Type 2 Diabetes Mellitus (T2DM) is a severe, chronic, and progressive disease whose prevalence is increasing rapidly and accounts for up to 90% of DM cases. Insulin Resistance (IR) contributes to the development of T2DM in approximately 92% of patients [1]. IR is characterised by an impaired ability of insulin to inhibit glucose output from the liver and to promote glucose uptake in fat and muscle. Obesity and decreased levels of physical activity were found to be the significant risk factors for IR. However, the precise mechanism by which obesity leads to IR and T2DM is not known completely [2].
Thiazolidinediones (TZDs) are a class of oral hypoglycaemic agents shown to enhance hepatic and muscle insulin sensitivity by binding to and activating Peroxisome Proliferator-Activated Receptor gamma (PPARγ). Additional effects of TZDs that were shown to reverse IR in T2DM include reduced expression of adipokines, increased plasma adiponectin levels [3], decreased production of inflammatory cytokine TNFα from macrophages [4], among others. Pioglitazone is the most common TZD used for treating T2DM patients in clinical practice. However, a host of adverse events, including body weight gain, peripheral oedema, congestive heart failure, bone fractures, and possibly bladder cancer, have restricted the use of pioglitazone. Having shown favourable risk-benefit ratio in a recent meta-analysis [5] in terms of improving glucose and lipid metabolism, the development of oedema and body weight gain due to pioglitazone usage were still detrimental in T2DM patients with previously diagnosed heart failure. None of the newer drugs (DPP-4 inhibitors, glucagon-like peptide-1 receptor agonists, and sodium-glucose co-transporter 2 inhibitors) target IR. So, there is an urgent need for an alternative drug whose efficacy is comparable to pioglitazone.
Materials and Methods
This was an interventional study conducted from October, 2015 to December, 2015 at the research laboratory of the KS Hegde Medical Academy, Mangalore, Karnataka, India. Approval from the Institutional Animal Ethical Committee (IAEC) was obtained before starting the study (KSHEMA/IAEC/20/2013).
Experimental Animals
The present study included 24 healthy wistar strain albino rats weighing around 240-270 g. They were kept in clean, well-ventilated and temperature-controlled (25°C±2°C) polypropylene cages with a constant 12 hours light/dark schedule. Standard rat pellet diet and clean drinking water was made available to all the animals ad libitum.
Preparation of Momordica Charantia Seed Extract (MCSE)
Momordica charantia fruit purchased from the local market were used in the study. The fruit was cut, and seeds were separated, dried under shade, and then grounded into a fine powder by using a household electronic grinder. An aqueous suspension was prepared by dissolving a known amount of seed powder in distilled water. The dosage schedule for the MCSE was 2500 mg/kg body weight per day for 12 days [10].
Experimental Set up
A total of 24 rats were randomly divided into four groups, six rats in each group. Bodyweight was checked for all groups on day one, day seven, and day 12.
Group I: Diabetic Control- Rats received dexamethasone alone in a dose of 8 mg/kg body weight [10] intraperitoneally for six days to induce metabolic changes. Rats were also given 10 mL/kg of 2% gum acacia orally.
Group II: Test Group- Rats received MCSE (2500 mg/kg body weight) in aqueous solution suspended in 10 mL/kg of 2% gum acacia orally six days before dexamethasone and six days during dexamethasone administration.
Group III: Standard Group- Rats received pioglitazone 75 mg/kg body weight suspended in 10 mL/kg of 2% gum acacia orally six days before dexamethasone and six days during dexamethasone administration.
Group IV: Normal Control- Rats were given only 10 mL/kg of 2% gum acacia.
[Table/Fig-1] shows the details of the study protocol.
Study protocol N=6 in each group.
| Group | Day 1-12 (7 AM) | Day 7-12 (7.30 AM) | Day 11 | Day 12 (8 AM) |
|---|
| I- Diabetic control | 10 mL/kg oral of 2% gum acacia | Dexamethasone 8 mg/kg i.p. | Overnight fast (from 4 PM) | Blood was drawn by tail-flick method for FBS, lipid profile, and PPBS*. Rats were sacrificed**, liver weight, and volume measured and sent for histopathology***. |
| II- Test control | MCSE 2.5 g/kg/10 mL of 2% gum acacia | Dexamethasone 8 mg/kg i.p. |
| III- Standard control | 75 mg/10 mL of 2% gum acacia/kg pioglitazone | Dexamethasone 8 mg/kg i.p. |
| IV- Normal control | 10 mL/kg oral of 2% gum acacia | NS 2 ml/kg i.p. |
FBS: Fasting blood sugar; PPBS: Postprandial blood sugar; i.p.: Intraperitoneally
*PPBS was measured 2 hours after a glucose load of 2 g/10 mL/kg, i.p
**Rats were sacrificed by cervical dislocation as per the CPCSEA (Committee for the Purpose of Control and Supervision of Experiments on Animals) guideline approved method of euthanasia
***Livers were stored in 10% formalin and sent for histopathological analysis
Statistical Analysis
All experimental results were represented as the Mean±SD for six animals per group. Data were analysed by using Statistical Package for the Social Sciences (SPSS) version 17.0 (SPSS Inc. Released 2008. SPSS Statistics for Windows, Version 17.0. Chicago: SPSS Inc.). An Independent t-test was used to compare between two groups. ANOVA with Scheffe’s post-hoc test was done for multiple comparisons. Statistical significance was set at p<0.05.
Results
Effect of MCSE on Blood Sugar Levels in Rats
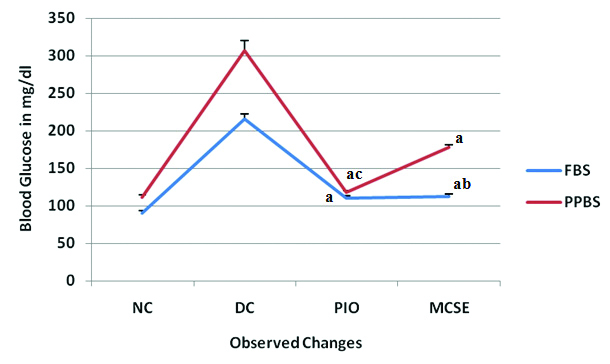
The blood sugar levels of the four groups are shown in [Table/Fig-2]. Both fasting and postprandial blood glucose levels were increased in diabetic control group in comparison to normal controls. FBS and PPBS levels were significantly decreased in both MCSE and pioglitazone-treated groups in comparison to diabetic controls (p<0.01). Among MCSE and pioglitazone-treated groups, fasting blood glucose levels were comparable in both the groups (p=0.196), but significant decrease in postprandial blood glucose levels was observed (p<0.01) in the pioglitazone group.
Line chart showing the effect of MCSE on blood sugar levels in rats (n=6 per group). Values are mean±SD. ap<0.01 vs dexamethasone control, bp=0.196 vs pioglitazone group, cp<0.01 vs MCSE group. NC: Normal control; DC: Dexamethasone control; PIO: Pioglitazone; MCSE: Momordica charantia seed extract
Effect of MCSE on Lipids
The values of lipid profile of all four groups are shown in [Table/Fig-3]. Total Cholesterol (TC) and Triglyceride (TG) levels were increased and high-density lipoprotein (HDL) levels were decreased in diabetic control group in comparison to normal controls. Also, TC and TG levels were significantly decreased and HDL levels were significantly increased in both MCSE and pioglitazone-treated groups in comparison to diabetic controls (p<0.01). Among MCSE and pioglitazone-treated groups, pioglitazone-treated groups had lower TC and TG levels (p=0.059, p=0.376) and higher HDL levels (p=0.81), but they were not statistically significant.
Effect of MCSE on lipids, liver weight, and liver volume in rats (n=6 per group). Values are Mean±SD. ap<0.01 vs Dexamethasone Control, bp=0.059, 0.376, 0.81 vs pioglitazone-treated group, cp =0.322, 0.155 vs pioglitazone-treated group. HDL: High-density lipoproteins; SD: Standard deviation
| Group | Total cholesterol (mg/dL) | Triglycerides (mg/dL) | HDL (mg/dL) | Liver weight (g) | Liver volume (mL) |
|---|
| Normal control | 88.75±5.31 | 68.25±1.71 | 39.67±2.665 | 6.769±0.2641 | 6.597±0.318 |
| Diabetic control | 190.33±5.503 | 155.08±4.32 | 17.57±2.091 | 13.36±0.3742 | 13.730±0.294 |
| Standard (Pioglitazone) | 115.33±4.32a | 87.37±1.789a | 38.19±2.87a | 8.059±0.2944a | 7.737±0.463a |
| Test (MCSE) | 120.63±4.32ab | 88.92±3.692ab | 37.85±1.781ab | 8.226±0.2608ac | 8.077±0.2828ac |
Effect of MCSE on Liver Weight and Liver Volume
Liver weight and volume was more in diabetic controls in comparison to normal controls [Table/Fig-3]. A significant decrease in the liver weight and volume was observed in the MCSE and pioglitazone-treated groups as compared to diabetic controls (p<0.01). Among MCSE and pioglitazone-treated groups, liver weight and volume was less in pioglitazone-treated group compared to MCSE treated group (p=0.322, p=0.155), but the difference was not statistically significant.
Effect of MCSE on Body Weight
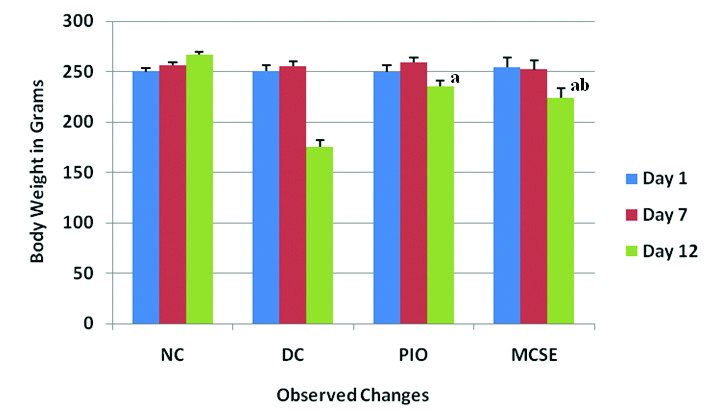
The body weights of the four groups are shown in [Table/Fig-4]. There was a decrease in body weight in diabetic controls in comparison to normal controls on day 12. However, the body weight was significantly more in MCSE and pioglitazone-treated groups in comparison to diabetic controls (p<0.01). There was a comparable difference in body weight between MCSE and pioglitazone-treated groups (p=0.044).
Column chart showing the effect of MCSE on body weight in rats (n=6 per group). Values are mean±SD. ap<0.01 vs dexamethasone control, bp=0.044 vs pioglitazone group. NC: Normal control; DC: Dexamethasone control; PIO: Pioglitazone; MCSE: Momordica charantia seed extract.
Histopathological Observations
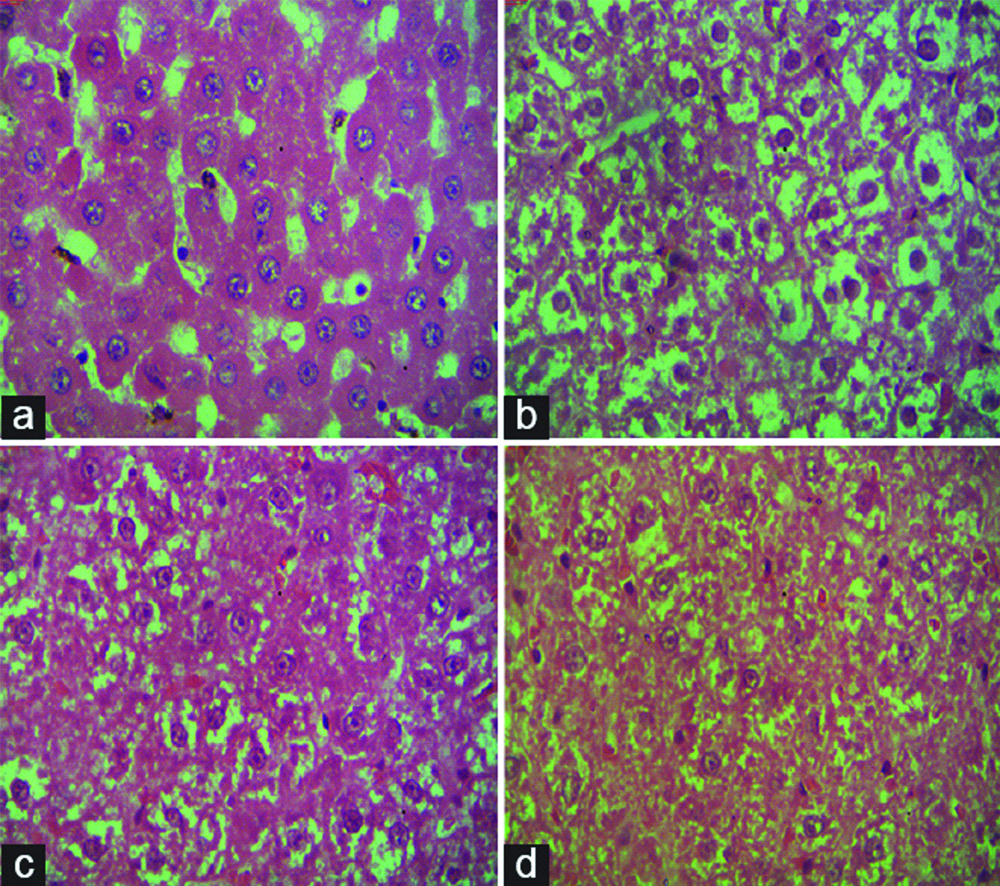
Rats in normal control group had normal hepatocytes. However, the rats in diabetic control group showed an increase in the size of hepatocytes with fat deposition. Reduction in the size of hepatocytes along with reduced-fat deposition was observed in Standard control as well as Test control rats compared to Diabetic control rats [Table/Fig-5].
Histopathological changes of rat liver tissue (H&E; ×40). (a) Hepatocytes in the normal control group; (b) Hepatocytes in DEX treated group showing fat deposition pushing the nucleus to the periphery; (c and d) Hepatocytes showing reduced fat deposition in pioglitazone and MCSE treated rats, respectively.
Discussion
The present study revealed that intraperitoneal injection of a single dose (8 mg/kg body weight) of dexamethasone to adult albino rats was suitable to induce hyperglycaemia, dyslipidemia, and hepatic steatosis. As all these features are part of metabolic syndrome produced by IR in T2DM, they can be prevented by using insulin sensitisers like pioglitazone.
In the present study, MCSE was as effective as pioglitazone in reducing fasting and postprandial serum glucose levels compared to the diabetic control group. However, postprandial blood glucose levels were significantly decreased in the pioglitazone group compared to the MCSE group. These results are in accordance with the findings of a study done by Ali L et al., administration of bitter melon juice caused low fasting blood glucose levels and decreased glucose tolerance in NIDDM model rats [11]. Similar findings were also observed in a study conducted in T2DM patients [12]. The glucose-lowering effect of M.charantia in diabetic rats is attributed to increased activity of PPAR-γ compared to the diabetic control group [13].
Treatment with 2500 mg/kg body weight of M.charantia seed extract to diabetic rats decreased TC and TG and increased HDL levels significantly. These results are in agreement with the findings by Rahman IU et al., who observed favourable changes in the TC and HDL levels from baseline to endpoint, except for the TGs that achieved statistical significance in a group of subjects receiving bitter melon 4 g/day [14]. On the contrary, Kumari S et al., reported that 1.5 gm of M.charantia as add on treatment along with a stable dose of oral antidiabetic lowered TC and increased HDL levels significantly, no beneficial effect on TGs was observed [15]. This lipid-lowering effect of M.charantia is attributed to its ability to increase AMPK phosphorylation, and PPARγ mediated lipid metabolism in the liver [16].
Clinical data implicating Glucocorticoids (GC) in the pathogenesis of hepatic steatosis are limited, however existing data suggest enhanced Lipoprotein Lipase (LPL) activity on GC exposure, which mediates the breakdown and uptake of circulating TGs and Free Fatty Acids (FFA) into adipocytes and hepatocytes leading to de-novo lipogenesis in these tissues [17]. In the present study, the treatment of diabetic rats with MCSE reduced the accumulation of fat in the liver, comparable to pioglitazone-treated rats. Yoon NA et al., reported similar findings in mice with high-fat diet-induced T2DM [18]. The mechanism by which M.charantia attenuates hepatic steatosis was suggested by Yu Y et al., who demonstrated that bitter melon significantly enhances Fibroblast Growth Factor 21 (FGF21) and AMPK/Sirt1 signaling in hepatocytes [19].
Regarding body weight, the obtained data indicate that the MCSE prevented a decrease in body weight caused by dexamethasone administration. This may be ascribed to the insulin-secreting property of M.charantia [20]. However, M.charantia was also shown to decrease body weight in studies conducted with overweight rats [21] and T2DM patients with BMI >25/kg/m2 [14]. Prevention of adipocyte differentiation and visceral fat accumulation by the extracts of M.charantia were suggested mechanisms for this decrease in body weight [22].
Overall in the present study, the treatment of diabetic rats with MCSE resulted in favourable hypoglycaemic and hypolipidemic effects comparable to pioglitazone.
Limitation(s)
The total duration of the study was 12 days, and the dose of M.charantia seed aqueous extract used was 2500 mg/kg body weight per day. Hence, longer duration of the study could have checked the safety and sustainability of the antidiabetic effects of M.charantia in a steroid-induced diabetes model in a better manner.
Conclusion(s)
The majority of T2DM patients are obese, which should not be aggravated by a drug used in the management of these patients. Since lifestyle interventions such as nutrition therapy and regular physical activity are important approaches in the management of diabetes mellitus, the antidiabetic effect of M.charantia is useful to the maximum extent. Due to its weight-lowering effect, MCSE could be an add-on therapy for the treatment of T2DM in obese patients. It may substitute pioglitazone provided its safety and efficacy is being proved in well-controlled randomised clinical trials in humans.