Over the years it has been proven that a healthy and safe labour is among the top priorities of any health care system in the world. According to WHO, the rate of Cesarean Section (CS) has increased from 6.7% to 19.1% from 1990 to 2014 [1]. Similar, but rather faster, rates were reported in Iran from 16% to 60% from 1985 to 2013 [1,2].
Studies in Iran found three major reasons for the Iranian women’s tendency toward CS deliveries. These include: social and demographic features, medical or obstetric considerations and non-obstetric problems [1]. Among these, fear of Labour pain is the most common ground for all three etiologies as it is one of the biggest challenges that a woman could face during natural delivery [1-3]. Furthermore, the pain could lead to anxiety and stress which could consequently cause a total or partial deterioration of the mothers’ status during Labour. These include prolonged deliveries and a sense of fear of Labour in women for future pregnancies [4]. Although, holding general pre-Labour educational classes for mothers seems promising, but this to cope up with labour pain requires other treatment methods, facilitating the complex process of Labour, especially for the primigravidae [5].
Pharmacological and nonpharmacological modalities are the two basic methods for managing the Labour pain in women. While anesthetic approaches (i.e., epidural or spinal analgesia, etc.,) are now among the common medical treatments, non-medical approaches like acupuncture, hypnosis and Psycho-prophylactic and TENS have been introduced and are being studied and actively evaluated in the recent years [6,7].
TENS is considered as a nonpharmacological modality in treating many conditions in recent years, including the relief from Labour pain. Based on different studies, the mechanism of this procedure is still controversial [8]. However, as it is assumed as a nonharmful method, both for the mother and the fetus, widespread studies have been conducted to better evaluate this procedure during active phases of Labour to eliminate the pain [8-10]. TENS method, which is rather new than Acupuncture, includes electrical stimulation on certain areas, facilitating the use of TENS in active phases of Labour when the stress of the mothers are significantly Increased [6,10].
In some studies, the combination of TENS was used. In these studies, the TENS was placed on certain points used in traditional acupuncture method to evaluate the role of electrical impulses on decreasing the Labour pain [10-12]. Dowswell T et al, in a systematic review, evaluated the effect of TENS on Labour pain and found that fewer mothers reported severe Labour pain. Finally, they suggested that further studies be undertaken with emphasis on the early use of TENS in the early stages of Labour [8].
The aim of this study was to investigate the effect of concurrent use of TENS on thoracic-lumbar and acupuncture points (Hegu and Sanyinjiao) on pain relief from latent phase of Labour to evaluate the ways of encouraging women for choosing natural delivery in the future.
Materials and Methods
Study Type and Population
This was a double-blind randomised clinical trial study conducted on pregnant women in the Obstetrics and Gynecology Department of Al-zahra Hospital in Guilan University of Medical Sciences, in the north of Iran, during June-October, 2018. A total of 256 women were initially assessed according to eligibility criteria. Of the total, 104 eligible women were randomly assigned to the four groups of study.
Inclusion criteria:
Age: 18-40-year-old
Gestational age: 37-41 weeks.
Labour: singleton, cephalic presentation, latent phase of Labour (dilation less than four centimeters)
Estimated fetal weight <4000 g.
Negative history of: Anatomical disorders (e.g., pelvic abnormalities), Cephalo-Pelvic Disproportion (CPD), Psychological diseases (e.g., psychosis, schizophrenia), Chronic diseases (e.g., cardiac, pulmonary, hypertension, diabetes mellitus), Dermatological diseases (e.g., lesions, inflammations, eczema) on the areas of electrodes, Epidural or other analgesics use in 24 hours prior to Labour, Prior history of TENS or Acupressure managements, Rupture of membranes more than 12 hours before Labour, Use of narcotics 12 hours before Labour.
Not having high risk pregnancies (i.e., pre-eclampcia, polyhydramnious, sonography-confirmed oligohydramnious, decreased fetal movements).
Exclusion criteria:
Any emergencies throughout the Labour (e.g., Abraptio Placenta (AP), umbilical cord prolapsed, etc.,).
Patients’ refusal to continue the process.
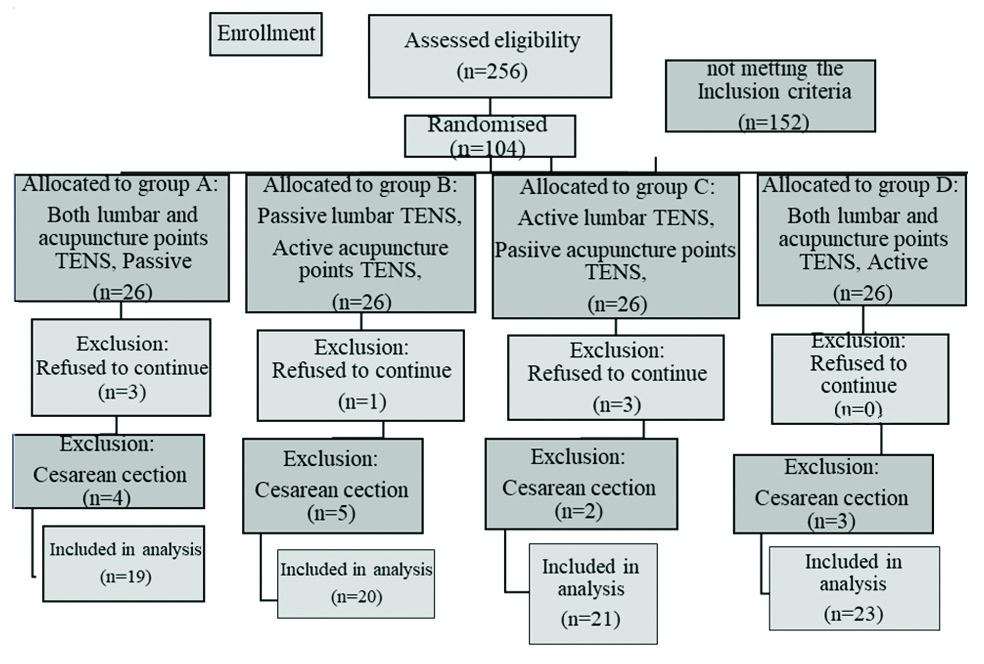
After enrolling in the study, seven patients withdrew from the study due to their unwillingness to attach to the TENS device wires and the study continued with 97 participants. Then, another 14 participants dropped out because of CS, and final outcome analysis was performed on 83 participants. [Table/Fig-1] illustrates the flow diagram of the study. The subjects were divided into four groups based upon the randomised balanced block method with the 1:1:1:1 ratio as A, B, C and D. The randomised sequences were obtained by the Random Generator Software. A serial number was written in sealed envelopes and they were taken out by the participants in the admission office of the Labour department. The staff of the Labour section (first operators) was also educated to take proper medical history, filling out forms and giving information about the TENS method and other possible question made by the participants.
CONSORT flowchart of the study.
The data collection instruments were labeled with unique serial number and all women in the four study groups received disposable pads. The participants and research assistants that measured the outcome of the study were blinded until the end of the study. The sample size of the study was calculated based on the study by Shahoei R et al., [13] with 90% statistical power, 95% confidence interval, 0.05 margin of error and considering 20% dropout rate, a minimum of 26 patients were calculated for each group.
The study protocol was approved by the ethical committee of Guilan University of Medical Sciences (code: IR.GUMS.REC.1396.300) and Clinical Trial Registration Code was obtained (IRCT20080826001096N6). Moreover, all the data remains confidential and results are reported as overall statistics and not applying to any specific individuals. Prior to performing the procedures, informed consents were obtained from the participants, following a comprehensive description of the study in their own words.
TENS Device
ELLE TENS device (with two pairs of electrodes) made in England (UK), portable by hand (size: 115×55 ×30 mm, weight: 75 g), battery: (2×1.5 AA battery, type: LR6), with output intensity 0-110 mA was used. The device would switch off automatically after five minutes if not used.
Acupuncture Points TENS Anatomical Locations
Hegu point (also known as large intestine 4:LI 4) is a strong acupressure point located as a dime-shaped area between the thumb and forefinger, just anterior to the anatomical snuffbox on the dorsal side of the hands [10].
Sanyinjiao point (also known as spleen point 6) is another acupressure point located five centimeters above the inner ankle, on the distal point of tibia [10,14]. The two pairs of disposable 30×30 mm electrodes were placed on the Hegu points of both hands and also the two electrodes were fixed on the points of the Sanyinjiao on two legs by elastic band.
Lumbar TENS Anatomical Locations
The lumbar TENS device was connected to two electrodes, each attached to a 10×15 cm disposable pad. These were then placed on the paravertebral regions adjacent to the T10-L1 spinal vertebrae in the upper portion and to the S2-S4 on the lower paravertebral Parts [11,13].
In order to maximise the assumed pain relief effects of this procedure, proper placements of the pads and electrodes were mandatory. The Acupuncture points-TENS device were handled by educated personnel, while the TENS device was controlled by the participants. Based on the total body weight of the subjects [10], appropriate stimulations ranging between zero to 110 mA were used.
The device was switched on or off by ON/OFF buttons, the starting point always being on the BURST1 mode (low voltage wavy impulses) on the ELLE TENS device. These BURST1 impulses were also used automatically, after BURST1 impulses, between the contractions, causing tingling sensations for mothers on the electrode sites [10]. On the other hand, BOOST1 stimulations were applied within the active contractions, introducing maximal pain killing effects.
Groups
All pregnant women involved in the study were treated with routine medical care including proper hydrations, fetal heart rate monitoring, maternal vital sign monitoring, and proper medication injections as indicated for any individual participant. The four groups of the study received the treatments as follows:
A: Placebo control group (both lumbar and acupuncture points TENS were passive): electrical pads and lumbar TENS pads were attached to the patients and low amplitude stimulations (about five mA) without frequency changes were sent, so that the mother experienced transient tingling sensations. This electrical stimulation was not repeated until the end of the first phase of the Labour.
B: Passive lumbar TENS-Active acupuncture points TENS: the acupressure points were stimulated for half an hour for each mother and in case the participant was eager to receiving the pulse again, more stimulation was sent up to 4 series of electrical waves.
However, for lumbar TENS low amplitude stimulations (about five mA) without frequency changes were sent, so that the mother experienced transient tingling sensations. This electrical stimulation was not repeated until the end of the first phase of the Labour.
C: Active lumbar TENS-Passive acupuncture points TENS, based on the BURST1 and BOOST1 stimulations, instructed to the subjects (as mentioned in the design section), whereas, for acupuncture points TENS low amplitude stimulations (about five mA) without frequency changes were sent, so that the mother experienced transient tingling sensations. This electrical stimulation was not repeated until the end of the first phase of the Labour.
D: Both lumbar and acupuncture points TENS were active, so that for TENS BURST1 and BOOST1 stimulations were sent, according to the contraction or in between the contractions (as mentioned in the design section).
Outcome Measurements
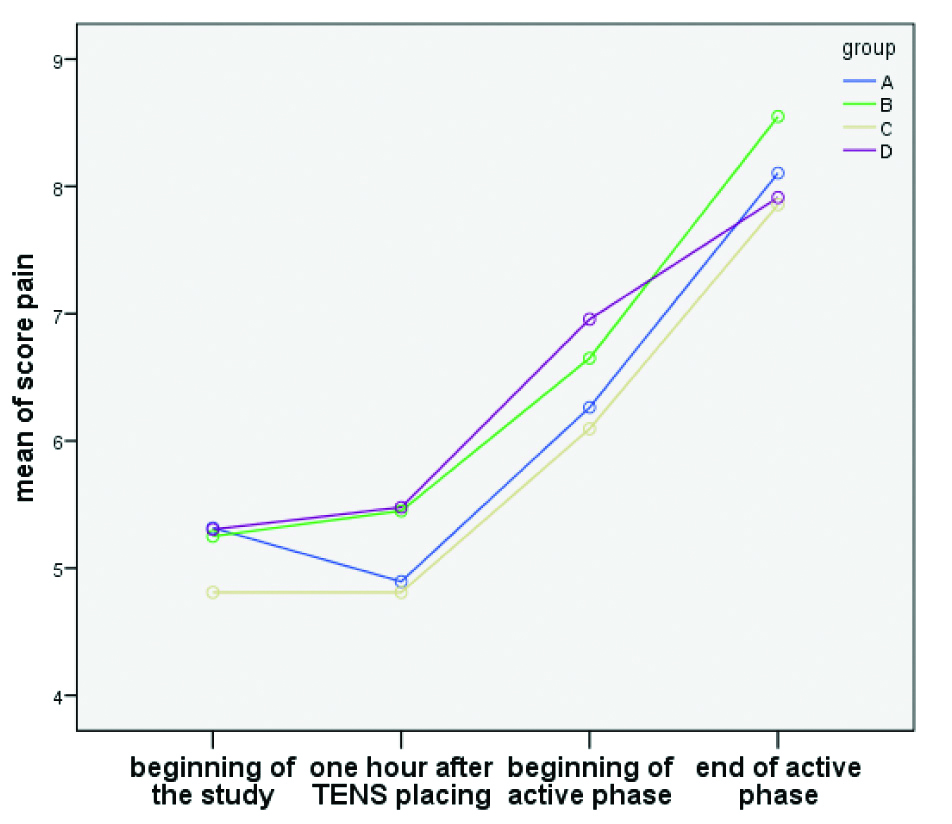
Pain score was measured using VAS, where zero stated no pain and ten expressed the highest level of pain as stated by the participants. The pain score was recorded at four study points including the beginning of the study (before the electrode placing), one hour after the placing of the electrodes, the beginning and end of stage of the active phase of Labour.
Postpartum haemorrhage in vaginal delivery is known as blood loss more than 500 mm or visual estimation of blood loss [15]. In the present study, postpartum haemorrhage was assessed by measuring and visually estimating the amount of blood on the pads.
Participant satisfaction toward the procedure was measured using a questionnaire containing three items- mobility restrictions, comfort of placing the electrodes on the body, tendency toward using the device for future pregnancy. The response as measured in a 3 point Likert scale (satisfied, no opinion and unsatisfied). The questionnaire was validated using content validity method and measuring content validity index was over 0.79. The reliability of the questionnaire was confirmed by alpha Cronbach of 0.73.
Statistical Analysis
Data were analysed by the Statistical Package for the Social Sciences (SPSS) software version 20. The variables were initially evaluated for normal distribution using Kolmogrov-Smirnov tests. The groups were compared using chi-square, Kruskal Wallis test, as appropriate. The trend of pain score over the study time points were assessed using GEE. The significant cut-off point was considered as p-values less than 0.05.
Results
The mean age of the participants was 27.86±5.92 years. There were no significant differences among the groups based on their demographic characteristics [Table/Fig-2].
Baseline characteristics of the participants according to the study groups.
| Groups variables | Both lumbar and acupuncture points TENS, Passive (Group A) | Passive lumbar TENS- Active acupuncture points TENS (Group B) | Active lumbar TENS- Passive acupuncture points TENS (Group C) | Both lumbar and acupuncture points TENS, Active (Group D) | Total (%)±SD | p-value |
|---|
| Total | 23 | 25 | 23 | 26 | 97 | - |
|---|
| aMaternal age (year): Mean±SD | 27.83±6.10 | 26.84±6.16 | 26.30±5.42 | 30.23±5.51 | 27.86±5.92 | 0.08 |
| Educational statusNo (%) | Uneducated up to middle school | 8 (34.8) | 9 (36) | 10 (43.5) | 12 (1/46) | 39 (40.3) | 0.654 |
| High school and above | 15 (65.2) | 16 (64) | 13 (56.5) | 14 (53.9) | 58 (59.7) |
| Occupational statusNo (%) | Housewife | 23 (100) | 23 (92.0) | 21 (91.3) | 26 (100) | 93 (95.9) | 0.233 |
| Employed | 0 (0) | 2 (8.0) | 2 (8.7) | 0 (0) | 4 (4.1) |
| aBody Mass Index (BMI) | Mean±SD | 29.22±5.42 | 31.05±6.15 | 30.63±4.94 | 31.31±6.09 | 30.59±5.66 | 0.61 |
| aHeight (cm) | Mean±SD | 160.4±6.2 | 160.7±6.5 | 161.5±5.4 | 160.9±5.3 | 160.9±6.1 | 0.936 |
| ParityNo (%) | Nulliparity | 8 (34.8) | 13 (52) | 14 (60.9) | 14 (53.8) | 49 (50.5) | 0.334 |
| Multiparity | 15 (65.2) | 12 (48) | 9 (39.1) | 12 (46.2) | 48 (49.5) |
| aGestational age (wk) | Median (Interquartile range) | 39.00 (2.11) | 39.00 (2.00) | 38.8 (1.14) | 39.00 (2.00) | 39.00 (2.11) | 0.620 |
| Planed pregnancyNo (%) | Yes | 17 (73.9) | 20 (80) | 15 (65.2) | 22 (84.6) | 74 (76.3) | 0.421 |
| No | 6 (26.1) | 5 (20) | 8 (34.8) | 4 (15.4) | 23 (23.7) |
| Attitude towards childbirth No.(%) | Afraid | 16 (69.6) | 17 (68) | 14 (60.9) | 20 (76.9) | 67 (69.1) | 0.844 |
| Not afraid | 2 (8.7) | 1 (4) | 3 (13) | 2 (7.7) | 8 (8.2) |
| Happy | 5 (21.7) | 7 (28) | 6 (26.1) | 4 (15.4) | 22 (22.7) |
| Perception about labour painNo.(%) | Mild | 0 (0) | 2 (8) | 3 (13) | 1 (3.8) | 6 (6.2) | 0.488 |
| Moderate | 7 (30.4) | 4 (16) | 6 (26.1) | 5 (19.2) | 22 (22.7) |
| Severe | 16 (69.6) | 19 (76) | 14 (60.9) | 20 (76.9) | 69 (71.1) |
| aDilatation at the beginning of study (cm)Median (Interquartile Range) | 3.00 (1) | 3.00 (1) | 3.00 (1) | 3.00 (0) | 3.00 (0.05) | 0.606 |
SD: Standard deviation; The groups were compared using chi-square or Kruskal Wallis test. aThe groups were compared using Kruskal Wallis test.
Outcomes distribution was calculated for those who completed the study that is 19, 20, 21 and 23 women in the four study groups. The duration of Labour was considered as the time interval between TENS device placing (latent phase) to the end of delivery for all participants. Although, group C (active lumbar TENS) had the shortest duration of Labour, there were no significant differences among the groups in terms of Labour duration (p=0.59) [Table/Fig-3].
Outcomes distribution among the study groups.
| Groups variables | Both lumbar and acupuncture points TENS, Passive (Group A) | Passive lumbar TENS- Active acupuncture points TENS (Group B) | Active lumbar TENS- Passive acupuncture points TENS (Group C) | Both lumbar and acupuncture points TENS, Active (Group D) | Total (%)±SD | p-value |
|---|
| Total (No.) | 19 | 20 | 21 | 23 | 83 | - |
| Labour duration (hours) Mean±SD | 11.08±7.05 | 12.4±8.2 | 9.3±5.2 | 12.9±8.5 | 11.4±7.2 | 0.59 |
| bAmount of postpartum Vaginal Bleeding No. (%) | Normal | 17 (89) | 20 (100) | 21 (100) | 23 (100) | 81 (97.6) | 0.363 |
| Abnormal | 2 (10.5) | 0 (0) | 0 (0) | 0 (0) | 2 (2.4) |
| (Mean±SD) First minute Apgar score | 8.79±0.79 | 8.65±1.56 | 8.43±0.87 | 8.87±0.62 | 8.69±1.01 | 0.51 |
| (Mean±SD) Fifth minute Apgar score | 9.74±0.56 | 9.74±0.56 | 9.65±1.35 | 9.62±0.49 | 9.87±0.34 | 0.71 |
| Head circumflex (Mean±SD) | 29.22±5.42 | 31.05±6.15 | 30.63±4.94 | 31.31±6.09 | 30.59±5.66 | *0.028 |
| Newborns’ weight Mean±SD | 3369±342 | 3238±427 | 3286±474 | 3284±537 | 3294±449 | 0.862 |
| Pain score at start pointMedian (Interquartile range) | 6.00 (4) | 5.00 (4) | 5.00 (4) | 5.50 (3) | 0.956 |
| Pain score, one hour after TENS placingMedian (Interquartile range) | 4.50 (2) | 5.50 (2) | 4.00 (3) | 5.00 (2) | 0.538 |
| Pain score at start point of active phaseMedian (Interquartile range) | 5.50 (3) | 6.50 (3) | 6.00 (3) | 8.00 (2) | 0.269 |
| Pain score at the end point of active phaseMedian (Interquartile range) | 8.00 (1) | 8.00 (1) | 8.00 (2) | 8.00 (2) | 0.345 |
*p-value<0.05, SD: Standard deviation; The groups were compared using chi-square or Kruskal Wallis test. bThe groups were compared using chi-square test
Vaginal bleeding was reported in two and birth complications in one subject, both of them were from group A (inactive lumbar and acupuncture points TENS). Only 2.4% of participants reported need for instruments for vaginal delivery, which was in group A and in group C (active lumbar TENS). However, there were no statistically significant differences between the groups (p>0.05).
There were no significant differences among the groups based on the first and fifth minute APGAR scores. The head circumflex of the newborns in group A was lower than the others, and the mean range of this variable was 30.59±5.66 cm among the groups which showed significant difference. The mean weight of newborns was 3294±449 gram. There was no statistically significant difference between groups (p=0.862).
The median pain score at the onset of active phase of Labour was the highest (8/10) in the D group (active lumbar and
acupuncture points TENS) and was the lowest (5.5/10) in group A. However, there was no statistically significant difference in the median of pain intensity between groups at any of the four studied time periods (p>0.05) [Table/Fig-3].
Due to the small number of samples and the failure to establish normal distribution of pain data at four time sections, GEE were used to compare pain score over the four study time points among the studied groups. In the model, the age variable was adjusted as covariate and the autoregressive structure was used as the correlation matrix. Pain variables measured at four time points were modeled as outcome variables with linear method. The results showed that there was no statistically significant difference for pain score over the study periods among the four groups (p-value=0.588) [Table/Fig-4].
Overall, participants’ satisfaction rate for mobility was 88% and the satisfaction rate of using the electrodes was 89.2%. However, there was no statistically significant difference toward satisfaction on mobility (p-value=0.159) and satisfaction of using electrode on body among groups (p-value=0.857). But, there was a statistically significant difference between groups toward tendency to reuse TENS in future labour and group A (inactive lumbar and acupuncture points TENS) (74%) compared to the other three groups (with 93% to 100% satisfaction) [Table/Fig-5].
Final satisfaction outcome among the study groups.
| Groups variables | Both lumbar and acupuncture points TENS, Passive (Group A) | Passive lumbar TENS- Active acupuncture points TENS (Group B) | Active lumbar TENS- Passive acupuncture points TENS (Group C) | Both lumbar and acupuncture points TENS, Active (Group D) | Total No. (%) | p-value |
|---|
| Total (No.) | 19 | 20 | 21 | 23 | 83 | - |
| Mobility restrictions No. (%) | Satisfied | 0 | 1 (5) | 0 | 2 (8.7) | 3 (3.6) | 0.159 |
| No opinion | 4 (21.1) | 0 | 2 (9.5) | 1 (4.3) | 7 (8.4) |
| Unsatisfied | 15 (78.9) | 19 (95) | 19 (90.5) | 20 (87) | 73 (88) |
| Comfort of using electrode on body No. (%) | Satisfied | 1 (5.3) | 2 (10) | 0 | 2 (8.7) | 5 (6) | 0.857 |
| No opinion | 2 (1.5) | 1 (5) | 1 (8.4) | 0 | 4 (4.8) |
| Unsatisfied | 16 (84.2) | 17 (85) | 20 (95.2) | 21 (9.3) | 74 (89.2) |
| Tendency toward TENS in the future No. (%) | Satisfied | 1 (5.3) | 0 | 0 | 0 | 1 (1.2) | 0.046* |
| No opinion | 4 (21.1) | 2 (10) | 0 | 0 | 6 (7.2) |
| Unsatisfied | 14 (73.7) | 18 (90) | 21 (100) | 23 (100) | 76 (91.6) |
*p-value<0.05; The groups were compared using chi-square test
Discussion
The main purpose of this study was to evaluate the effect of concurrent use of TENS on lumbar and acupuncture points on pain relief during Labour. Statistical analysis of VAS scores showed that use of TENS had no effect on pain intensity and severity. Secondary outcome measures included level of satisfaction and maternal-infant outcomes. Although there was no difference between the groups in method, many participants stated that they would like to re-use TENS at the next delivery.
The findings of the present study, similar to the results of some previous studies, indicate that the use of TENS does not change the severity of pain [11,16,17]. There was no statistically significant difference between the four groups, the results of the VAS survey were measured at different times. Along with this result, in the study of Vasegh Rahimparvar F and Seddighian Z a total of 84 nulliparous women were divided into two groups of 42 (lumbar TENS and TENS on Hugo acupuncture points), there was no significant difference in pain intensity between the two groups before and after the intervention, but the process of increasing pain in the acupuncture group was slower from the third hour onwards and had a mild slope [11].
These finding didnot match with other studies [10,13,18-20]. Sanata LS et al., evaluated 46 eligible pregnant women in two groups of 23 lumbar TENS (T10-L1 and S2-S4 points) and controls in the active phase of Labour (Dill=4 cm) in a randomised clinical trial in 2016. Pain intensity at time of study and after 3 min was evaluated with VAS ruler. Statistical analysis showed a significant decrease in pain intensity during Labour. Finally, they reported that lumbar TENS reduced pain in the intervention group [20].
It seems that the reason for the discrepancy with the present study appears to be in the characteristics of the research community, the method of work, and the place of attachment of TENS, as well as women’s attitudes toward childbirth. As most of the participants in the present study imaged the Labour pain to be severe and feared it (71.1% and 69.1%, respectively).
Perception of pain in individuals depends on the severity and duration of uterine contractions, cervical dilatation rate, female physical condition, and also, complex emotional factors such as previous Labour experience, current expectations, and cultural factors [10,21]. In most studies, these effective psychological traits have not been investigated. In the another study, Báez-Suárez A et al., stated that major weakness of their study reported the lack of evaluation patient’s anxiety and psychological variables. They reported that women with pain in the prenatal period may enter the Labour stage with a higher level of physiological arousal anxiety. Increased physiological arousal during childbirth has also been associated with decreased contractions, increased Labour duration and fetal distress, thus increasing the likelihood of intervention. They concluded that many factors influence the incidence of Labour pain. Therefore, it cannot be assumed that pain relief is only due to the use of TENS [19].
In the present study, the mean age of participants was 27.86±5.92. Between four groups were not observed differences in demographic features of the participants. In this study, although the duration of the first stage of Labour was shorter in group C (active lumbar TENS-placebo acupuncture TENS), this difference was not statistically significant (p>0.05). The average of latent phase, active phase of Labour and duration of second phase of Labour were not significantly different between the four groups. This finding is consistent with the results of some studies [10,12,19,20,22].
In the study by Peng T et al., similar to our study, eligible participants were in the latent and early active phase so that the midwife and the researcher had the opportunity to inform the patient about the treatment [22]. The duration of the first to third stages of Labour was not significantly different between the TENS group (Hugo, T12-L1 and S2-S4, PC6) and the control group. However, the latent phase in the TENS group was significantly longer. They identified the main flaws of their study as not being randomised and blinded to research. Randomisation eliminates sampling bias and blinding observer bias [23].
Contrary to the present study, in some studies, the use of TENS reduced the duration of Labour [11,13,18]. Sever N and Akyüz A observed that the duration of Labour in the TENS group was significantly different from the control group. They reported that TENS decreases VAS scores, performance is independent of other variables and has no adverse side effects. This effect of decreasing pain intensity and duration of Labour may affect maternal and neonatal health and lead to satisfaction with the delivery experience [18].
A possible reason for these inconsistencies with the current study may be the differences in routine midwifery care as well as differences in the characteristics of the community under study and the method of work.
The results of present study showed that application of TENS on lumbar and acupuncture point did not affect maternal and neonatal outcomes. Various studies confirm this and so far no neonatal complications have been reported regarding the use of TENS in the Labour [11,13,20,22].
In the present study, although there was no significant difference in pain relief as well as method satisfaction between groups, there was no difference in propensity to re-use. Significant differences were observed between the two groups (p=0.046) and a large number of participants indicated that they would prefer to use TENS again at the next delivery, with 73.7% in the placebo group and 90 to 100% in the active TENS group. This is consistent with many studies [8,10,16,19,20]. Dowswell T et al., compared the group of women receiving TENS with the placebo or control group and found that there was little difference between groups in women’s satisfaction with pain, although nearly two-thirds of the TENS group stated that they would tend to re-use TENS in the next childbirth [8]. This tendency is not due to a decrease in pain but rather to a decrease in unpleasant feelings of pain [16].
Despite the results, keep in mind that this is a mental result that is susceptible to recall bias [19]. There seems to be a tendency to use this method in the socio-cultural conditions of the province and if it provides useful information to pregnant women and encourages it to reduce analgesic consumption and promote effective vaginal delivery promote effective vaginal delivery.
Limitation(s)
The sample size decreased due to attrition at final analysis.
Conclusion(s)
Lumbar or Acupuncture points-TENS had no significant relieving effects on Labour pain among our participants. Although, in our study, there was no significant difference in method satisfaction between groups, a large number of participants would prefer to use TENS again at the next delivery.
SD: Standard deviation; The groups were compared using chi-square or Kruskal Wallis test. aThe groups were compared using Kruskal Wallis test.
*p-value<0.05, SD: Standard deviation; The groups were compared using chi-square or Kruskal Wallis test. bThe groups were compared using chi-square test
*p-value<0.05; The groups were compared using chi-square test