJ Craniofac Surg 2016 27(1):e77-80.10.1097/SCS.000000000000223526703040 [Google Scholar] [CrossRef] [PubMed]