The World Health Organisation (WHO) declared the SARS-CoV-2 (COVID-19) infection a global pandemic on 11th March 2020 [1] which was originally detected in Wuhan, China in late December 2019 [2]. There is no doubt that this is turning out to be the biggest public health challenge of this century so far. Almost no country has been unhurt and many have felt an appalling effect on their health services. With the rising number of cases worldwide, the Government of India imposed a complete lockdown of the whole country on 25th March for three weeks which was later prolonged till 3rd of May 2020 with the general message to stay at home and practice social distancing [3].
Consequent to the aim of developing more COVID-19 care facilities, many hospitals have been declared as dedicated COVID-19 care centres/hospitals while many others have earmarked a major part of their existing infrastructure for the same. This has coupled with the need to increase the workforce in these dedicated areas in view of the expected rise in the number of cases which has led to shifting the residents from various departments to these dedicated centres. Fortunately, however, with the strict lockdown in effect, during these 40 days, there has been a steep fall in the number of Road-Traffic Accidents (RTA) all over the country. Upon removal of RTA as the chief contributor, it becomes fathomable to expect a decrease in the number of emergency trauma. Many other countries have reported similar findings of reduced number of trauma cases wherever there have been similar restrictions on traffic movement [4,5]. Moreover, in lieu of government guidelines and recommendations from the Indian Orthopaedic Association [6] also, the elective surgeries were in majority postponed. This has also caused a paradigm shift in favour of conservative management of many trauma cases that earlier used to be treated preferably by surgery. In the Outpatient Department (OPD) also there has been a sharp decline for most people are avoiding coming to the hospital for the fear of contracting the virus.
While most studies are focussed on big hospitals catering to the city population [4,5,7], our study is based on the effect of lockdown in hospitals of hilly areas. The difference of terrain, the lack of long straight highways replaced by narrow two-laned roads with frequent curves, the variation of occupation and range of household activities etc.; they all contribute to a different epidemiological scenario in the lockdown period in these areas. Ours is a multispecialty state government run hospital located in the hilly areas of Himachal Pradesh state of India. This hospital is the first referral centre of the adjoining 5 districts and caters to a population of more than 2 million people. We retrospectively reviewed this lockdown period from the orthopaedic stand point with focus on the mountainous regions and their demography and the change that has occurred from the same period last year. This will help in knowing the characteristics of orthopaedic practices in these areas and may prove to be a guide in our future schemes of management.
Materials and Methods
The study was done at Shri Lal Bahadur Shastri Government Medical College (and associated district hospital), a level 2 trauma centre in Northern India. Data pertaining to the total lockdown period, that is, from 25th March 2020 to 3rd May 2020 was collected retrospectively, analysed and compared with the same time period last year to decrease the number of confounding factors and bias. Data was collected in such a way as to not reveal the identities of the patients. The study included all patients that were admitted in the emergency trauma bay during the aforementioned time period with a history of trauma (including trivial trauma at home leading to fragility fractures in elderly) and patients with non-traumatic causes of musculoskeletal pain were excluded. Similarly, patients operated in trauma OT were included and those operated in routine OT were excluded. The patients showing in OPD were excluded from the study. However, the total number of OPD patients was noted and compared with last year as the OPD timing was the same as in 2019. The medical record department was the source of data and various parameters like age, gender, mechanism of injury, fracture type, number of emergency admissions, and number of surgeries were recorded and compared. The mechanism of injury was sub-classified into fall, cut injury with sharp object (includes any injury to hands which occurred while working in the kitchen or in the fields), twisting injury to the ankle and knee, assault with blunt object, hit by animal (commonly bull/cow/buffalo), RTA and gunshot injuries (the remaining were classified into others). Patients who were advised telephonically were not included. Data collected was transformed into Microsoft excel for processing statistical analysis.
Statistical Analysis
Statistical testing was conducted with the statistical package for the social science system version SPSS 17.0. Continuous variables were presented as mean±SD or median (IQR) for non-normally distributed data. Categorical variables were expressed as frequencies and percentages.
Results
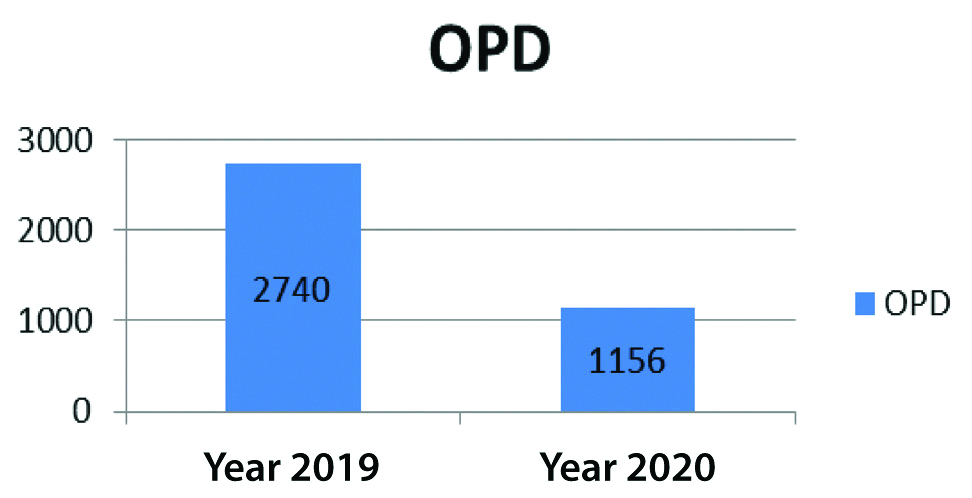
The total number of patients coming in the OPD has decreased from 2740 in 2019 to 1156 in 2020 [Table/Fig-1].
OPD registrations during lockdown period in 2020 vs the same time period in 2019.
Mean age of patients admitted in emergency ward was found to be 41.8±19.7 years in 2020 vs 38.8±20.63 years in 2019. The total number of emergency admissions during the lockdown period (40 days) has remained the similar (164 in 2019 as compared to 169 in 2020) with maximum share borne by the young adults (18-59 years) as seen in [Table/Fig-2].
Age distribution of patients in 2019 and 2020.
| 2019 | 2020 |
|---|
| Age group | Males | Females | Males | Females |
|---|
| <18 years | 21 | 6 | 18 | 14 |
| 18-59 years | 76 | 34 | 60 | 40 |
| >=60 years | 18 | 9 | 18 | 19 |
The broad category of patient age that showed the most change was between ages 18-59 years; with the number of patients seen in emergency decreasing from 59 in 2019 to 34 in 2020. The percentage share of females in trauma patients has increased from 49 (30%) in 2019 to 73 (43%) in 2020.
Surgery
The most common mechanism of injury remained to be fall (fall from height, fall on level and uneven surface) as shown in [Table/Fig-3] in both the years. Falls occurred in a variety of situations, but commonly included fall from tree, falling down the stairs, falling in the bathroom/at home and, in some cases, falling down a hill.
Comparison of common mechanisms of injury.
| Mechanism of injury | Number of patients |
|---|
| 2019 | 2020 |
|---|
| Fall | 94 (57.3%) | 134 (79.3%) |
| RTA | 48 (29.3%) | 7 (4.2%) |
| Injury to hand with sharp object | 4 (2.4%) | 10 (6%) |
| Twisting injury to ankle | 10 (6.2%) | 7 (4.2%) |
| Hit by farm animal (bull/cow/buffalo) | 1 (0.6%) | 5 (3%) |
| Assault with blunt object/gunshot | 0 | 3 (1.8%) |
| Hit by football | 1 (0.6%) | 0 |
| Throwing cricket ball | 1 (0.6%) | 1 (0.5%) |
| Heavy object falling on back/shoulder | 2 (1.2%) | 1 (0.5%) |
| Arm wrestling | 1 (0.6%) | 0 |
| Weightlifting at gym | 1 (0.6%) | 0 |
| Ploughing field | 1 (0.6%) | 1 (0.5%) |
| Total | 164 | 169 |
RTA: Road trafiic aacidents
RTA showed a significant decrease from 48 in 2019 to 7 in 2020. The number of assault cases and gunshot cases were more, 3 and 1, respectively, as compared to zero cases in this category last year.
The total number of trauma surgeries decreased from 62 in 2019 to 51 in 2020. There has been a similar decrease in the percentage of emergency admissions going for surgery. While 62 out of 164 (38%) of patients admitted in emergency went on to be treated surgically in 2019, it reduced to 51 out of 169 (30%) in 2020.
The incidence of some fracture patterns have increased like proximal tibia fractures and hand injuries (more than doubled). On the other hand, some fractures that have shown a decrease in incidence are fracture shaft of femur and fractures around the ankle [Table/Fig-4].
Descriptive table of some of the surgeries that showed change in number in 2020 vs 2019.
| Surgically treated injuries | Number of operated patients |
|---|
| 2019 | 2020 |
|---|
| Total surgeries | 62 | 51 |
| Proximal tibia fractures | 2 | 7 |
| Shaft tibia fracture | 9 | 6 |
| Femur shaft fracture | 10 | 3 |
| Fracture around the ankle | 8 | 4 |
| Hand injuries | 4 | 10 |
| Hip fractures (neck femur, intertrochanteric) | 9 | 9 |
| Humerus fracture (proximal, shaft, supracondylar) | 11 | 7 |
| Olecranonfracture | 2 | 1 |
| Calcaneumfracture | 0 | 1 |
| Fracture both bones forearm/radius/ulna | 5 | 2 |
| Fractures around foot | 2 | 1 |
Notably, the number of operated fragility fractures (fracture neck femur and intertrochanteric fractures in elderly associated with trivial fall) has not changed much during the lockdown period with a total of nine cases operated in both 2020 and 2019 during this period. While the above mentioned specific changes in pattern for operations have been seen, most of the other fracture patterns going on for surgery have not drastically changed. Though, there has been a decrease in the proportion of emergency trauma admission going for surgery; 30% in 2020 in comparison to 38% in 2019. With the fall from height being the chief mechanism of injury, fractures of the spine (anterior wedge compression and burst fractures) are also fairly common in this topography and their prevalence has remained similar in the periods being compared (14 spine fractures in 2020 vs 17 in 2019).
Discussion
Conceivably enough, the number of patients showing up in orthopaedics OPD has decreased; on the contrary, the number of trauma admissions has almost remained the same. This is mainly attributed to the fact that fall is more common than RTA as injury mechanism in our area. Unwittingly, the drastic decline in RTA has not proven to be the same off loader of emergency work as one might expect. This scenario is quite uncommon to be found in this lockdown period taking place worldwide.
Unlike other studies focussing on the lockdown period in their respective areas, there has not been a drastic decline in trauma in our population residing in the hills with farming as the chief occupation [7]. People in our hilly areas have continued to do farm work as it is considered as essential service during this total lockdown also. The people here rear cattle and they frequently climb trees and hills to provide fodder for the animals. This makes them prone to accidental fall from heights. For similar reasons, and while farming on their land, the people end up getting cut injuries with sharp objects. These inadvertent injuries are particularly in their hands, usually with instruments like sickle or axe. This translates to predominantly extensor tendon cut injury in these patients. A plausible reason for increase in hand injuries seems that people are getting more time for the farming activities, coupled with the inexperienced office going individuals joining hands in the same during lockdown period.
The surgical decision making has also leaned towards a more conservative approach in many instances which was also promoted by the Indian Orthopaedic Association in their ‘COVID-19 IOA guidelines’ dated 25th March 2020 [6] and updated on 8th June 2020 [8]. Ergo, the number of surgeries has decreased despite the total number of emergency admissions remaining the same during lockdown. This is also, in part, due to the radical decrease in high-energy trauma of which RTA was the major causative factor.
Interestingly, the fragility fractures have not shown any decline. This substantially points towards the fact that our elder population is at risk for injury even at our homes. These injuries are also hiked by the fact there is lack of realisation of this somewhat preventable disease burden. The lack of awareness among the people in the village, absence of measures taken to prevent the same and an overall under assessment of the disease burden of osteoporosis contributes majorly to this injury pattern. The surgical part is further burdened by the requirement of multidisciplinary management required in this particular age group. Hence, apart from medical management of osteoporosis, we should also focus on preventing falls. Steps like physical activities with exercises focussed on gait and balance rehabilitation, use of hip protectors, walking aids and assessment of home environment to remove obstacles or hazards can prove beneficial. Similar impact of safety-awareness in the field of farming and do-it-yourself activities with conventional instruments can be predicted. A targeted awareness campaign for the same may prove advantageous in our efforts against the COVID-19 pandemic. We need to focus on preventive measures more than before, for more resource allocation in pandemic areas.
This study clearly shows that the orthopaedic trauma load in the hilly areas has not reduced but only its pattern has changed. Consequently, the Orthopaedic department has been running almost the same as before lockdown. Especially, when beds and ventilators from orthopaedics are going to COVID-19 ward and doctors have to exercise extra precautions with few added steps in every procedure, have added more burden. In addition to this, shifting the residents to these dedicated COVID-19 wards has further strained the workforce. Thus, it can be emphasised that orthopaedic trauma is one of the areas that needs constant staffing despite the pandemic.
Limitation(s)
This study is only an estimation of the changes. The sample size in our study is small mainly due to sparse population in the mountainous regions. Apart from that, multicentric studies focussing on similar population cohort with more number of patients will be required to overcome the limitations of our study. The inferences of our study will be better validated if there can be a cumulation of data from hospitals situated in similar geographical areas.
Conclusion(s)
The geography of a place deeply affects the demography of trauma occurring in that area which has been elucidated in this study. It is difficult to arrive at any definitive conclusion based on the data collected during this pandemic time. However, some indicators can definitely be identified from this study and worked upon. This would decrease the burden of trauma in the hilly/mountainous areas and add to the public health. The article also underscores the existing orthopaedic trauma load with continuous inflow of patients even during lockdown period and a requirement to upgrade the same.