Introduction
STH constitute the most common parasitic (worm) infections worldwide. The transmission route is feco-oral, primarily due to soil-contamination by eggs present in human faeces [1]. The most important STH are roundworms (Ascaris lumbricoides), whipworms (Trichuris trichura) and hookworms (Necator americanus or Ancyclostoma duodenale) [1].
Globally, around 1.5 billion people (or 24% of world’s population) are infected with STH, with highest cases in the tropical and sub-tropical regions [1]. For India, high STH prevalence among School-Age Children (SAC) has been documented across 6 States [2,3]. However, the data is considerably heterogenous, probably due to varying climatic conditions, demographics and sociocultural practices of the population. For instance, STH prevalence has been found to be relatively higher in rural India compared to urban areas [4,5].
Undoubtedly, STH control has now become a public health priority globally. Studies show that for robust STH control, adopting measures like PC, improvement in sanitation, clean drinking water, use of pit-latrines and good hygiene practices will be crucial [5-7]. Currently, the WHO strategic plan (2011-2020) recommends similar measures for ‘at-risk’ populations residing in STH endemic areas [8]. Over the years, India has also ramped-up STH control measures through several innovative programmes [9], including National Deworming Day, Swachh Bharat Abhiyan, Nirmal Gram Puraskar, Water Sanitation and Hygiene (WASH) interventions, Clean India: Clean schools, etc. In this paper, authors relooked at such initiatives that have positively impacted STH burden trends and public health in India. Using keywords and Boolean operators, authors have searched electronic databases (Pubmed, IndMed, PsychInfo, Science-Direct and Google Scholar) and grey literature to identify recent articles on STH control in India. A formal review/meta-analysis was not conducted; authors present the findings in the form of succint description of literature according to the identified theme- challenges and opportunities in STH control in India.
STH Control Strategies in India
According to WHO, India has nearly 241 million children between ages 1 and 14 (68% of SAC) constituting ‘at-risk’ category for STH infections. This represents approximately 28% of the global burden [2]. Multiple surveys conducted over the years indicate infection with more than one STH species [10-16]. For instance, Greenland K et al., in a cross-sectional survey (using stool-sample) among children in 20 schools across Bihar reported STH prevalence of 68% (10-86% across schools). The prevalence of ascariasis, hookworm and trichuriasis was 52%, 42% and 5%, respectively [10]. Ganguly S et al., reported overall weighted STH prevalence of 75.6% across 130 primary schools in 9-agro climatic zones in Uttar Pradesh [11]. Kaliappan SP et al., in their cross-sectional study with one-stage cluster sampling of 22 clusters (n=1237) in Tamil Nadu, reported overall STH prevalence of 39%, with hookworm 38% and Ascaris lumbricoides 1.5% [15]. There has also been an increase in morbidity statistics not only for India, but globally as measured by Disability-Adjusted Life Years (DALY) [17]. Moreover, while the impact of hookworm infection appears to disproportionately affect SAC, studies show that women in child-bearing age group, pregnant women and even adults seem to be at high risk of STH-related morbidity [5,6,8,17-20].
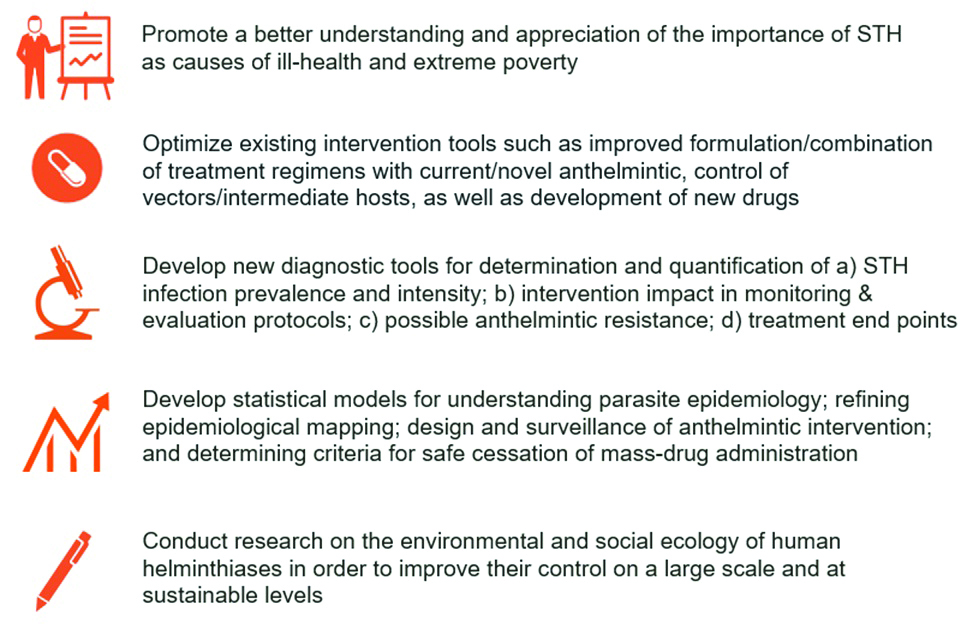
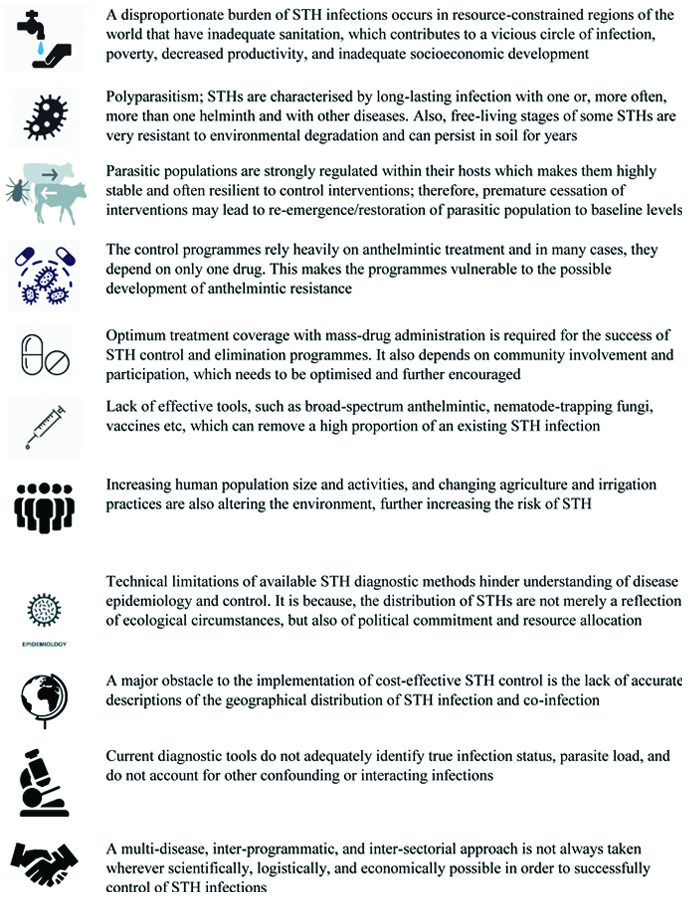
Overall, effective STH control will require identifying major gaps that impede sustained control and elimination measures [Table/Fig-1] [21]. This is because, apart from sanitation, several other factors are known to drive the persistence and re-emergence of STH infections in humans [Table/Fig-2] [21]. In this regard, having expanded health programmes which promote healthy behaviour modifications apart from benefits of deworming and good WASH practices was essential. Such efforts would have required mobilisation of consequential human and financial resources. Of late, India has prioritised its health resource to introduce several novel solutions for STH control [Table/Fig-3] [9,22-28].
Gaps that hinder sustainability of STH control and elimination measures [21].
This figure has been independently created by GSK for illustration purposes only; Figure adapted from Lustigman S, Prichard RK, Gazzinelli A, Grant WN, Boatin BA, McCarthy JS, et al. A research agenda for helminth diseases of humans: the problem of helminthiases. PLoS Negl Trop Dis. 2012;6(4):e1582. [Reference 21]
Factors driving the persistence and re-emergence of STH infections [21].
The list is not exhaustive; created independently by GSK for illustration purposes only; Figure adapted from Lustigman S, Prichard RK, Gazzinelli A, Grant WN, Boatin BA, McCarthy JS, et al. A research agenda for helminth diseases of humans: the problem of helminthiases. PLoS Negl Trop Dis. 2012;6:e1582. [Reference 21]
Major initiatives contributing to STH control and elimination in India [9,22-28].
| Timeline | Description | Reference |
|---|
| 1954 | First formal sanitation programme launched as a part of the First Five Year Plan of the Government of India | [9,22] |
| 1963 | National Centre for Disease Control (NCDC) starts conducting STH surveys in different parts India | [9,22] |
| 1986 | Launch of Central Rural Sanitation Programme primarily with the objective of improving the quality of life of the rural people and to provide privacy and dignity to women | [9,23] |
| 1996 | Launch of Total Sanitation Programme; a “demand driven” approach emphasised more on information, education and communication, human resource development, capacity development activities to increase awareness among the rural people and generation of demand for sanitary facilities | [9,23,24] |
| 1999 | NCDC adopts WHO sampling methodologies and Kato-Katz technique for stool sample examination and STH surveys conducted in different ecological zones in India | [9,22] |
| 2002 | Launch of Swajaldhara, a national level program to change the way in which water and sanitation services are supported in rural areas, by decentralizing service delivery responsibility to rural local governments and user groups | [22,25] |
| 2003 | Launch of Nirmal Gram Puraskar to give a fillip to Total Sanitation Campaign (first awards given in 2005) | [26] |
| 2008 | Launch of National Urban Sanitation Policy (NUSP) by the Ministry of Urban Development (MoUD), emphasising the need of defining integrated city/state-wide sanitation plans | [9,24] |
| 2010 | Launch of national level reward scheme (under MoUD) for ranked cities achieving measurable milestones in becoming sanitised, livable Nirmal Shahars. The rankings are based on 19 sanitation parameters, on the basis of which cities were assigned either of four colour code rating; ‘red category’ (in need of immediate remedial action, score < 33), ‘black category’ (needing considerable improvement, score 34-66), ‘blue category’ (recovering, score 67-90) and ‘green category’ (healthy clean city, score 91-100). | [24,25,26] |
| 2012 | Launch of Nirmal Bharat Abhiyan (later restructured as Swachh Bharat Abhiyan). Its main objective was to accelerate the sanitation coverage in the rural areas to comprehensively cover the rural community through renewed strategies and saturation approach. | [25] |
| 2014 | Launch of Swachh Bharat Mission (SBM) or Swachh Bharat Abhiyan (SBA) or Clean India Mission to eliminate open defecation (by 2019) and improve Solid Waste Management (SWM) in urban and rural areas in India. The mission was split into two: rural (SBM Gramin) and urban (SBM Urban). | [25] |
| Launch of Swachh Vidyalaya or “Clean India: Clean Schools” with primary goal is to make a visible impact on children’s health and hygiene through improving both their health and hygiene practices and those of their families and communities | [27] |
| 2015 | The first round of National Deworming Day conducted in February 2015 | [28] |
| NCDC undertakes countrywide mapping of the STH prevalence and intensity | [9, 22] |
| 2018 | Launch of Swajal project (under the National Rural Drinking Water Programme), designed as a demand driven and community centered program to provide sustainable access to drinking water to people in rural areas. It was initiate as a pilot scheme in six states of Bihar, Madhya Pradesh, Maharashtra, Rajasthan, Uttar Pradesh and Uttarakhand. | [22-25] |
*The above list is not exhaustive
National Deworming Day
The WHO ‘2020 Roadmap on Neglected Tropical Diseases (NTD)’ (released 2012) emphasised targeted deworming programmes aimed at ‘at-risk’ populations including children (age ≥1 year), non-pregnant adolescent females (age 10-19 years), non-pregnant women of the reproductive age-group (age 15-49 years) and pregnant women (second and third trimester) to control morbidity associated with STH. In areas where the baseline prevalence of any STHs >20%, the recommendation is an annual dose of albendazole (400 mg; 200 mg for children age 1-2 years) or mebendazole (500 mg). In areas with baseline STH prevalence >50%, the recommendations is biannual deworming. In addition, if the STH prevalence of anaemia >40% among pregnant women, deworming is conditionally recommended [8]. The overall objective is to ensure 75% of Pre-SAC (PSAC) and SAC in need of treatment are regularly treated, by targeting 75% PC coverage in 100% countries by 2020 [8].
India launched its first ‘National Deworming Day’ (NDD) on February 10, 2015. The exercise, one of the largest in the world, included massive school-based deworming effort across twelve States to treat all children ‘at-risk’ for STH [28]. The NDD was followed by a Mop-Up Day (MUD) on February 13, 2015 with the intent of deworming children who missed the dose on February 10, 2015 [28]. The main objective of NDD is to deworm all PSAC/SAC (enrolled and non-enrolled) between the ages of 1-19 years biannually through the platform of local schools and Anganwadi centres. This would ensure improvement in overall health, nutritional status, access to education and quality of life for these children [28,29].
After the first round of NDD (2015), nearly 8.9 crore SAC were administered deworming tablet across 12 States/Union territories (Assam, Bihar, Chhattisgarh, Delhi, Dadra and Nagar Haveli, Haryana, Karnataka, Maharashtra, Madhya Pradesh, Rajasthan, Tamil Nadu and Tripura) achieving approximately 85% national coverage [28]. Over the next two years (2016-17), the outreach expanded the coverage 88% against the initial set targets of NDD. Approximately 26.68 crore children have been administered Albendazole (400 mg and 200 mg for children age between 1-2 years and 2-19 years, respectively) till February 2018, and more than 114 crore doses of Albendazole were administered to children between ages 1 and 19 years, since 2015 [28]. Both Albendazole and Mebendazole (500 mg) are WHO recommended drugs; are safe, effective, inexpensive and easy to administer by even non-medical personnel (e.g., teachers) [8]. Both drugs are donated to national ministries of health through WHO in all endemic countries for STH treatment of all PSAC and SAC. Ivermectin use against S. stercoralis is expected to be available at affordable price from 2021 [8].
Swachh Bharat Mission (SBM)
To adhere to United Nations Sustainable Development Goal 6 (SDG 6) [30], and to expand the public health needs, in 2014, India launched a fully funded national hygiene, sanitation and waste management campaign called Swachh Bharat Mission to eliminate open defecation and improve SWM in the country [25]. The transition of a Swachh Bharat to a healthier India has also been advocated by numerous public figures.
The strategy is to move towards a ‘Swachh Bharat’ i.e., Clean India by making it a massive mass movement (‘Jan Andolan’) that seeks to engage everyone in the task of cleaning his/her living area and surroundings in a collective quest. The mission was split into two; in rural areas (SBM- Gramin, under Ministry of Drinking Water and Sanitation) and urban areas (SBM- urban, under Ministry of Housing and Urban Affairs) [25]. Also, volunteers known as Swachhchagrahis or ‘Ambassadors of cleanliness’, was trained to promote indoor plumbing and community approaches to sanitation at village level.
The relationship between cleanliness and better health has been propagated since the inception of the Swachh Bharat Abhiyan. As on date, the progress reported for rural sanitation coverage is 98.8%; 92 million toilets have been constructed, and 604 districts have been declared with ‘Open Defecation Free’ (ODF) status [25]. With respect to urban sanitation, 5.4 million individual household toilets, community, and public toilets have been constructed. Approximately, 3461 cities/town were declared with ODF status in 2019 [25].
The states of Chhattisgarh, Jharkhand, Madhya Pradesh and Rajasthan have already reported stark change in their sanitation coverage ≥80%. In the latest Swachh Survekshan Survey 2019, Indore was adjudged as the cleanest city, while Chhattisgarh was the cleanest state in India [25]. Additionally, in the two years since Swachh Bharat Abhiyan was launched, the deaths due to unsafe water and sanitation as percentage of total deaths across the country were reportedly reduced to 5% in 2016 (compared to 13% in 1996) [25]. Child diarrhoea deaths in India were also reported to decrease by 12.7% in 2016 i.e., from 1,21,889 cases in 2014 to 1,02,813 cases in 2016 [25]. The percentage of under-five children dying from diarrhoea came down from 13% to 9% [25].
National Urban Sanitisation Policy
The 2001 Census reflected the need for healthier urban living, which would mean healthier sanitation and waste disposal practises [2,23]. To this effect, in November 2008, India launched the ‘National Urban Sanitation Policy’ (NUSP) with the objective of creating ‘totally sanitised cities’ that are ODF, safely collect and treat all their waste water, eliminate manual scavenging and dispose solid waste safely [24]. By 2010, nearly 12 States had completed drafting state sanitation strategies based on the policy. Currently, additional 120 cities/town have completed or are in the process of preparing city sanitisation plans [24].
The Ministry of Urban Development (MoUD) has also introduced a national level reward scheme (Nirmal Shahar Puraskar) based on its survey of cities/states that achieve measurable milestones in becoming sanitised, livable Nirmal Shahars (exemplary city) [9,23,24]. Each year if the city improves its ratings, specifically on achieving ‘green category’ status, cities are typically invited for the national award. The rankings are based on 19 sanitation parameters such as access to community toilets, safe management of human excreta, SWM etc. Four colour codes have been assigned to the cities based on the points they obtained in the rating; ‘red category’ (in need of immediate remedial action, score < 33), ‘black category’ (needing considerable improvement, score 34-66), ‘blue category’ (recovering, score 67-90) and ‘green category’ (healthy clean city, score 91-100). Currently, three cities are found to be in the category of “recovering” in terms of sanitation facilities, including Chandigarh (73.480), Mysore (70.650), Surat (69.080), and the New Delhi Municipal Corporation administered area (68.265) [23,24].
The MoUD survey rating serves as a baseline to measure improvements in the future and to prioritise actions. Such ratings also support implementation of the NUSP, to create healthy competition among cities as each strives to earn the glory of being a Nirmal Shahar, that will determine its sanitation and healthy living status [23,24].
Total Sanitation Campaign
In 1999, India had initiated a demand-driven, public sanitation programme under ‘Total Sanitation Campaign’ (TSC), resembling ‘Community-led Total Sanitation’ (CLTS) with subtle differences viz., while CLTS focused more on preventing open defecation through self-awareness and shame, TSC focused more on building sanitation infrastructure. The main goal of TSC was to eradicate the practise of open defecation by 2017 [23,24]. It was modelled on the 1986 ‘Central Rural Sanitation Programme’ (CRSP), one of the first programmes to provide financial assistance to below poverty level families for constructing individual household toilets [23,24]. Under the CRSP scheme, the Union government contribution was 60% cost, the State government was 20% and the rest was to be borne by the household for cost up to INR 1500. The programme also noted the importance of sanitary complexes for community spaces and provisioned an amount of up to Rs. 2 lacs for construction of such facilities [23,24].
The uniqueness of TSC was its adherence to ‘demand-driven’ approach, that paid emphasis on information, awareness/capacity building activities, education and communication, human resource development and demand generation for sanitary facilities [9,23,24]. As a result, by December 2017, total sanitation coverage throughout India had improved to 73% (compared to 42% on October 2, 2014, the day Swachh Bharat Abhiyan was launched) [25].
Moreover, as an encouragement to this endeavour, Nirmal Gram Puraskar (NGP) aka Clean Village Award was launched in 2003, to recognise the efforts in terms of monetary awards for those who have contributed significantly in ensuring full sanitation in their area of operation. The project is being implemented in rural areas taking district as a unit of implementation [26]. As on December 2013, 28002 Gram Panchayats have been awarded the NGP. An independent National level study was conducted by the Ministry of Drinking Water and Sanitation, Govt. of India in 2010 for impact assessment of NGP. The study covered 664 Gram Panchayats awarded NGP in 12 States. Main findings of the study included: 19.1% surveyed households reported limited of access to any type of sanitation facility, 67% surveyed households reported all members using the latrine regularly, and 91% of the schools and 71% of the Anganwadis had sanitation facilities [26].
WASH Interventions
The term ‘WASH’ expands into ‘wash, sanitation and hygiene’, denoting SDG 6 public health provisions that must be available universally, in an affordable and sustainable way [30,31]. Several studies from India have shown that attention to WASH can improve health, life expectancy, student learning, gender equality and other important issues of international development [31-33]. The data also informed several policy decisions, including provision of ‘flush-pit latrines’ and community mobilisation in village populations where parasitological measures of STH were recorded [32,33].
Apart from Swachh Bharat Abhiyan, another key campaign in driving WASH strategy is Swachh Bharat, Swachh Vidyalaya aka ‘Clean India: Clean Schools’, initiated on September 24, 2014 [27]. The main feature of the campaign is to ensure that every school in India has a set of functioning and well-maintained WASH facilities and must incorporate human development components that help to prevent WASH related disease [27]. In other words, every school in India must have six essential requirements in their school WASH programme:
Gender segregated toilets having soap/washing facilities and private cleaning/disposal facilities for menstrual waste.
Adequate group handwashing facilities which allows groups of students (10-12) to wash their hands at the same time.
Apart from daily access to safe drinking water, water for handwashing, school-cleaning, food preparation/cooking, appropriate handling and storage of drinking water should be practiced throughout the school.
WASH facilities need to be clean/sanitised and well maintained with periodic checks to ensure intended results are achieved.
WASH behaviour change communication activities should be part of the daily routine of all children.
Capacity building at various levels within the sector, to develop the right mix of skills, knowledge and experience to facilitate, finance, manage and monitor WASH programmes in schools effectively [27].
Apart from STH control, several benefits of a school-based WASH intervention have been identified. First, WASH facilities in school ensures a healthy school environment and protect children from illness and exclusion [27]. Hygiene education promotes practices that would prevent infectious diseases as well as encourage healthy behaviour in future generations of adults. Hygiene in school also supports school nutrition, as the simple act of washing hands with soap pre-‘mid-day meal’ assists to break disease transmission routes. Having gender segregated toilets and WASH facilities hugely benefits girls, who may be vulnerable to school drop-out if such facilities are unavailable or non-private. Differently-abled children are also vulnerable to school drop-out, hence effective WASH programme seeks to remove barriers by promoting inclusive design, user-friendly, child-friendly facilities that benefit all users. WASH facilities in schools also promotes equity, as children nurture their right to access to safe drinking and WASH facilities and gain benefits through the improved hygiene practices promoted in schools. Overall, having a clean school fosters a child’s pride in his or her school and community. It enables every child to become an agent of change for improving WASH practices in their families and community [27].
Best Practices, Opportunities, and Challenges for STH Control in India
Enhanced Monitoring of Programme Impact
To achieve good STH control, the WHO Roadmap set out strict targets that have been difficult for most nations to comply [34]. By far the biggest issue for India has been in identifying the patient base i.e., who needs treatment, since conducting parasitological survey is costly and time consuming. This is mainly attributed to India’s expansive geography, diverse climatic conditions and socio-political landscape [2,5]. Such diversities often have a strong influence on disease distribution; as a result, STH infections in India take varied forms, including forest versus tribal or urban versus rural disease trends, requiring adaptive surveillance and containment measures [5].
However, India has been efficient in handling mega public health issues historically, aided by some of the largest surveillance programmes in the world. In fact, its track record in handling small pox, polio and malaria has been exemplary. Sometimes, frugal yet effective initiatives, like ‘finger marking’ in polio, have proved to be a cost-effective surveillance tool; a useful measure that could be applied in the NDD programme [35].
Furthermore, India also resourced information on STH prevalence through Global Atlas Helminth Infections (GAHI), to ensure quality data and decipher regional trends [36]. The GAHI is an online open-access information source on the distribution STH, schistosomiasis and lymphatic filariasis. Based on the GAHI project data from 127 surveys implemented in India between 1999 to 2007, the national STH prevalence was estimated at 21% [36].
However, for a vast country like India, it is difficult to reliably obtain data from rural areas. To cater this, India has been investing into advanced solutions for comprehensive Monitoring and Evaluation (M&E) of STH burden. Much of its understanding was derived from Africa’s recent progress in data sharing and transparency for NTD through the work of ESPEN (Expanded Special Project for Elimination of NTDs) and their data portal [37]. The ESPEN portal is an electronic platform designed to enable health ministries and stakeholders to share and exchange sub-national programme data, in support of NTD control and elimination goals. Additionally, countries are starting to adopt high-tech methodologies like remote sensing proxy environmental data for rapid epidemiological assessment of STH prevalence among SAC [38,39]. Advanced measures like spatial analysis and risk mapping of STH infections using Bayesian geostatistical models are also underway in many countries, including India [40,41].
Identifying at-risk Groups Other than Children
Deworming of PSAC/SAC has been shown to reduce high-burden of the disease in a cost-effective manner [7]. However, for most nations, empirical evidence from both multi-year deworming programmes and modelling studies suggested that targeting SAC alone for PC is insufficient for sustained control and elimination of STH infection [42,43]. This is especially true for T. trichura (due to poor drug efficacy) and for hookworm (due to typically convex age-intensity profiles or reach a plateau in adulthood) [44,45]. Data also showed that adults could be at high risk of hookworm infection and thus contribute substantially to STH transmission [46].
Although, India’s NDD has been a testament of how large-scale PC could be benefitting, the requirement to scale-up sentinel surveillance in order to predict, detect and treat widely dispersed pockets of STH transmission is essential. However, a meticulous approach targeting ‘at-risk’ will be needed, also regarding current drug availability and added cost of this approach. Kenya’s ‘Breaking Transmission Strategy’ (2019-2023) is a similar example of large-scale national strategy for elimination of endemic Preventive Chemotherapy-NTD (PC-NTD) including STH, schistosomiasis, lymphatic filariasis and trachoma [47].
Holistic Approach Against Anti-helminthic Drug Resistance
Several reports indicate that there is variable degree of anthelmintic resistance among different species of gastrointestinal nematodes [48-50]. Overall, human populations with long history of single drug deworming in places with low STH burden, due to reach transmission peak, are likely to be at greatest risk of developing drug-resistant parasites [48-50].
Although, advancement in field-applicable diagnostics including quantitative Polymerase Chain Reaction (qPCR) that can identify and monitor signs of emerging resistance, have been crucial in STH control measures, further research is still needed [51]. In many instances, newer modalities like maintaining parasites in ‘refugia’ without exposure to anthelmintic have been tried to delay emergence of anthelmintic resistance, as susceptible genes are preserved [52]. Additionally, not relying solely on drug-based STH control schemes but employing sustainable options like parasite-resistant breeds, pasture management, nematode-trapping fungi, anti-parasitic vaccine and botanical dewormers can prove beneficial [52]. This is because; such measures reduce reliance on the use of non-environmental friendly, harmful chemicals.
Employing Validated Programme Stage-specific Diagnostics
The need for newer diagnostics that are appropriate for informing key decision points for national STH programs has been long identified [53]. The widely employed Kato-Katz technique, although inexpensive, has lower positive-predictive values in low-prevalence settings [54-56]. In addition, preliminary analysis using microscopy and/or PCR can even mis-identify hookworm infection [53,56].
In this regard, newer diagnostics have been validated including direct smear technique, formol-ether concentration technique, agar-plate culture technique, Baermann technique, Water Emergence technique for detecting strongyloides larvae in feces, Harada-Mori technique, Merthiolate-Iodine-Formaldehyde-Concentration Technique (MIFC), Flotation techniques, Stoll’s Dilution Egg-Counting technique, McMaster Method for Quantitative fecal examination and Antigen technique [56]. However, on-field tests that are highly sensitive, with quick turn-over time is the need of the hour, especially those that can be employed in settings that from STH control to elimination. Field-diagnostic and laboratory protocols need to be standardised, along with establishment of reference laboratories and training development for different contexts and languages. Identifying additional gap areas like sustaining animal models, conducting field studies to calculate test performance in various settings will be crucial follow-up activities [57].
Identifying WASH Indicator(s) to be included in STH Control Measures
The 2020 WHO roadmap identified the critical role of WASH in STH control, but did not set actionable targets [8,58] In several geographies, establishing a structure for engagement with the WASH sector has been difficult. However, the recent development of the WASH-NTD joint strategy provides an entry point and guidance for improved collaboration [58].
Recent meta-analysis demonstrates effective WASH intervention can immensely reduce STH infection and prevalence rates [59,60]. Ziegelbauer K et al., demonstrated that availability of sanitation facilities was associated with significant protection against STHs (OR 0.46 to 0.58) [59]. Strunz EC et al., concluded WASH practices are generally associated with reduced odds of STH infection by atleast 33% [60]. In most studies, apart from WASH interventions, access to water and hygiene also appears to significantly reduce odd of STH [59,60].
Apart from monitoring of WASH indicators, as part of STH control programming, mapping of certain behavioural or practise adoption (like shoe-wearing) is important especially in STH-endemic areas [61]. Additionally, identifying consistent indicators across WASH programmes (like water sources, food hygiene) can essentially reflect unmet areas and guide policy making [62].
Conclusion(s)
The current piece, although, having the limitations of a narrative review, provides a succinct understanding of various STH control strategies in India and identifies areas of opportunities. The key take-away is India’s substantial progress in increasing coverage of PC and introduction of novel STH-control strategies. However, there remain knowledge gaps and the need to address region-specific needs regarding STH control. This can be achieved through active collaboration by pertinent agencies including governments, NGOs, civil society, WHO, bio/pharmaceutical industry and multi-sectoral co-ordination.
*The above list is not exhaustive
[1]. World Health Organization. Soil transmitted helminth infection [internet]. https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections. Accessed May 1, 2020 [Google Scholar]
[2]. Salam N, Azam S, Prevalence and distribution of soil-transmitted helminth infections in IndiaBMC Public Health 2017 17:20110.1186/s12889-017-4113-228209148 [Google Scholar] [CrossRef] [PubMed]
[3]. Silver ZA, Kaliappan SP, Samuel P, Venugopal S, Kang G, Sarkar R, Geographical distribution of soil transmitted helminths and the effects of community type in South Asia and South East Asia-A systematic reviewPLoS Negl Trop Dis 2018 12:e000615310.1371/journal.pntd.000615329346440 [Google Scholar] [CrossRef] [PubMed]
[4]. Pullan RL, Smith JL, Jasrasaria R, Brooker SJ, Global numbers of infection and disease burden of soil transmitted helminth infections in 2010Parasit Vectors 2014 7:3710.1186/1756-3305-7-3724447578 [Google Scholar] [CrossRef] [PubMed]
[5]. Jain S, Dwivedi A, Shrivastava A, Vijayananth P, Vidyavardhini R, Venkatesh S, Prevalence of soil-transmitted helminthic infection in india in current scenario: A systematic reviewJ Commun Dis 2016 48(2):24-35. [Google Scholar]
[6]. Jia TW, Melville S, Utzinger J, King CH, Zhou XN, Soil-transmitted helminth reinfection after drug treatment: A systematic review and meta-analysisPLoS Negl Trop Dis 2012 6(5):e162110.1371/journal.pntd.000162122590656 [Google Scholar] [CrossRef] [PubMed]
[7]. Government of India. Guideline on Filariasis Elimination [internet]. http://nvbdcp.gov.in/doc/guidelines-filariasis-elimination-india.pdf. Accessed May 1, 2020 [Google Scholar]
[8]. World Health Organization. Preventive chemotherapy to control soil-transmitted helminth infections in at-risk population groups: Guideline. Geneva: WHO; 2017. http://www.who.int/nutrition/publications/guidelines/deworming/en/. Accessed May 1, 2020 [Google Scholar]
[9]. Abraham D, Kaliappan SP, Walson JL, Rao Ajjampur SS, Intervention strategies to reduce the burden of soil-transmitted helminths in IndiaIndian J Med Res 2018 147(6):533-44.10.4103/ijmr.IJMR_881_1830168484 [Google Scholar] [CrossRef] [PubMed]
[10]. Greenland K, Dixon R, Khan SA, Gunawardena K, Kihara JH, Smith JL, The epidemiology of soil-transmitted helminths in Bihar State, IndiaPLoS Negl Trop Dis 2015 9(5):e000379010.1371/journal.pntd.000379025993697 [Google Scholar] [CrossRef] [PubMed]
[11]. Ganguly S, Barkataki S, Karmakar S, Sanga P, Boopathi K, Kanagasabai K, High prevalence of soil-transmitted helminth infections among primary school children, Uttar Pradesh, India, 2015Infect Dis Poverty 2017 6:13910.1186/s40249-017-0354-728988538 [Google Scholar] [CrossRef] [PubMed]
[12]. Kiran T, Shashwati N, Vishal B, Kumar D, Intestinal parasitic infections and demographic status of school children in Bhopal region of Central IndiaIOSR J Pharm Biol Sci 2014 9:83-87.10.9790/3008-09528387 [Google Scholar] [CrossRef]
[13]. GiveWell. Prevalence of Soil Transmitted Helminths in the State of Rajasthan. Summary Report prepared by ‘Deworm the World Initiative’. 2013. http://files.givewell.org/files/DWDA%202009/DtWI/DtWI%20Rajasthan%202013%20prevalence%20survey%20report.pdf. Accessed May 1, 2020 [Google Scholar]
[14]. GiveWell. Report on Prevalence and Intensity of Soil Transmitted Helminth Infections in Chattisgarh. http://files.givewell.org/files/DWDA%202009/DtWI/Deworm_the_World_Chhattisgarh_prevalence_survey_report_August_2016.pdf. Accessed May 1, 2020 [Google Scholar]
[15]. Kaliappan SP, George S, Francis MR, Kattula D, Sarkar R, Minz S, Prevalence and clustering of soil-transmitted helminth infections in a tribal area in Southern IndiaTrop Med Int Health 2013 18(13):1452-62.10.1111/tmi.1220524237860 [Google Scholar] [CrossRef] [PubMed]
[16]. Kattula D, Sarkar R, Rao Ajjampur SS, Minz S, Levecke B, Muliyil J, Prevalence & risk factors for soil transmitted helminth infection among school children in South IndiaIndian J Med Res 2014 139(1):76-82. [Google Scholar]
[17]. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010Lancet 2012 380(9859):2197-223.10.1016/S0140-6736(12)61689-4 [Google Scholar] [CrossRef]
[18]. Bundy DA, Chan MS, Savioli L, Hookworm infection in pregnancyTrans R Soc Trop Med Hyg 1995 89(5):521-22.10.1016/0035-9203(95)90093-4 [Google Scholar] [CrossRef]
[19]. Brooker S, Bethony J, Hotez PJ, Human hookworm infection in the 21st centuryAdv Parasitol 2004 58:197-288.10.1016/S0065-308X(04)58004-1 [Google Scholar] [CrossRef]
[20]. Tshikuka JG, Gray-Donald K, Scott M, Olela KN, Relationship of childhood protein-energy malnutrition and parasite infections in an urban African settingTrop Med Int Health 1997 2(4):374-82.10.1111/j.1365-3156.1997.tb00154.x9171847 [Google Scholar] [CrossRef] [PubMed]
[21]. Lustigman S, Prichard RK, Gazzinelli A, Grant WN, Boatin BA, McCarthy JS, A research agenda for helminth diseases of humans: The problem of helminthiasesPLoS Negl Trop Dis 2012 6(4):e158210.1371/journal.pntd.000158222545164 [Google Scholar] [CrossRef] [PubMed]
[22]. National Centre for Disease Control. Directorate General of Health Services, Government of India [internet]. https://ncdc.gov.in/index1.php?lang=1&level=1&sublinkid=166&lid=55. Accessed May 1, 2020 [Google Scholar]
[23]. Sustainable sanitation in India [internet]. http://www.gtz.de/en/dokumente/en-ecosan-sustainablesanitation-india-2008.pdf. Accessed May 1, 2020 [Google Scholar]
[24]. Government of India. National Urban Sanitation Policy. Ministry of Urban Development, GOI [internet]. https://smartnet.niua.org/sites/default/files/resources/National%20Urban%20Sanitation%20Policy.pdf. Accessed May 1, 2020 [Google Scholar]
[25]. Swachh Bharat Mission [internet]. http://swachhbharatmission.gov.in/sbmcms/index.htm. Accessed May 1, 2020 [Google Scholar]
[26]. Nirmal Gram Puraskar [internet]. http://www.indiaenvironmentportal.org.in/files/ngp-guidelines_March_2010.pdf. Accessed May 1, 2020 [Google Scholar]
[27]. Swachh Bharat Swachh Vidyalaya [internet]. https://vikaspedia.in/health/sanitation-and-hygiene/swachh-bharat-swachh-vidyalaya. Accessed May 1, 2020 [Google Scholar]
[28]. National Deworming Day. National Health Portal of India [internet]. https://www.nhp.gov.in/National-Deworming-Day_pg. Accessed May 1, 2020 [Google Scholar]
[29]. Drake LJ, Singh S, Mishra CK, Drake LJ, Singh S, Mishra CK, Bihar’s Pioneering School-Based Deworming Programme: Lessons Learned in Deworming over 17 Million Indian School-Age Children in One Sustainable CampaignPLoS Negl Trop Dis 2015 9(11):e000410610.1371/journal.pntd.000410626584484 [Google Scholar] [CrossRef] [PubMed]
[30]. Sustainable Development Goals. Knowledge Platform [internet]. https://sustainabledevelopment.un.org/. Accessed May 1, 2020 [Google Scholar]
[31]. Freeman MC, Clasen T, Assessing the impact of a school-based safe water intervention on household adoption of point-of-use water treatment practices in Southern IndiaAm J Trop Med Hyg 2011 84(3):370-78.10.4269/ajtmh.2011.10-036121363972 [Google Scholar] [CrossRef] [PubMed]
[32]. Clasen T, Boisson S, Routray P, Torondel B, Bell M, Cumming O, Effectiveness of a rural sanitation programme on diarrhoea, soil-transmitted helminth infection, and child malnutrition in Odisha, India: A cluster-randomised trialLancet Glob Health 2014 2(11):e645-53.10.1016/S2214-109X(14)70307-9 [Google Scholar] [CrossRef]
[33]. Patil SR, Arnold BF, Salvatore AL, Briceno B, Ganguly S, Colford Jr JM, The effect of India’s total sanitation campaign on defecation behaviours and child health in rural Madhya Pradesh: A cluster randomized controlled trialPLoS Med 2014 11:e100170910.1371/journal.pmed.100170925157929 [Google Scholar] [CrossRef] [PubMed]
[34]. World Health Organization. Accelerating work to overcome the global impact of neglected tropical diseases: A roadmap for implementation. Geneva: WHO; 2012. http://www.who.int/neglected_diseases/NTD_RoadMap_2012 Fullversion.pdf. Accessed May 1, 2020 [Google Scholar]
[35]. Solomon R, Involvement of Civil Society in India’s Polio Eradication Program: Lessons LearnedAm J Trop Med Hyg 2019 101(4 suppl):15-20.10.4269/ajtmh.18-093131760980 [Google Scholar] [CrossRef] [PubMed]
[36]. Global Atlas of Helminth Infections [internet]. http://www.thiswormyworld.org/. Accessed May 1, 2020 [Google Scholar]
[37]. World Health Organization. Expanded Special Project for Elimination of Neglected tropical diseases (ESPEN). WHO: Regional Office for Africa. 2018. https://www.afro.who.int/health-topics/expanded-special-project-elimination-neglected-tropical-disease. Accessed May 1, 2020 [Google Scholar]
[38]. Brooker S, Beasley M, Ndinaromtan M, Madjiouroum EM, Baboguel M, Djenguinabe E, Use of remote sensing and a geographical information system in a national helminth control programme in ChadBull World Health Organ 2002 80(10):783-89. [Google Scholar]
[39]. Scholte RG, Schur N, Bavia ME, Carvalho EM, Chammartin F, Utzinger J, Spatial analysis and risk mapping of soil-transmitted helminth infections in Brazil, using Bayesian geostatistical modelsGeospat Health 2013 8(1):97-110.10.4081/gh.2013.5824258887 [Google Scholar] [CrossRef] [PubMed]
[40]. Brooker S, Singhasivanon P, Waikagul J, Supavej S, Kojima S, Takeuchi T, Mapping soil-transmitted helminths in Southeast Asia and implications for parasite controlSoutheast Asian J Trop Med Public Health 2003 34(1):24-36. [Google Scholar]
[41]. Kulinkina AV, Sarkar R, Mohan VR, Walz Y, Kaliappan SP, Ajjampur SSR, Prediction of hookworm prevalence in southern India using environmental parameters derived from Landsat 8 remotely sensed dataInt J Parasitol 2020 50(2020):47-54.10.1016/j.ijpara.2019.10.00131756313 [Google Scholar] [CrossRef] [PubMed]
[42]. Truscott JE, Turner HC, Farrell SH, Anderson RM, Soil-transmitted helminths: Mathematical models of transmission, the impact of mass drug administration and transmission elimination criteriaAdv Parasitol 2016 94:133-98.10.1016/bs.apar.2016.08.00227756454 [Google Scholar] [CrossRef] [PubMed]
[43]. Coffeng LE, Nery SV, Gray DJ, Bakker R, de Vlas SJ, Clements ACA, Predicted short and long-term impact of deworming and water, hygiene, and sanitation on transmission of soil-transmitted helminthsPLoS Negl Trop Dis 2018 12(12):e000675810.1371/journal.pntd.000675830522129 [Google Scholar] [CrossRef] [PubMed]
[44]. Anderson R, Truscott J, Hollingsworth TD, The coverage and frequency of mass drug administration required to eliminate persistent transmission of soil-transmitted helminthsPhilos Trans R Soc Lond B Biol Sci 2014 369(1645):2013043510.1098/rstb.2013.043524821921 [Google Scholar] [CrossRef] [PubMed]
[45]. Moser W, Schindler C, Keiser J, Efficacy of recommended drugs against soil transmitted helminths: Systematic review and network meta-analysisBMJ 2017 358:j430710.1136/bmj.j430728947636 [Google Scholar] [CrossRef] [PubMed]
[46]. Bethony J, Chen J, Lin S, Xiao S, Zhan B, Li S, Emerging patterns of hookworm infection: Influence of aging on the intensity of Necator infection in Hainan province, People’s Republic of ChinaClin Infect Dis 2002 35(11):1336-44.10.1086/34426812439796 [Google Scholar] [CrossRef] [PubMed]
[47]. The Kenya National Breaking Transmission Strategy for Soil-Transmitted Helminthiasis, Schistosomiasis, Lymphatic Filariasis And Trachoma [internet]. https://www.eliminateschisto.org/sites/gsa/files/content/attachments/2019-07-07/Kenya%20Breaking%20Transmission%20Strategy%20for%20NTDs_Final%20PDF.pdf. Accessed May 1, 2020 [Google Scholar]
[48]. Geerts S, Gryseels B, Drug resistance in human helminths: Current situation and lessons from livestockClin Microbiol Rev 2000 13(2):207-22.10.1128/CMR.13.2.20710755998 [Google Scholar] [CrossRef] [PubMed]
[49]. Gill BS, Anthelmintic resistance in IndiaVet Parasitol 1996 63(1-2):173-76.10.1016/0304-4017(95)00884-5 [Google Scholar] [CrossRef]
[50]. Swarnkar CP, Sanyal PK, Singh D, Khan FA, Bhagwan PS, Anthelmintic resistance on an organized sheep farm in IndiaTrop Anim Health Prod 2001 33(4):305-12.10.1023/A:101053601921011474864 [Google Scholar] [CrossRef] [PubMed]
[51]. Papaiakovou M, Pilotte N, Williams SA, Recent advances in developing an optimized qPCR system for STH detection in stoolSoil-Transmitted Helminthiasis Advisory Committee Meeting 2017 Baltimore, MD [Google Scholar]
[52]. Shalaby HA, Anthelmintics Resistance; How to Overcome it?Iran J Parasitol 2013 8(1):18-32. [Google Scholar]
[53]. Bergquist R, Johansen MV, Utzinger J, Diagnostic dilemmas in helminthology: What tools to use and when?Trends Parasitol 2009 25(4):151-56.10.1016/j.pt.2009.01.00419269899 [Google Scholar] [CrossRef] [PubMed]
[54]. Bärenbold O, Raso G, Coulibaly JT, N’Goran EK, Utzinger J, Vounatsou P, Estimating sensitivity of the Kato-Katz technique for the diagnosis of Schistosoma mansoni and hookworm in relation to infection intensityPLoS Negl Trop Dis 2017 11:e000595310.1371/journal.pntd.000595328976979 [Google Scholar] [CrossRef] [PubMed]
[55]. Becker SL, Liwanag HJ, Snyder JS, Akogun O, Belizario V Jr, Freeman MC, Toward the 2020 goal of soil-transmitted helminthiasis control and eliminationPLoS Negl Trop Dis 2018 12(8):e000660610.1371/journal.pntd.000660630106975 [Google Scholar] [CrossRef] [PubMed]
[56]. Mbong Ngwese MM, Prince Manouana G, Nguema Moure PA, Ramharter M, Esen M, Adégnika AA, Diagnostic techniques of soil-transmitted helminths: impact on control measuresTrop Med Infect Dis 2020 5(2):9310.3390/tropicalmed502009332516900 [Google Scholar] [CrossRef] [PubMed]
[57]. Freeman MC, Akogun O, Belizario V Jr, Brooker SJ, Gyorkos TW, Imtiaz R, Challenges and opportunities for control and elimination of soil-transmitted helminth infection beyond 2020PLoS Negl Trop Dis 2019 13(4):e000720110.1371/journal.pntd.000720130973872 [Google Scholar] [CrossRef] [PubMed]
[58]. World Health Organization. Water sanitation & hygiene for accelerating and sustaining progress on neglected tropical diseases: a global strategy 2015-2020. Geneva: WHO. https://www.who.int/water_sanitation_health/publications/wash-and-ntd-strategy/en/. Accessed May 1, 2020 [Google Scholar]
[59]. Ziegelbauer K, Speich B, Mäusezahl D, Bos R, Keiser J, Utzinger J, Effect of sanitation on soil-transmitted helminth infection: Systematic review and meta-analysisPLoS Med 2012 9(1):e100116210.1371/journal.pmed.100116222291577 [Google Scholar] [CrossRef] [PubMed]
[60]. Strunz EC, Addiss DG, Stocks ME, Ogden S, Utzinger J, Freeman MC, Water, sanitation, hygiene, and soil-transmitted helminth infection: A systematic review and meta-analysisPLoS Med 2014 11(3):e100162010.1371/journal.pmed.100162024667810 [Google Scholar] [CrossRef] [PubMed]
[61]. Tomczyk S, Deribe K, Brooker SJ, Clark H, Rafique K, Knopp S, Association between footwear use and neglected tropical diseases: A systematic review and meta-analysisPLoS Negl Trop Dis 2014 8(11):e328510.1371/journal.pntd.000328525393620 [Google Scholar] [CrossRef] [PubMed]
[62]. Nakagawa J, Ehrenberg JP, Nealon J, Fürst T, Aratchige P, Gonzales G, Towards effective prevention and control of helminth neglected tropical diseases in the Western Pacific Region through multi-disease and multi-sectoral interventionsActa Trop 2015 141:407-18.10.1016/j.actatropica.2013.05.01023792012 [Google Scholar] [CrossRef] [PubMed]