Uterine Torsion Masquerading as Abruptio Placentae: Diagnosed on Laparotomy
Niranjan Mayadeo1, Anusha Devalla2
1 Professor, Department of Obstetrics and Gynaecology, Seth GS Medical College, KEM Hospital, Mumbai, Maharastra, India.
2 Junior Resident, Department of Obstetrics and Gynaecology, Seth GS Medical College, KEM Hospital, Mumbai, Maharastra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Anusha Devalla, House No. 15, Sector 9A, Saket Nagar, Bhopal-462024, Madhya Pradesh, India.
E-mail: anushadevalla2@gmail.com
Uterine torsion is a rare, life-threatening and unexpected obstetric emergency. It is almost always diagnosed at caesarean section. Its ill-defined clinical presentation may pose a diagnostic dilemma. Here the authors present a case of 32-year-old, Primigravida, 36 weeks pregnancy with acute abdomen and intrauterine foetal demise. Clinical features resembled Abruptio Placentae. The diagnosis of uterine torsion (180°) was established on laparotomy where the left ovarian ligament was seen on the right side anteriorly. A posterior hysterotomy was done to extract the baby which was followed by detorsion of the uterus. The postoperative period was uneventful.
Abdomen acute, Hysterotomy, Perinatal mortality, Pregnancy, Uterus
Case Report
The patient was 32-year-old Primigravida with married life of five years and spontaneous conception with singleton pregnancy. She had infrequent antenatal visits at a nearby primary hospital; however, the course was uneventful. The patient denied any history of chronic medical or past surgical illness. Suddenly, at 36 weeks of gestation, the patient developed sweating, vomiting followed by acute abdominal pain not relieved with analgesics. She was not able to perceive foetal movements since the onset of pain. Within four hours of the onset of pain, she presented to our Emergency Room with pallor (1+), tachycardia (110/min) and normal blood pressure (100/70 mm Hg) with higher function well-preserved. Abdomen palpation indicated a tonically contracted uterus, foetal parts and presentation couldn’t be identified, foetal heart sounds could not be appreciated. Local and Per Speculum examination revealed no fluid or blood loss. Per Vaginal examination revealed posteriorly placed, long, undilated and uneffaced cervix. Clinical impression of concealed Abruptio Placentae was made. Ultrasonography confirmed intrauterine foetal demise with no retroplacental clots.
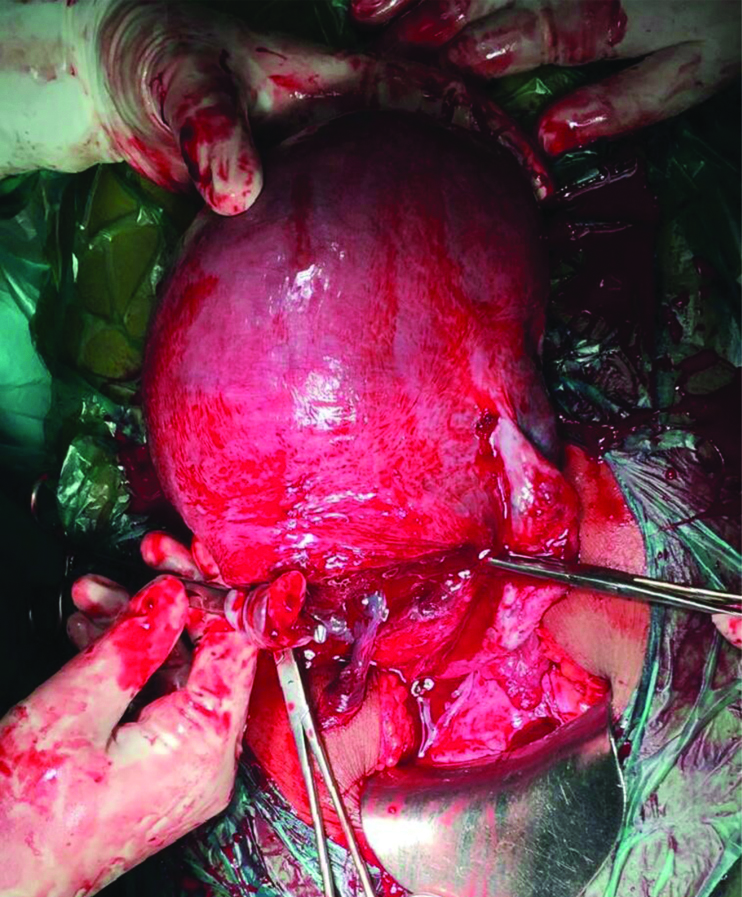
Investigations including complete blood count and coagulation screen were within normal limits. Patient was induced with dinoprostone gel twice at an interval of six hours. The decision for delivery by emergency lower segment caesarean section was taken as there were no significant cervical changes. Patient was taken under spinal anaesthesia and abdomen opened by infraumbilical midline vertical incision. The utero-vesical fold couldn’t be identified. Left-sided round ligament and ovarian ligament twisted around the uterus anteriorly and to the right (180°). A deliberate posterior transverse lower segment incision was given as a result of failure to perform detorsion [Table/Fig-1]. Liquor was found to be clear on amniotomy. A macerated male child of 1.8 kg was delivered. After baby delivery, uterus was exteriorized and findings of uterine torsion were confirmed. Uterus was seen rotated along the long axis nearly 180 degree clockwise and congestion in the fundal region secondary to torsion [Table/Fig-2]. Bilateral ovaries and fallopian tubes were found to be normal. Placenta delivered spontaneously and completely with no retroplacental clots. There was mild postpartum haemorrhage which got controlled with uterotonics. Haemostasis achieved and abdomen closed.
Shows the deliberate posterior low transverse hysterotomy incision with both ovaries seen.
Shows anterior surface of uterus with uterovesical fold after detorsion.

Vital parameters of the patient were stable postoperatively. She was given intravenous antibiotics and oral cabergoline (lactation suppression) and had an uneventful postoperative recovery. She was discharged on 7th postoperative day after suture removal.
Discussion
Uterine torsion is an unexpected obstetric emergency usually diagnosed at the time of caesarean section [1] and may jeopardise maternal and foetal outcomes. Mild dextrorotation (less than 45°) is a common physiological phenomenon. The rotation around the cervical canal (longitudinal) may be from 45° to 180°, although some cases up to 720° have been documented [2]. The vague symptoms and rarity of this condition raises concern for its management [3]. Obstruction of the uterine veins raises pressure in the placental cotyledons leading to abruption and foetal distress. If left uncorrected, it may lead to uterine artery obstruction interrupting the placental perfusion causing intrauterine foetal demise [4].
Cases of uterine torsion have been reported sporadically in the literature, first in 1863, Virchow demonstrated in a human during postmortem examination. In 1876, Labbe described this abnormality for the first time in a living woman [3].
Only about 200 cases have been reported in the last 100 years. Most of the cases in the literature associated with uterine torsion had singleton pregnancies; however, few have occurred in twin pregnancies as well. Uterine torsion in pregnancy can occur in any trimester, age and parity. The cases reported in the literature from India in the last decade (2011-2020) have been tabulated below [Table/Fig-3].
Reports of uterine torsion in pregnancy in the last decade (2011-2020) from India.
| Year | Author | Age of patient | Gravidity | Gestational age | Case details | Diagnostic modality | Intraoperative findings | Treatment | Outcome |
|---|
| 2011 | Deshpande G et al., [4] | 25 years | G1 | 38 weeks | Abdominal pain and uterine tenderness with foetal bradycardia | Intraoperative | 180° torsion | Detorsion of uterus with lower segment caesarean section, fundal fibroid 10×10 cm | Both mother and foetus doing good |
| 2012 | Rasquinha SD et al., [9] | 31 years | G3P2 | 38 weeks | Asymptomatic | Intraoperative | Uterine torsion 180° | Posterior hysterotomy followed by baby delivery and uterine detorsion | Neonate and mother fine |
| 2012 | Gohil A and Patel M [10] | 23 years | G1 | 28 weeks | Acute pain in abdomen and uneasiness | Intraoperative | 180° laevorotation with profuse congestion | Obstetric hysterectomy with baby in-situ | IUD baby, mother well |
| 2013 | Qureshi S et al., [11] | 25 years | G2P1 | 25 weeks | Pain in abdomen, bleeding per vaginum, decreaed foetal movemenets | Intraoperative | 180° uterine torsion with IUFD abruptio placentae | Delibertae posterior hysterotomy; Obstetric hysterectomy (all medical and conservative surgical failed) | Mother died of pulmonary embolism, IUD baby |
| 2013 | Bissa U and Shyam KR [3] | 20 years | G1 | 28 weeks | Pain in abdomen, vomiting, reduced foetal movements. IUFD on UG and subacute intestinal obstruction | Intraoperative | 720° uterine torsion | Detorsion of the unicornuate uterus followed by obstetric hysterectomy; no features of intestinal obstruction | Mother fine |
| 2014 | Sachan R et al., [12] | 27 years | G2P1 | 20 weeks | Acute pain with shock | Intraoperative | 360° axial torsion, massive abruption, large fundal leiomyoma | Detorsion followed by hysterotomy, uterine artery ligation to treat atonic PPH, Blood transfusions | Mother doing well, 16 weeks IUD baby |
| 2015 | Varsha S et al., [13] | 26 years | G5P4L1D2A1 | 36 weeks | Shock and intrauterine foetal demise | Intraoperative | 180° uterine torsion | Detorsion followed by hysterotomy by LSCS, dead foetus delivered; subtotal hysterectomy due to uterus atony | IUD baby, Mother doing well |
| 2015 | Singh P et al., [14] | 28 years | G3P2 | 20 weeks | Pain in abdomen | MRI (preoperative) | Unruptured pregnancy in rudimentary horn with torsion of gravid horn | Resection of the rudimentary horn (left) with the necrosed left adnexa | IUD baby, Mother well |
| 2016 | Ulu I et al., [1] | 37 years | G3P2 | 32 weeks | Severe abdominal pain and mild vaginal bleeding with foetal decelerations | Intraoperative | 180° torsion, subchorionic hematoma, 5×4 cm fibroid | Detorsion failed; posterior hysterotomy | Baby admitted in NICU, discharged in two weeks; mother doing well |
| 2016 | Chundawat RS et al., [15] | 22 years | G2P1 | 28 weeks | Primary abdominal pregnancy with dead foetus and gravid uterus | Intraoperative | Uterine torsion 180° | Detorsion unsucessful followed by posterior hysterotomy, clots 400 mL | Mother fine, baby IUD |
| 2017 | Goswami B and Gautam H [16] | 23 years | G1 | 31 weeks | Pain in abdomen with reduced foetal movements | Intraoperative | 180° torsion of gravid right-sided horn of bicornuate uterus | Excision of that horn and delivery of foetus by posterior hysterotomy | Mother fine, baby IUD |
| 2018 | Kumar N et al., [17] | 16 years | G1 | 17 weeks | No specific complaints | Intraoperative | Non-communicating rudimentary horn torsion 90° and rupture | Rudimentary horn resected with the tube | Mother fine, IUD baby |
| 2018 | Toshniwal R [18] | 27 years | G4P1L1A2 | 20 weeks | Severe abdominal pain with shock | Intraoperative | Torsion of left horn of bicornuate uterus 90° | Posterior hysterotomy and detorsion | IUD baby, Mother well |
| 2018 | Thanappan A [19] | 29 years | G4P1L1A2 | 25 weeks | Acute pain in abdomen with shock | Intraoperative | Uterine torsion 180° | Classical incision on posterior uterine surface, two litre blood clots drained, detorsion | IUD baby, mother fine |
| 2020 | Present study | 32 years | G1 | 36 weeks | Sweating, vomiting, abdominal pain | Ultrasonography (preoperatively) | Uterine torsion 180° | Postero-transverse lower segment incision given. Delivery done. | Macerated baby, mother fine |
IUFD: Intrauterine foetal death; IUD: Intrauterine device; NICU: Neonatal intensive care unit; UG: Ultrasonography; PPH: Post-partum haemorrhage; LSCS: Lower segment ceasarian section
Kopko J et al., recently in 2019 described an incidental finding of uterine torsion of 100 degrees on laparotomy during 2nd trimester, done for appendectomy [5]. Only one maternal death has been observed in the last 50 years [6]. The chances of perinatal mortality secondary to foetal compromise may be as high as 12-18% [2]. Uterine leiomyomas were one of the major risk factor contributing to 31.8%, uterine anomalies were 19.9%, pelvic adhesions 8.4%, ovarian cyst 7%, malpresentations (particularly transverse lie) 4.3%, deformities 2.7% and unknown causes 25.5% [6]. Also uterine torsion with demonstrated foetal bradycardia associated with external cephalic version due to uterine torsion [6].
In this case, there was no apparent cause identified.
The clinical features may cause diagnostic dilemma due to absence of pathognomic symptoms. Common presentations being shock, intestinal obstruction, bleeding per vaginum, labour dystocia. Some may even remain asymptomatic [6]. Associated adnexal torsion requiring bilateral salpingo-oophorectomy has only been reported in 7% of cases [7]. A partial bladder torsion has been reported by Kilicci C associated with 720 degrees of uterine torsion [2]. In some cases, the diagnosis is only made after delivery of the foetus if the repair of posterior hysterotomy incision seems vascular. Radiological investigations may not be much yielding in such emergency situations. Common differential diagnoses includes ectopic pregnancy, placental abruption, intra-abdominal bleeding, torsion of a pelvic tumour, peritonitis, obstructed labour.
Wherever possible, an attempt to detort the uterus should be performed. It has been suggested, vertical hysterotomy/caesarean section should be advised in suspected cases to prevent the vascular or ureteral injury [1]. At term, uterus is derotated and lower segment caesarean section is done. Bilateral plication of utero-sacral ligaments as described by Ulu I et al., to prevent long-term recurrence of uterine torsion still lacks proper validation [1]. Such patients with incision on the posterior wall of the uterus preferably should have a repeat caesarean section in future pregnancy, since the risk of rupture is not known [8]. Hysterectomy should be considered only for greater degree and long-standing cases of torsion.
The correctable factors responsible for the uterine torsion should be dealt with during laparotomy. Difficulty in assessing the uterine scar integrity in the subsequent pregnancy owing to the posterior uterine incision and prior caesarean section being one of the risk factor for torsion, the patient must be advised for a suitable contraception and a close antenatal follow-up in the next pregnancy.
We have revisited various reports published by Indian authors in the literature (last decade) of cases with uterine torsion in pregnancy [Table/Fig-3].
Conclusion(s)
Obstetricians should have this condition in mind while performing caesarean section on a patient with acute abdomen associated with foetal malpresentations, uterine tumours and structural uterine abnormalities. Anatomical landmarks (round ligament) should always be defined prior to uterine incision during a caesarean section, to prevent damage to uterine vessels and to check for any degree of torsion of the pregnant uterus.
IUFD: Intrauterine foetal death; IUD: Intrauterine device; NICU: Neonatal intensive care unit; UG: Ultrasonography; PPH: Post-partum haemorrhage; LSCS: Lower segment ceasarian section
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 23, 2020
Manual Googling: Jul 24, 2020
iThenticate Software: Sep 29, 2020 (13%)
[1]. Ulu I, Guneş MS, Kiran G, Gülşen MS, A rare cause of placental abruption: Uterine torsionJ Clin Diagn Res JCDR 2016 10(1):QD06-07.10.7860/JCDR/2016/16531.707126894131 [Google Scholar] [CrossRef] [PubMed]
[2]. Kilicci C, Sanverdi I, Bostanci E, Abide CY, Eser SK, Uterine torsion of 720 degrees in the third trimester of pregnancy and accompanying bladder torsion: A case reportPan Afr Med J 2018 29:17510.11604/pamj.2018.29.175.1410130050639 [Google Scholar] [CrossRef] [PubMed]
[3]. Bissa U, Shyam KR, Complete Axial Torsion of Gravid Uterus By 720IOSR Journal of Dental and Medical Sciences 2013 7(4):12-15.10.9790/0853-0741215 [Google Scholar] [CrossRef]
[4]. Deshpande G, Kaul R, Manjuladevi P, A case of torsion of gravid uterus caused by leiomyomaCase Reports in Obstetrics and Gynecology 2011 2011(10):20641810.1155/2011/20641822567496 [Google Scholar] [CrossRef] [PubMed]
[5]. Kopko J, Stańczak R, Warzecha D, Wielgos M, Uterine torsion in the second trimester of pregnancyNeuro Endocrinol Lett 2019 39(6):423-26. [Google Scholar]
[6]. Zullino S, Faiola S, Paganelli AM, Ferrazzi E, A Case of Abruptio Placentae due to the Torsion of Gravid UterusCase Rep Obstet Gynecol 2014 2014:80161610.1155/2014/80161625544919 [Google Scholar] [CrossRef] [PubMed]
[7]. Cook KE, Jenkins SM, Pathologic uterine torsion associated with placental abruption, maternal shock, and intrauterine fetal demiseAm J Obstet Gynecol 2005 192(6):2082-83.10.1016/j.ajog.2004.09.00315970905 [Google Scholar] [CrossRef] [PubMed]
[8]. Dua A, Fishwick K, Deverashetty B, Uterine Torsion in Pregnancy: A ReviewThe Internet Journal of Gynecology and Obstetrics 2005 6(1):01-03.10.5580/ce1 [Google Scholar] [CrossRef]
[9]. Rasquinha SD, Rao SB, Rasquinha VC, Aithal V, A twist in the tale- Rare case of uterine torsionInternational Journal of Biomedical Research 2013 3(11):435-36. [Google Scholar]
[10]. Gohil A, Patel M, Torsion of gravid uterus managed by obstetric hysterectomy with the fetus in situJ Obstet Gynecol India 2013 63(4):279-81.10.1007/s13224-012-0188-y24431656 [Google Scholar] [CrossRef] [PubMed]
[11]. Qureshi S, Singh U, Bansal B, Singh N, Torsion of preterm gravid uterus: A case reportInternational Journal of Case Reports and Images 2013 4(7):392-95.10.5348/ijcri-2013-07-339-13 [Google Scholar] [CrossRef]
[12]. Sachan R, Patel ML, Sachan P, Arora A, Complete axial torsion of pregnant uterus with leiomyomaBMJ Case Rep 2014 201410.1136/bcr-2014-20555825193815 [Google Scholar] [CrossRef] [PubMed]
[13]. Varsha S, Devi GP, Bharathi T, Priya VP, Rao SS, Israel YN, A twist in the diagnosis … and the uterus! A case report of third trimester uterine torsionJournal of Clinical and Scientific Research 2015 4(3):240-43.10.15380/2277-5706.JCSR.14.049 [Google Scholar] [CrossRef]
[14]. Singh P, Gupta R, Das B, Bajaj SK, Misra R, Midtrimester spontaneous torsion of unruptured gravid rudimentary horn: Presurgical diagnosis on magnetic resonance imagingJ Obstet Gynaecol Res 2015 41:1478-82.10.1111/jog.1272226013913 [Google Scholar] [CrossRef] [PubMed]
[15]. Chundawat RS, Rastogi R, Tak A, Torsion of gravid horn of bicornuate uterus: A rare case reportInt J Reprod Contracept Obstet Gynecol 2016 5(7):2428-30.10.18203/2320-1770.ijrcog20162141 [Google Scholar] [CrossRef]
[16]. Bivarani Goswami, Himleena Gautam, Torsion of Gravid Horn of Bicornuate Uterus in 3rd Trimester- A Case ReportIOSR Journal of Dental and Medical Sciences 2017 16(9):01-04. [Google Scholar]
[17]. Kumar N, Das V, Pandey A, Agarwal S, Torsion and rupture of a non-communicating rudimentary horn in a 17-week gestation in a 16-year-old girl: Lessons learntBMJ Case Reports 2018 2018:bcr-2017-22207310.1136/bcr-2017-22207329331998 [Google Scholar] [CrossRef] [PubMed]
[18]. Toshniwal R, Uterine Torsion in 20 Weeks of Pregnancy: A Rare Case ReportJ Obstet Gynaecol India 2019 69(1):28-30.10.1007/s13224-018-1145-130956487 [Google Scholar] [CrossRef] [PubMed]
[19]. Thanappan A, Uterine torsion in pregnancy- A rare case reportUniversity Journal of Medicine and Medical Specialities 2018 Vol. 4(3) [Google Scholar]