Malocclusion is the third most common oral health problem and is associated with a number of complications such as gingivitis and periodontitis [1]. Orthodontic treatment with the help of fixed appliances is required for the correction of dental and skeletal discrepancies. Despite its obvious advantages in improving aesthetics, occlusal balance and function, it carries with it some side effects which sometimes occur due to poor oral hygiene maintenance. In these patients, oral hygiene may be more difficult to maintain due to the presence of attachments like brackets, wires, bands, which may lead to plaque accumulation and gingival inflammation [2]. Chang HS et al., reported that orthodontic treatment with fixed appliances induces changes in the oral environment, with an increase in the bacterial concentration mainly Streptococcus mutans and Lactobacilli sp., and concurrent alterations in buffering capacity, pH acidity and salivary flow rate. This may lead to enamel decalcification if preventive measures are not followed to their full capacity [3,4].
Proper maintenance of oral hygiene with fixed orthodontic appliances is difficult to maintain which will result in increased plaque accumulation. This is especially severe in the cervical region between the margins of brackets/buccal tubes/bands and marginal gingiva. Subsequently, it leaves the patient at an increased risk of decalcification and gingivitis [5]. In addition, insertion of fixed appliances favours frequent retention of fermentable carbohydrates which would increase the acid formation at a low pH level and thereby facilitate growth of Streptococcus mutans and Lactobacilli sp., at the plaque retentive sites [6]. During orthodontic treatment, there is an increase in the number of Streptococcus mutans and Lactobacilli sp., [7]. These bacteria may cause demineralisation or decalcification of dental enamel which leads to the subsequent development of White Spot Lesions (WSLs) adjacent to the orthodontic brackets. Without proper intervention, progression of these lesions can lead to dental caries.
The WSLs are defined as “subsurface enamel porosity from carious demineralisation [8]. They appear as a milky opacity when located on a smooth surface” [8]. The overall prevalence of WSLs has been reported with much variation in literature ranging between 2-97% [9]. The frequency of WSLs in orthodontically treated patients in decreasing order are maxillary lateral incisors, mandibular canines, mandibular first premolars, mandibular molars, mandibular second premolars, maxillary canine, maxillary first premolars, and central incisors [10,11]. No significant differences were found in the incidence and prevalence of WSLs between the right and left sides of the maxilla and mandible and also between males and females [10,12,13].
The WSLs begin to appear around the brackets within one month of bracket placement and these lesions are commonly seen on the buccal surfaces of teeth especially in the gingival region [14]. Patients undergoing orthodontic treatment showed a continuous increase in the levels of Streptococcus mutans and Lactobacilli sp., levels but Streptococcus mutans showed significant difference only in the first month of treatment and marginal difference during retraction stages whereas lactobacilli counts were different in all treatment stages with diverse levels of significance [15]. Prevalence of oral microbial flora especially during the retraction stages (orthodontic space closure with friction mechanics) can be worsened by the use of attachments such as elastic chains, loops and springs.
The WSLs around fixed orthodontic appliances are a major challenge during and after fixed orthodontic treatment because it affects the dental and facial aesthetics and predisposes the teeth to dental caries. Hence, knowledge of the potential risk factors that predisposes teeth to lesions is important. Therefore, the aim of this pilot study was to estimate the prevalence of oral microbial flora during orthodontic space closure which may in turn help to determine the risk of development of WSLs and in turn lead to the development of appropriate preventive measures to control the demineralisation process before the lesions progress further.
Materials and Methods
This cross-sectional study pilot study was carried out during the month of December 2019 for a period of two weeks in the Department of Orthodontics at Saveetha Dental College under the supervision of two blinded observers. Ethical clearance for the study protocol was obtained from the Institutional Review Board (IHEC/SDC-ORTHO-1501/20/168) to conduct this research. It is a general rule that the sample size of the pilot study may be 10% of targeted population in the final research [16]. So, 8 patients undergoing treatment in the Orthodontic Department and at the stage of orthodontic space closure were randomly selected. They were within the age group of 18-25 years and gender was not considered and friction biomechanics was used to close the space. The sample consisted of four males and four females.
Inclusion criteria: Patients with full complement of permanent dentition, Skeletal class I with Angles class I malocclusion with moderate crowding (Little’s irregularity index, 4-6 mm), extraction of first premolar as a part of orthodontic treatment, patients undergoing orthodontic space closure with friction mechanics with the use of E-chain (Ormco) 1 month after start of space closure, pre-adjusted standard edgewise (Gemini 3M Unitek) appliance metal brackets, retraction by 19×25 SS wires (Captain Ortho) used for retraction were included in this study.
Exclusion criteria: Patients with a history of orthodontic treatment, patients with history of habits like drinking alcohol, and tobacco smoking, patients diagnosed with fluorosis, gingival and periodontal problems, those under antibiotics and oral mouth rinses past 3 months and patients with any other systemic disorders and nutritional deficiencies were excluded from the study.
Informed consent was obtained from participants after explaining about the study.
Collection of Specimens
Samples were collected twice, first at 6-8 months from the start of treatment and again 1-2 months after the start of the space closure step. All the samples were collected one hour after eating. All patients were asked to rinse the oral cavity with water to remove any residual food debris. All four quadrants were isolated with cotton rolls to avoid saliva contamination before collecting the sample. Plaque samples were collected in aseptic conditions, with the help of sterile cotton swabs moistened with sterile saline from the cervical region (labial/buccal surface) around the orthodontic brackets from the regions of maxillary lateral incisor, maxillary premolar, mandibular canine and mandibular premolar in the 1st, 2nd, 3rd and 4th quadrants, respectively. Since, it is a cross-sectional study, the sample was collected only once from each site after the start of space closure. Thus, 4 samples were collected from each patient. The handle of sterile tube was held without any contamination at the time of use and it was transferred immediately into the sterile tube containing 2 mL of Brain Heart Infusion (BHI) broth medium and it was delivered to the Microbiology laboratory [Table/Fig-1].
Collection of specimens in a transport vial with broth from different sites on the oral cavity from the orthodontic patients.

Estimation of Microbial Counts
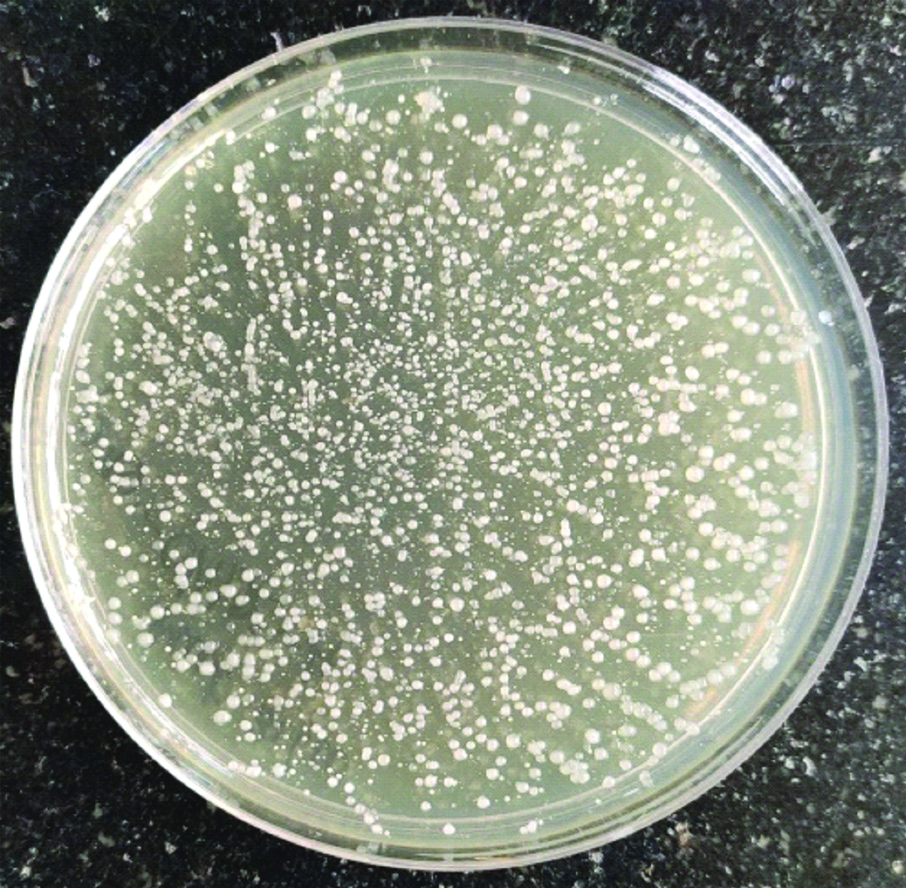
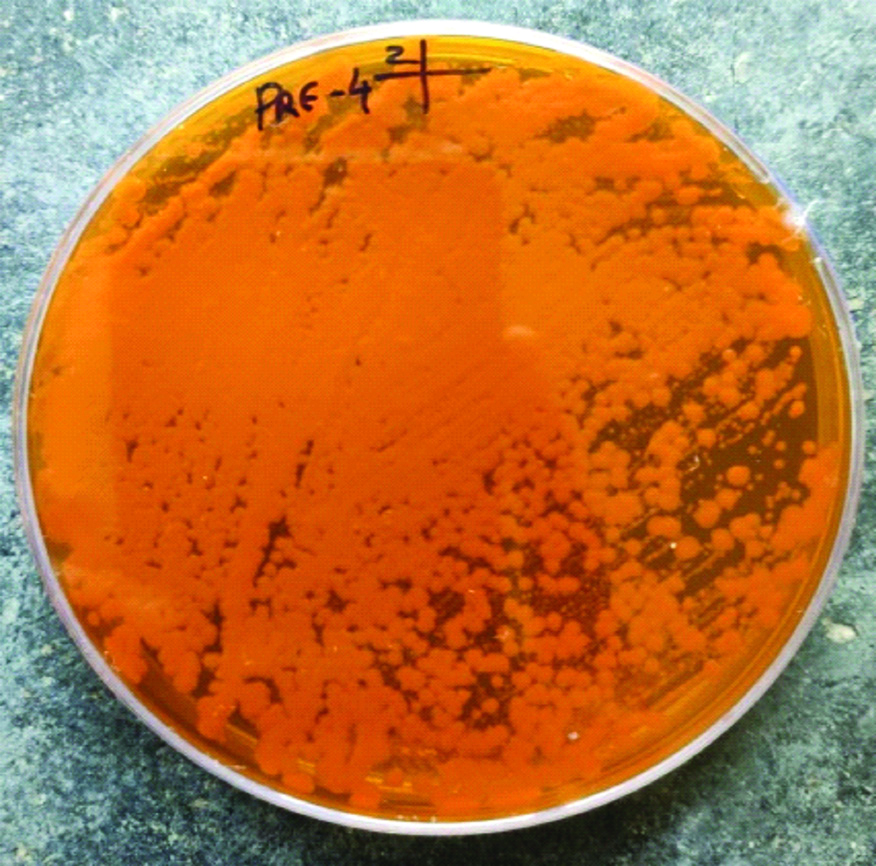
The swab was inoculated in the tube containing 2 mL of BHI broth for bacterial isolation and identification and was incubated at 37°C for 2 hours [17]. Serial dilutions were not performed since the count of bacteria was done by using mere mathematical calculation from 10 μL. After 2 hours, 10 μL of the broth was inoculated onto freshly prepared Mutans Sanguis agar (HiMedia Laboratories) for Streptococcus mutans isolation and MRS agar (HiMedia Laboratories) for Lactobacillus isolation. Other bacteria such as Actinomyces, Prevotella, Neisseria, and Veillonella usually harbour the tooth surfaces. Since these are present at small concentrations and do not contribute to demineralisation, they were not evaluated in this study [18]. The culture plates were then incubated at 37°C, for 24 hours for Streptococcus mutans [19] and 48 hours for Lactobacillus, respectively [20]. Bacterial growth was identified and evaluated directly as visible colonies in their respective agar plates. S. mutans colonies were identified as rough yellow heaped colonies with white frosty glass appearance [19] whereas Lactobacillus were identified as irregular, creamy white coloured, circular, low convex colonies with entire margin [21]. Gram staining was performed and S.mutans was observed as gram positive cocci in chains and Lactobacillus as gram positive bacilli in chains. Biochemical characterisation assay test catalase test was performed to confirm the bacterial strain, which identified both as catalase negative and were calibrated manually by two independent assessors with the help of a colony counter (Manti Lab) [22] and were measured in terms of colony forming units (cfu/mL) [Table/Fig-2,3]. Kappa statistics was performed which revealed an inter-examiner reliability of 0.91.
Estimation of colony counts from Mutans Sanguis (MS) agar to determine the colony forming units at different sites.
Estimation of colony counts from deMan, Rogosa and Sharpe (MRS) agar to determine the colony forming units at different sites.
Statistical Analysis
Descriptive statistics were used for data summarisation. An independent sample t-test was done to determine the mean and standard deviation between S. mutans and Lactobacilli at the four evaluated sites. One-way ANOVA and Post-Hoc Tukey HSD test was done to estimate the prevalence of the microorganisms at the different sites. The statistical analysis was carried out by using SPSS Software (IBM Corp, Version 13) and the level of significance was fixed at p≤0.05.
Results
A total of 8 patients were included in the study. Out of these 4 were males and 4 were females. Mean and SD of age in Males and Females were 22±2.16 years and 22.25±1.70 years, respectively [Table/Fig-4].
Distribution of study subjects according to gender and age.
| Gender | Males | Females |
|---|
| Number of patients | 4 | 4 |
| Mean Age±SD (Years) | 22±2.16 | 22.25±1.70 |
The microbiological data is presented in [Table/Fig-5,6].
ANOVA shows Streptococcus mutans showed highly significant difference compared to lactobacillus (p<0.001).
| Bacteria studied | Sites | N | Mean (×102) cfu/mL | Std. deviation (×102) cfu/mL | Significant difference |
|---|
| Streptococcus | 12 | 8 | 7.07 | 1.68 | <0.001 |
| 33 | 8 | 6.32 | 1.41 |
| 25 | 8 | 2.65 | 1.39 |
| 45 | 8 | 3.15 | 2.01 |
| Total | 32 | 4.8 | 2.50 |
| Lactobacilllus | 12 | 8 | 25.12 | 4.04 | 0.146 |
| 33 | 8 | 27.86 | 9.41 |
| 25 | 8 | 21.66 | 11.40 |
| 45 | 8 | 17.75 | 8.96 |
| Total | 32 | 23.1 | 9.27 |
One-way ANOVA with Post-hoc Tukey HSD analysis to estimate the prevalence of microbial flora at various sites p<0.05.
| Dependent variable sites | Mean difference (I-J) | Significance | 95% Confidence interval | Significant difference |
|---|
| Lower bound | Upper bound |
|---|
| Streptococcus | 12 | 33 | 0.75 | 0.800 | -1.49 | 2.99 | <0.001 |
| 25 | 4.42 | <0.001 | 2.17 | 6.67 |
| 45 | 3.92 | <0.001 | 1.67 | 6.17 |
| 33 | 12 | -0.75 | 0.800 | -2.99 | 1.49 |
| 25 | 3.67 | 0.001 | 1.42 | 5.92 |
| 45 | 3.17 | 0.003 | 0.92 | 5.42 |
| 25 | 12 | -4.42 | <0.001 | -6.67 | -2.17 |
| 33 | -3.67 | 0.001 | -5.92 | -1.42 |
| 45 | -0.50 | 0.929 | -2.74 | 1.74 |
| 45 | 12 | -3.92 | <0.001 | -6.17 | -1.67 |
| 33 | -3.17 | 0.003 | -5.42 | -0.92 |
| 25 | 0.50 | 0.929 | -1.74 | 2.74 |
| Lactobacilllus | 12 | 33 | -2.73 | 0.926 | -14.86 | 9.38 | 0.146 |
| 25 | 3.46 | 0.863 | -8.66 | 15.58 |
| 45 | 7.37 | 0.363 | -4.74 | 19.49 |
| 33 | 12 | 2.73 | 0.926 | -9.38 | 14.86 |
| 25 | 6.20 | 0.512 | -5.92 | 18.32 |
| 45 | 10.11 | 0.128 | -2.01 | 22.23 |
| 25 | 12 | -3.46 | 0.863 | -15.58 | 8.66 |
| 33 | -6.20 | 0.512 | -18.32 | 5.92 |
| 45 | 3.91 | 0.815 | -8.21 | 16.03 |
| 45 | 12 | -7.37 | 0.363 | -19.49 | 4.74 |
| 33 | -10.11 | 0.128 | -22.23 | 2.01 |
| 25 | -3.91 | 0.815 | -16.03 | 8.21 |
Out of 8 patients, collected microbiological data showed that Streptococcus mutans was highly significant compared to Lactobacillus acidophilus (p<0.001) indicating that streptococcus is the main cause for the development of WSLs. It is interesting to note that the number of colonies of lactobacillus was greater than the colonies of streptococcus mutans during the stage of retraction. This may be due to the change in the local oral environment during the retraction phase. However, further elaborate studies need to be conducted to confirm the validity of this finding [Table/Fig-5].
From [Table/Fig-6], bacterial count of Streptococcus mutans was highly significant among the different sites (p-value <0.001) mainly in the maxillary incisor (12) region and also in mandibular canine (33) region and the difference in colony forming units of Lactobacillus acidophilus was not found to be statistically significant among the different sites.
Discussion
The present investigation was performed as a pilot study and showed an increase in the prevalence of microbial flora that occurred in the oral environment during orthodontic space closure approximately 6-8 months since placement of fixed appliances on permanent dentition. Although there are few studies that report the prevalence of microbial flora during and after orthodontic treatment, the microbial flora that may occur specifically during orthodontic space closure has not been evaluated [4,7,23]. The reason behind this was that among the three stages of orthodontic treatment, the second stage (space closure) is one of the most challenging and crucial aspects for orthodontists due to the large number of biomechanical options available for space closure and also due to the variation in the period of treatment time. The longer duration of treatment might be responsible for development of WSLs. In this study, plaque collection was performed only on specific sites such as, maxillary lateral incisor, maxillary premolar, mandibular canine and mandibular premolar in the 1st, 2nd, 3rd and 4th quadrants, respectively, because these sites are more prone for the development of WSLs [10,11]. No articles were found regarding the effect of right or left-handedness on oral microbial flora in orthodontic patients and it is not feasible to collect samples from all the teeth.
Orthodontic patients have an increased risk of carious lesions due to higher retention of dental plaque and impaired oral hygiene. Colonisation of aciduric bacteria can cause demineralisation of enamel which leads to the development of WSLs and decay [24]. There is a significant difference in the number of Streptococcus mutans and Lactobacilli sp., between patients who are undergoing and who are not undergoing orthodontic treatment [25].
Streptococcus mutans is the main cause of dental decay and various lactobacilli are associated with progression of the lesion. Demineralisation of enamel is visible after 3 months of active orthodontic treatment due to increase in the levels of S.mutans and Lactobacillus which ferment the carbohydrates and create a low pH environment induced by acid production [3,26]. Excess composite around the bracket base and presence of a distinct gap at the composite-enamel interface is a critical site for plaque accumulation making it necessary to sample the plaque from the tooth surface [27]. Among the different samples collected for assessment such as saliva, tongue, mirror, and plaque, Streptococcus mutans and Lactobacillus were consistently higher in plaque than in other sampling techniques and plaque samples have consistently been used to evaluate site-specific Streptococcus mutans levels to predict caries risk on specific tooth surfaces [28]. Dental plaque collection and samples of stimulated whole saliva showed similar results in Streptococcus mutans counts. However, the most appropriate method for detection of lactobacilli is the stimulated whole saliva method [29]. Based on this study [29], lack of significance in testing Lactobacillus acidophilus in the present study may be due to the use of plaque samples for determination of Lactobacillus acidophilus count. Therefore, measuring Lactobacillus acidophilus from stimulated saliva may be considered in future studies. The Plaque sample method shows a significant difference in Streptococcus mutans count compared to the use of saliva method [30]. Among different sampling approaches, cotton swabbing is a low-cost and practical method, validating the use of the swab as the preferred oral sampling approach [31]. Hence, in the present study, samples were collected from dental plaque by cotton swabbing method.
Patients undergoing orthodontic treatment showed a continuous increase in the levels of Lactobacilli but not in the levels of Streptococcus mutans. Streptococcus mutans showed significant difference only in the first month of treatment and marginal difference at retraction stages but lactobacilli counts were different in all stages with diverse levels of significance [15]. This study evaluated microbial content after the placement of elastic chain and loop for space closure.
There are conflicting reports in literature regarding the distribution of WSLs. Some studies showed that the most commonly affected tooth was maxillary lateral incisor [9-11]. Other studies showed that first molars were the most commonly affected teeth [24]. The present study also showed that maxillary lateral incisor was the most commonly affected tooth followed by mandibular canine due to the significant increase in the streptococcus mutans in that region compared to the other sites. Gender distribution was also conflicting with no significant difference between the genders in incidence of WSLs in some studies [12,13] in contrast to other studies in which gender differences were present [10]. Frequency of WSLs was not significantly different among the age groups in some studies [13] in contrast to other studies which showed a significant difference among the age groups [11,12]. Good oral hygiene is the most important prophylactic measure to prevent WSLs in fixed orthodontic patients. In addition prophylaxis with topical fluorides and others including Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP) complexes, antiseptics, probiotics, polyols, sealants, lasers, tooth bleaching, resin infiltration, and microabrasion have also been recommended [32]. Recommended usage of fluoride and casein supplements in ameliorating WSLs during and after fixed orthodontic treatment is significantly effective in the reduction of demineralisation spots. This will be possible by using materials containing fluoride and/or casein phosphopeptide-amorphous calcium phosphate to manage and prevent the WSLs [33].
Two studies showed that the prevalence of WSL in patients undergoing orthodontic treatment as early as 6 months (38% and 40%, respectively), increased with longer treatment duration at 12 months (46% and 43%, respectively) [8,24]. Orthodontic treatment time appears to have a significant impact on the development of WSLs in some studies [9,11,13] in contrast to other findings in which there was no significant impact of treatment time on the development of WSLs [12]. Orthodontic treatment with clear aligner therapy showed a low incidence of WSLs [13].
Significant increase in the levels of Streptococcus mutans during orthodontic treatment reported in this study is similar to those published in existing literature [23,34]. Use of self-ligating brackets, properly contoured bands not impinging into the gingival sulcus, Glass Ionomer Cement (GIC) for banding in addition to the mechanical methods of plaque control such as brushing, flossing, etc., chemical methods such as mouthwashes, varnishes, etc., should be employed to reduce the plaque accumulation [18]. Indirect bonding protocol and super slick elastomeric ligatures should be used for reduction in plaque accumulation around the brackets which will aid in decreasing the onset of white spots during the orthodontic treatment [35].
Limitation(s)
Since the present study was a pilot study, a control group was not considered. The study being a preliminary one requires further experimental validation with a higher sample size. Some aciduric flora such as Actinomyces spp., and Candida albicans which also have an effect on the demineralisation of teeth [36] have not been evaluated in this study.
Conclusion(s)
This study showed that during orthodontic space closure, bacterial count of Streptococcus mutans showed a statistically significant difference among the different sites (maxillary lateral incisor, mandibular canines, maxillary and mandibular premolars) with the highest value in the maxillary lateral incisor region followed by mandibular canine region.
The incidence of Lactobacillus acidophilus did not show any statistically significant difference among the various sites. Considerable amount of plaque accumulation occurs during the orthodontic space closure procedures, which may increase the onset of WSLs hence, more attention should be given to oral hygiene maintenance by using plaque control methods. The results from this study would be used as a guide to formulate a more standardised research protocol for future researches.